Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Medical BillingDocument5 pagesMedical BillingBenziger Fernandez100% (7)
- Asepsis Antisepsis and Skin PreparationDocument6 pagesAsepsis Antisepsis and Skin PreparationDavid Tritono Di BallastrossNo ratings yet
- Management of HypertensionDocument64 pagesManagement of HypertensionAnonymous h0DxuJTNo ratings yet
- Pemeriksaan Refleks BulbocavernosusDocument2 pagesPemeriksaan Refleks BulbocavernosusAnonymous h0DxuJTNo ratings yet
- M 371Document14 pagesM 371Anonymous h0DxuJTNo ratings yet
- 712 PDFDocument74 pages712 PDFAnonymous h0DxuJTNo ratings yet
- PR MRDocument6 pagesPR MRAnonymous h0DxuJTNo ratings yet
- Influence of Nutritional Status On Clinical Outcomes in Critically Ill ChildrenDocument5 pagesInfluence of Nutritional Status On Clinical Outcomes in Critically Ill ChildrenAnonymous h0DxuJTNo ratings yet
- Hemoptysis: Contribution of The Computed Tomography (CT) : CC CBGDocument23 pagesHemoptysis: Contribution of The Computed Tomography (CT) : CC CBGAnonymous h0DxuJTNo ratings yet
- Feeding of The Critically Ill Child-Dr. Waceke KombeDocument22 pagesFeeding of The Critically Ill Child-Dr. Waceke KombeAnonymous h0DxuJTNo ratings yet
- Casa Er 2015Document12 pagesCasa Er 2015Anonymous h0DxuJTNo ratings yet
- Nutritional Status of Children in Critical Condition at Admission To Pediatric Intensive Care UnitsDocument6 pagesNutritional Status of Children in Critical Condition at Admission To Pediatric Intensive Care UnitsAnonymous h0DxuJTNo ratings yet
- HHS Public AccessDocument21 pagesHHS Public AccessAnonymous h0DxuJTNo ratings yet
- PXX 123Document8 pagesPXX 123Anonymous h0DxuJTNo ratings yet
- Upper Airway ManeuversDocument9 pagesUpper Airway ManeuversAnonymous h0DxuJTNo ratings yet
- Hard Ell 2017Document4 pagesHard Ell 2017Anonymous h0DxuJTNo ratings yet
- Impact of Mobile Use Amongst Children in Rural Area of Marathwada Region of Maharashtra, IndiaDocument5 pagesImpact of Mobile Use Amongst Children in Rural Area of Marathwada Region of Maharashtra, IndiaAnonymous h0DxuJTNo ratings yet
- Airway Management in TraumaDocument9 pagesAirway Management in TraumaAnonymous h0DxuJTNo ratings yet
- Internet Scientific PublicationsDocument12 pagesInternet Scientific PublicationsAnonymous h0DxuJTNo ratings yet
- OET Writing Module 1 (Updated)Document14 pagesOET Writing Module 1 (Updated)Leila100% (1)
- Occupational Hazards in DentistryDocument7 pagesOccupational Hazards in DentistryTejas KulkarniNo ratings yet
- Legal Aspects and EthicsDocument18 pagesLegal Aspects and EthicsBuyung Tegar AribowoNo ratings yet
- Department of Education: Annual Gender and Development (Gad) Plan and BudgetDocument6 pagesDepartment of Education: Annual Gender and Development (Gad) Plan and BudgetJaymar Padayao0% (1)
- Appendix 2 Self-Medicaition Study QuestionnaireDocument8 pagesAppendix 2 Self-Medicaition Study Questionnairetherese BNo ratings yet
- Mortality Review - ppt2Document27 pagesMortality Review - ppt2mohamad ashmuniNo ratings yet
- Asthma Devices PDFDocument28 pagesAsthma Devices PDFSiti ChodijahNo ratings yet
- Home Visit OrientationDocument29 pagesHome Visit OrientationMay Chelle ErazoNo ratings yet
- Colegio Gonzalo Jimenez Navas: Individual WorkDocument3 pagesColegio Gonzalo Jimenez Navas: Individual WorkNicolas Cárdenas maldonadoNo ratings yet
- The Periodontal Index: A. L. Russell ExaminingDocument7 pagesThe Periodontal Index: A. L. Russell ExaminingVivek PatelNo ratings yet
- Informed Consent On DocumentationDocument3 pagesInformed Consent On DocumentationanurajoneNo ratings yet
- Adult Airway DayDocument7 pagesAdult Airway DayDes Dwiputra EffendyNo ratings yet
- BCU Edit Tomat PDFDocument16 pagesBCU Edit Tomat PDFmuhammad adamNo ratings yet
- Persuasion Speech OutlineDocument4 pagesPersuasion Speech OutlineHarris1501No ratings yet
- The Guide To Medicare Preventive ServicesDocument283 pagesThe Guide To Medicare Preventive ServicesharrellmbNo ratings yet
- Mini Mental State Examination Cognitive FIM Instrument and The Loewenstein Occupational Therapy Cognitive Assessment Relation To Functional Outco PDFDocument4 pagesMini Mental State Examination Cognitive FIM Instrument and The Loewenstein Occupational Therapy Cognitive Assessment Relation To Functional Outco PDFDamira HalilovicNo ratings yet
- RewariDocument1 pageRewariShivNo ratings yet
- Level of Disease PreventionDocument16 pagesLevel of Disease Preventionenam professorNo ratings yet
- Cortical Neuroplasticity in Hearing LossDocument21 pagesCortical Neuroplasticity in Hearing LossElena RojasNo ratings yet
- 2021-EO New Localized Guidelines November GCQDocument6 pages2021-EO New Localized Guidelines November GCQDennis CosmodNo ratings yet
- NCM 106 Course SyllabusDocument9 pagesNCM 106 Course SyllabusEmmyNo ratings yet
- Essential Workers and QuarantineDocument3 pagesEssential Workers and QuarantineWWMTNo ratings yet
- PDF-bnys 2 2010 DecDocument5 pagesPDF-bnys 2 2010 DecmaguitcoolNo ratings yet
- IDB Assessment Tool (Questionnaire)Document7 pagesIDB Assessment Tool (Questionnaire)Somcio, Denise Grazelle Anne P.No ratings yet
- Solution Manual For Olds Maternal Newborn Nursing Womens Health Across The Lifespan 9 e 9th Edition 0133073777Document36 pagesSolution Manual For Olds Maternal Newborn Nursing Womens Health Across The Lifespan 9 e 9th Edition 0133073777pourlieustationcc2w7s100% (48)
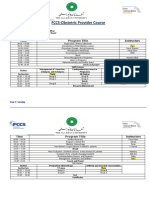
- FCCS-Obstetric Provider Course: Time Program Title InstructorsDocument2 pagesFCCS-Obstetric Provider Course: Time Program Title InstructorsSamina AyazNo ratings yet
- Policy Relating To Health Safety and Welfare of EmployeesDocument13 pagesPolicy Relating To Health Safety and Welfare of Employeeslucky javellanaNo ratings yet
- 5-Aminolevulinic Acid Photodynamic Therapy For Condyloma Acuminatum of Urethral MeatusDocument19 pages5-Aminolevulinic Acid Photodynamic Therapy For Condyloma Acuminatum of Urethral MeatusRiefka Ananda ZulfaNo ratings yet