
TP 04 04 304 PDF
TP 04 04 304 PDF
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- PB Assist +: Probiotic Defense FormulaDocument4 pagesPB Assist +: Probiotic Defense FormulaEduardo TakemuraNo ratings yet
- Anatomy and Physiology of Temporomandibular JointDocument16 pagesAnatomy and Physiology of Temporomandibular JointAsfoor gake1No ratings yet
- Sensory .N Motor. N: Trigeminal .N Cervical PlexusDocument3 pagesSensory .N Motor. N: Trigeminal .N Cervical PlexusAsfoor gake1No ratings yet
- DNA SequencingDocument21 pagesDNA SequencingAsfoor gake1100% (1)
- DNA StructureDocument23 pagesDNA StructureAsfoor gake1No ratings yet
- Periodontal Ligament: Teeth Maxillary MandibularDocument7 pagesPeriodontal Ligament: Teeth Maxillary MandibularAsfoor gake1No ratings yet
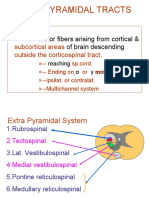
- Extrapyramidal Tracts: Motor Fibers Arising From Cortical & of Brain DescendingDocument21 pagesExtrapyramidal Tracts: Motor Fibers Arising From Cortical & of Brain DescendingAsfoor gake1No ratings yet
- Fluorescence in Situ Hybridization: Presented By: Shreya Lodh Under The Guidance Of: Dr.T.R.Sharma Dr.R.K.ChahotaDocument20 pagesFluorescence in Situ Hybridization: Presented By: Shreya Lodh Under The Guidance Of: Dr.T.R.Sharma Dr.R.K.ChahotaAsfoor gake1No ratings yet
- 7th Lecture Physics of Cardiovascular System1Document12 pages7th Lecture Physics of Cardiovascular System1Asfoor gake1No ratings yet
- 4th Lecture Physics of Diagnostic X-RayDocument43 pages4th Lecture Physics of Diagnostic X-RayAsfoor gake1No ratings yet
- HyperammonemiaDocument10 pagesHyperammonemiaAsfoor gake1No ratings yet
- Trigeminal Nerve AnatomyDocument56 pagesTrigeminal Nerve AnatomyAsfoor gake1No ratings yet
- Phenylketonuria: Abbas A. A. Shawka Medical Student 2 GradeDocument24 pagesPhenylketonuria: Abbas A. A. Shawka Medical Student 2 GradeAsfoor gake1No ratings yet
- First Week of Human DevelopmentDocument81 pagesFirst Week of Human DevelopmentAsfoor gake10% (1)
- Phenylketonur IA: Done byDocument27 pagesPhenylketonur IA: Done byAsfoor gake1100% (1)
- Phenylketonuria: DR Rohini C SaneDocument37 pagesPhenylketonuria: DR Rohini C SaneAsfoor gake1No ratings yet
- Biochemistry Lec 3Document3 pagesBiochemistry Lec 3Asfoor gake1No ratings yet
- L. 10 The Oral CavityDocument79 pagesL. 10 The Oral CavityAsfoor gake1No ratings yet
- About Microsoft Word:: PlanDocument26 pagesAbout Microsoft Word:: PlanAsfoor gake1No ratings yet
- Fungus VSL - Emotional Story DissectionDocument65 pagesFungus VSL - Emotional Story DissectionmarceloqNo ratings yet
- Amul ProjectDocument56 pagesAmul Projectabhishek61850% (2)
- Selection of A Chicken Lactobacillus Strain With Probiotic Properties and Its Application in Poultry ProductionDocument268 pagesSelection of A Chicken Lactobacillus Strain With Probiotic Properties and Its Application in Poultry ProductionMuhamad Akhmal HakimNo ratings yet
- 10 BV PDFDocument13 pages10 BV PDFYossy VesriNo ratings yet
- Anatomia de Lesiones en Pesuñas de Cerdos-Breeding FocusDocument6 pagesAnatomia de Lesiones en Pesuñas de Cerdos-Breeding FocusAlejandro CalderónNo ratings yet
- Microbial Ecology of Fermented Rege Tables and Non-Alcoholic Drinks and Current Knowledge On Their Impact On Human HealthDocument39 pagesMicrobial Ecology of Fermented Rege Tables and Non-Alcoholic Drinks and Current Knowledge On Their Impact On Human HealthNayeli MartinezNo ratings yet
