Download as pdf or txt
You might also like
- Cardiac Arrest QuestionsDocument2 pagesCardiac Arrest Questionsmine251580% (5)
- Jama Murthy 2020 It 200008Document2 pagesJama Murthy 2020 It 200008jorgeNo ratings yet
- Mja2 50598Document10 pagesMja2 50598Andi Astrid AmaliaNo ratings yet
- Consensus Statement: Safe Airway Society Principles of Airway Management and Tracheal Intubation Specific To The COVID-19 Adult Patient GroupDocument10 pagesConsensus Statement: Safe Airway Society Principles of Airway Management and Tracheal Intubation Specific To The COVID-19 Adult Patient GroupMeska AmeliaNo ratings yet
- Severe Covid-19: Clinical PracticeDocument10 pagesSevere Covid-19: Clinical Practicemarcelocarvalhoteacher2373No ratings yet
- Rizal JournalDocument2 pagesRizal Journallindzy.amurao01No ratings yet
- Supporting The Health Care Workforce During The COVID-19 Global EpidemicDocument2 pagesSupporting The Health Care Workforce During The COVID-19 Global EpidemicDema AlsouqiNo ratings yet
- Clinical PracticeDocument10 pagesClinical PracticeCarlos AlvarezNo ratings yet
- Severe Covid-19Document10 pagesSevere Covid-19Gabriela ArvelaezNo ratings yet
- NEJM Severe COVIDDocument10 pagesNEJM Severe COVIDErick Roa GandicaNo ratings yet
- Severe Covid-19: Clinical PracticeDocument10 pagesSevere Covid-19: Clinical PracticejoelNo ratings yet
- HCQ Study JamaDocument7 pagesHCQ Study Jamathe kingfishNo ratings yet
- Reabilitação Após Doença Crítica de CovidDocument5 pagesReabilitação Após Doença Crítica de CovidCristina BoaventuraNo ratings yet
- 6MINUTEWALKTESTABERTODocument5 pages6MINUTEWALKTESTABERTOpv7j8j6q5rNo ratings yet
- Novel Coronavirus 2019 (2019-Ncov) Infection: Part Ii - Respiratory Support in The Pediatric Intensive Care Unit in Resource-Limited SettingsDocument8 pagesNovel Coronavirus 2019 (2019-Ncov) Infection: Part Ii - Respiratory Support in The Pediatric Intensive Care Unit in Resource-Limited Settingsdiah Bayu siswantiNo ratings yet
- 2389-Article Text-9837-6-10-20211201Document9 pages2389-Article Text-9837-6-10-20211201Sumendhe Hayuning SukmaraniNo ratings yet
- Covid 19 Hospital AcquiredDocument2 pagesCovid 19 Hospital AcquiredeliassssssNo ratings yet
- The Journal For Nurse PractitionersDocument5 pagesThe Journal For Nurse Practitionersagstri lestariNo ratings yet
- High Incidence of Barotrauma in Patients With Severe Coronavirus Disease 2019Document9 pagesHigh Incidence of Barotrauma in Patients With Severe Coronavirus Disease 2019AMBUJ KUMAR SONINo ratings yet
- Respiratory Support For Adult Patients With COVID-19Document7 pagesRespiratory Support For Adult Patients With COVID-19SekarNo ratings yet
- Evolution of Acute Respiratory Distress Syndrome IDocument14 pagesEvolution of Acute Respiratory Distress Syndrome InalgatronNo ratings yet
- Pneumonia and VAP PreventionDocument35 pagesPneumonia and VAP Preventionhendro harahapNo ratings yet
- Invasive and Non-Invasive Ventilation in Patients With COVID-19Document6 pagesInvasive and Non-Invasive Ventilation in Patients With COVID-19Augusto ManoelNo ratings yet
- Who 2019 Ncov Ipc Ppe Use 2020.3 EngDocument28 pagesWho 2019 Ncov Ipc Ppe Use 2020.3 EngKumanan1304No ratings yet
- Tx. COVID 19 en UCIDocument6 pagesTx. COVID 19 en UCIVictor Augusto Ávila HernándezNo ratings yet
- 1 s2.0 S0025712522000955 MainDocument12 pages1 s2.0 S0025712522000955 MainMonika Diaz KristyanindaNo ratings yet
- COVID-19: A Quick Look at Aspects of Critical CareDocument5 pagesCOVID-19: A Quick Look at Aspects of Critical CareJbarrianNo ratings yet
- Pi Is 0025619620311873Document5 pagesPi Is 0025619620311873Achmad RyandaNo ratings yet
- Dr. Hendri - Early Warning System & PPEDocument106 pagesDr. Hendri - Early Warning System & PPEViniFortunataNo ratings yet
- CCJM 87a ccc033 FullDocument4 pagesCCJM 87a ccc033 FullKamar Operasi Hermina BogorNo ratings yet
- 394 Full PDFDocument20 pages394 Full PDFHaltiNo ratings yet
- COVID-19 Disease Invasive VentilationDocument8 pagesCOVID-19 Disease Invasive VentilationfikriafisNo ratings yet
- Jamaotolaryngology Givi 2020 SC 200001Document6 pagesJamaotolaryngology Givi 2020 SC 200001dina ayu SeptianiNo ratings yet
- 10 1111@anae 15054 PDFDocument33 pages10 1111@anae 15054 PDFJuliana Rodriguez MariñoNo ratings yet
- Global Guidance For Surgical Care During The COVID-19 PandemicDocument7 pagesGlobal Guidance For Surgical Care During The COVID-19 PandemicSergio Losada AmayaNo ratings yet