- Tugas Susu Dr. SandyDocument10 pagesTugas Susu Dr. SandyAlisa Sharen AssyfaNo ratings yet
- Probiotics Prebiotics BIOL325Document4 pagesProbiotics Prebiotics BIOL325Adil ParvaizNo ratings yet
- Food Micro PPT 5 Sep Training QalhDocument38 pagesFood Micro PPT 5 Sep Training Qalhnuria mukarani100% (1)
- Sourdough BreadDocument14 pagesSourdough BreadBanupriyaNo ratings yet
- Application of Biotechnology in Dairy and Food Processing 2003Document213 pagesApplication of Biotechnology in Dairy and Food Processing 2003Rohit SinghNo ratings yet
- Fermented Products of India and Its Implication A ReviewDocument9 pagesFermented Products of India and Its Implication A ReviewvikashvermaiitkgpNo ratings yet
- Enterogermina: DO NOT INJECT or Administer in Any Other WayDocument3 pagesEnterogermina: DO NOT INJECT or Administer in Any Other WayHack NologyNo ratings yet
- Natural RemediesDocument25 pagesNatural Remediesbalasuk100% (3)
- Probiotics Downloadable PDFDocument2 pagesProbiotics Downloadable PDFGreg WrightNo ratings yet
- Thesis: Compiled By: Athaya Ramadhani Janitra NIM 3920187181454Document47 pagesThesis: Compiled By: Athaya Ramadhani Janitra NIM 3920187181454alfinmuhafidhahNo ratings yet
- Characterization and Identification of Lactobacillus Acidophilus Using Biolog Rapid Identification SystemDocument5 pagesCharacterization and Identification of Lactobacillus Acidophilus Using Biolog Rapid Identification Systemarina31No ratings yet
- Goodbelly: Using Statistics To Justify The Marketing ExpenseDocument8 pagesGoodbelly: Using Statistics To Justify The Marketing ExpenseAlejo Mendez OsorioNo ratings yet
- Foods 13 00111Document15 pagesFoods 13 00111Edward Josehp Uriarte SánchezNo ratings yet
- Sample - Global Dairy Market (2020 - 2025) - Mordor IntelligenceDocument35 pagesSample - Global Dairy Market (2020 - 2025) - Mordor Intelligencehaluk tukelNo ratings yet
- 2011 Nestle Purina Veterinary Symposium On Companion Animal MedicineDocument30 pages2011 Nestle Purina Veterinary Symposium On Companion Animal Medicineguadasampaio100% (1)
- Traditional Starter Cultures in CheesethDocument88 pagesTraditional Starter Cultures in CheesethCAPRINOS BAJA CALIFORNIA SUR, MEXICO100% (1)
- Probiotics Benefits, Foods and SupplementsDocument11 pagesProbiotics Benefits, Foods and SupplementsKishore KumarNo ratings yet
- Helicobacter Pylori (H. Pylori) Infection FactsDocument38 pagesHelicobacter Pylori (H. Pylori) Infection FactsPieter SteenkampNo ratings yet
- Telaah Kritis Jurnal Dengan Critical Appraisal WorksheetDocument7 pagesTelaah Kritis Jurnal Dengan Critical Appraisal WorksheetalfathulnurkarismaNo ratings yet
- Safety Studies of Bacillus Coagulans Unique Is-2 in Rats: Morphological, Biochemical and Clinical EvaluationsDocument6 pagesSafety Studies of Bacillus Coagulans Unique Is-2 in Rats: Morphological, Biochemical and Clinical EvaluationsJohanaNo ratings yet
- 1 The Definition of ProbioticsDocument11 pages1 The Definition of ProbioticsMohd Shuaib KhanNo ratings yet
- Treating The Top Five Chronic Conditions Chris KresserDocument85 pagesTreating The Top Five Chronic Conditions Chris Kresserlamag100% (1)
- Association Between Diarrhea Duration and Severity and Probiotic Efficacy in Children With Acute GastroenteritisDocument19 pagesAssociation Between Diarrhea Duration and Severity and Probiotic Efficacy in Children With Acute Gastroenteritis0019 Azhar WicaksonoNo ratings yet






















































































Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- PB Assist +: Probiotic Defense FormulaDocument4 pagesPB Assist +: Probiotic Defense FormulaEduardo TakemuraNo ratings yet
- Anatomy and Physiology of Temporomandibular JointDocument16 pagesAnatomy and Physiology of Temporomandibular JointAsfoor gake1No ratings yet
- Sensory .N Motor. N: Trigeminal .N Cervical PlexusDocument3 pagesSensory .N Motor. N: Trigeminal .N Cervical PlexusAsfoor gake1No ratings yet
- DNA SequencingDocument21 pagesDNA SequencingAsfoor gake1100% (1)
- DNA StructureDocument23 pagesDNA StructureAsfoor gake1No ratings yet
- Periodontal Ligament: Teeth Maxillary MandibularDocument7 pagesPeriodontal Ligament: Teeth Maxillary MandibularAsfoor gake1No ratings yet
- Extrapyramidal Tracts: Motor Fibers Arising From Cortical & of Brain DescendingDocument21 pagesExtrapyramidal Tracts: Motor Fibers Arising From Cortical & of Brain DescendingAsfoor gake1No ratings yet
- Fluorescence in Situ Hybridization: Presented By: Shreya Lodh Under The Guidance Of: Dr.T.R.Sharma Dr.R.K.ChahotaDocument20 pagesFluorescence in Situ Hybridization: Presented By: Shreya Lodh Under The Guidance Of: Dr.T.R.Sharma Dr.R.K.ChahotaAsfoor gake1No ratings yet
- 7th Lecture Physics of Cardiovascular System1Document12 pages7th Lecture Physics of Cardiovascular System1Asfoor gake1No ratings yet
- 4th Lecture Physics of Diagnostic X-RayDocument43 pages4th Lecture Physics of Diagnostic X-RayAsfoor gake1No ratings yet
- HyperammonemiaDocument10 pagesHyperammonemiaAsfoor gake1No ratings yet
- Trigeminal Nerve AnatomyDocument56 pagesTrigeminal Nerve AnatomyAsfoor gake1No ratings yet
- Phenylketonuria: Abbas A. A. Shawka Medical Student 2 GradeDocument24 pagesPhenylketonuria: Abbas A. A. Shawka Medical Student 2 GradeAsfoor gake1No ratings yet
- First Week of Human DevelopmentDocument81 pagesFirst Week of Human DevelopmentAsfoor gake10% (1)
- Phenylketonur IA: Done byDocument27 pagesPhenylketonur IA: Done byAsfoor gake1100% (1)
- Phenylketonuria: DR Rohini C SaneDocument37 pagesPhenylketonuria: DR Rohini C SaneAsfoor gake1No ratings yet
- Biochemistry Lec 3Document3 pagesBiochemistry Lec 3Asfoor gake1No ratings yet
- L. 10 The Oral CavityDocument79 pagesL. 10 The Oral CavityAsfoor gake1No ratings yet
- About Microsoft Word:: PlanDocument26 pagesAbout Microsoft Word:: PlanAsfoor gake1No ratings yet
- Fungus VSL - Emotional Story DissectionDocument65 pagesFungus VSL - Emotional Story DissectionmarceloqNo ratings yet
- Amul ProjectDocument56 pagesAmul Projectabhishek61850% (2)
- Selection of A Chicken Lactobacillus Strain With Probiotic Properties and Its Application in Poultry ProductionDocument268 pagesSelection of A Chicken Lactobacillus Strain With Probiotic Properties and Its Application in Poultry ProductionMuhamad Akhmal HakimNo ratings yet
- 10 BV PDFDocument13 pages10 BV PDFYossy VesriNo ratings yet
- Anatomia de Lesiones en Pesuñas de Cerdos-Breeding FocusDocument6 pagesAnatomia de Lesiones en Pesuñas de Cerdos-Breeding FocusAlejandro CalderónNo ratings yet
- Microbial Ecology of Fermented Rege Tables and Non-Alcoholic Drinks and Current Knowledge On Their Impact On Human HealthDocument39 pagesMicrobial Ecology of Fermented Rege Tables and Non-Alcoholic Drinks and Current Knowledge On Their Impact On Human HealthNayeli MartinezNo ratings yet
- Tugas Susu Dr. SandyDocument10 pagesTugas Susu Dr. SandyAlisa Sharen AssyfaNo ratings yet
- Probiotics Prebiotics BIOL325Document4 pagesProbiotics Prebiotics BIOL325Adil ParvaizNo ratings yet
- Food Micro PPT 5 Sep Training QalhDocument38 pagesFood Micro PPT 5 Sep Training Qalhnuria mukarani100% (1)
- Sourdough BreadDocument14 pagesSourdough BreadBanupriyaNo ratings yet
- Application of Biotechnology in Dairy and Food Processing 2003Document213 pagesApplication of Biotechnology in Dairy and Food Processing 2003Rohit SinghNo ratings yet
- Fermented Products of India and Its Implication A ReviewDocument9 pagesFermented Products of India and Its Implication A ReviewvikashvermaiitkgpNo ratings yet
- Enterogermina: DO NOT INJECT or Administer in Any Other WayDocument3 pagesEnterogermina: DO NOT INJECT or Administer in Any Other WayHack NologyNo ratings yet
- Natural RemediesDocument25 pagesNatural Remediesbalasuk100% (3)
- Probiotics Downloadable PDFDocument2 pagesProbiotics Downloadable PDFGreg WrightNo ratings yet
- Thesis: Compiled By: Athaya Ramadhani Janitra NIM 3920187181454Document47 pagesThesis: Compiled By: Athaya Ramadhani Janitra NIM 3920187181454alfinmuhafidhahNo ratings yet
- Characterization and Identification of Lactobacillus Acidophilus Using Biolog Rapid Identification SystemDocument5 pagesCharacterization and Identification of Lactobacillus Acidophilus Using Biolog Rapid Identification Systemarina31No ratings yet
- Goodbelly: Using Statistics To Justify The Marketing ExpenseDocument8 pagesGoodbelly: Using Statistics To Justify The Marketing ExpenseAlejo Mendez OsorioNo ratings yet
- Foods 13 00111Document15 pagesFoods 13 00111Edward Josehp Uriarte SánchezNo ratings yet
- Sample - Global Dairy Market (2020 - 2025) - Mordor IntelligenceDocument35 pagesSample - Global Dairy Market (2020 - 2025) - Mordor Intelligencehaluk tukelNo ratings yet
- 2011 Nestle Purina Veterinary Symposium On Companion Animal MedicineDocument30 pages2011 Nestle Purina Veterinary Symposium On Companion Animal Medicineguadasampaio100% (1)
- Traditional Starter Cultures in CheesethDocument88 pagesTraditional Starter Cultures in CheesethCAPRINOS BAJA CALIFORNIA SUR, MEXICO100% (1)
- Probiotics Benefits, Foods and SupplementsDocument11 pagesProbiotics Benefits, Foods and SupplementsKishore KumarNo ratings yet
- Helicobacter Pylori (H. Pylori) Infection FactsDocument38 pagesHelicobacter Pylori (H. Pylori) Infection FactsPieter SteenkampNo ratings yet
- Telaah Kritis Jurnal Dengan Critical Appraisal WorksheetDocument7 pagesTelaah Kritis Jurnal Dengan Critical Appraisal WorksheetalfathulnurkarismaNo ratings yet
- Safety Studies of Bacillus Coagulans Unique Is-2 in Rats: Morphological, Biochemical and Clinical EvaluationsDocument6 pagesSafety Studies of Bacillus Coagulans Unique Is-2 in Rats: Morphological, Biochemical and Clinical EvaluationsJohanaNo ratings yet
- 1 The Definition of ProbioticsDocument11 pages1 The Definition of ProbioticsMohd Shuaib KhanNo ratings yet
- Treating The Top Five Chronic Conditions Chris KresserDocument85 pagesTreating The Top Five Chronic Conditions Chris Kresserlamag100% (1)
- Association Between Diarrhea Duration and Severity and Probiotic Efficacy in Children With Acute GastroenteritisDocument19 pagesAssociation Between Diarrhea Duration and Severity and Probiotic Efficacy in Children With Acute Gastroenteritis0019 Azhar WicaksonoNo ratings yet