- Recommendations For Prehospital Airway Management in Patients With Suspected COVID-19 InfectionDocument5 pagesRecommendations For Prehospital Airway Management in Patients With Suspected COVID-19 InfectionConnor StephensonNo ratings yet
- Internal Medicine Journal - 2009 - Ferguson - Preventing Healthcare Associated Infection Risks Healthcare Systems andDocument8 pagesInternal Medicine Journal - 2009 - Ferguson - Preventing Healthcare Associated Infection Risks Healthcare Systems andHamid ShahNo ratings yet
- Neurologic Emergencies During The Coronavirus DiseDocument17 pagesNeurologic Emergencies During The Coronavirus DiseCristina CalzadaNo ratings yet
- Final Seminar Manuscript Group 5 To PrintDocument30 pagesFinal Seminar Manuscript Group 5 To PrintGuenevere DamasinNo ratings yet
- How COVID-19 Has Changed The Management of Glomerular DiseasesDocument4 pagesHow COVID-19 Has Changed The Management of Glomerular DiseasesLouie MercadoNo ratings yet
- BMJ 2021 065871.fullDocument24 pagesBMJ 2021 065871.fullEfen YtNo ratings yet
- How COVID-19 Has Changed The Management of Glomerular DiseasesDocument4 pagesHow COVID-19 Has Changed The Management of Glomerular DiseasesHendri WahyudiNo ratings yet
- Covid 19 ProgramDocument12 pagesCovid 19 ProgramBAGUIO CATSNo ratings yet
- Novel Coronavirus 2019 (2019-Ncov) Infection: Part Ii - Respiratory Support in The Pediatric Intensive Care Unit in Resource-Limited SettingsDocument9 pagesNovel Coronavirus 2019 (2019-Ncov) Infection: Part Ii - Respiratory Support in The Pediatric Intensive Care Unit in Resource-Limited SettingsHanni HarahapNo ratings yet
- Recognition and Prevention of Nosocomial Pneumonia in The ICU and Infection Control in Mechanical VentilationDocument11 pagesRecognition and Prevention of Nosocomial Pneumonia in The ICU and Infection Control in Mechanical Ventilationandres felipe burgos granadosNo ratings yet
- Nac 2017Document18 pagesNac 2017Nataly CortesNo ratings yet
- The Central Role of Clinical Nutrition in COVID-19 Patients During and After Hospitalization in Intensive Care UnitDocument5 pagesThe Central Role of Clinical Nutrition in COVID-19 Patients During and After Hospitalization in Intensive Care UnitReaz MorshedNo ratings yet
- COVID en ObstetriciaDocument9 pagesCOVID en Obstetriciaantonio123valenciaNo ratings yet
- Guias JamaDocument2 pagesGuias JamaEliana TorresNo ratings yet
- The Interplay Between Coagulation and Inflammation Pathways in COVID-19-Associated Respiratory Failure: A Narrative ReviewDocument17 pagesThe Interplay Between Coagulation and Inflammation Pathways in COVID-19-Associated Respiratory Failure: A Narrative ReviewAlanNo ratings yet
- High Flow Nasal Cannula For Acute Respiratory Distress Syndrome Due To Covid 19Document5 pagesHigh Flow Nasal Cannula For Acute Respiratory Distress Syndrome Due To Covid 19Cesar C SNo ratings yet
- De Pascale 2012Document9 pagesDe Pascale 2012HellcroZNo ratings yet
- Healthcare Associated Pneumonia - Dr. Christian A. Johannes, SP - an.KICDocument30 pagesHealthcare Associated Pneumonia - Dr. Christian A. Johannes, SP - an.KICvenyNo ratings yet
- Jurding KLP A Anes 3Document18 pagesJurding KLP A Anes 3mreza26No ratings yet
- Pi Is 0099176720304220Document10 pagesPi Is 0099176720304220yasintameganabilaNo ratings yet
- 30794136: Aspiration Pneumonia in Older AdultsDocument7 pages30794136: Aspiration Pneumonia in Older AdultsNilson Morales CordobaNo ratings yet
- Nos InfecDocument6 pagesNos InfecMimi ElagoriNo ratings yet
- PIIS0003999320302951Document3 pagesPIIS0003999320302951Adiel CarrascoNo ratings yet
- 7.qiu2020 Article IntensiveCareDuringTheCoronaviDocument3 pages7.qiu2020 Article IntensiveCareDuringTheCoronaviM. TERESA TORNEL MARINNo ratings yet
- Whooping Cough Unveiled: From Pathogenesis to Promising TherapiesFrom EverandWhooping Cough Unveiled: From Pathogenesis to Promising TherapiesNo ratings yet
- 21 AdisaDocument6 pages21 AdisaTri UtariNo ratings yet
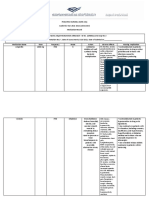
- Medication Sheet 2021-2022Document3 pagesMedication Sheet 2021-2022Attekah MohammedNo ratings yet
- Blood GroupsDocument5 pagesBlood GroupsMalik IrfanNo ratings yet
- ICD-10 CM All Diagnosis and Trigger Codes - Revised 9-17-2015Document6,507 pagesICD-10 CM All Diagnosis and Trigger Codes - Revised 9-17-2015Puskesmas MakaleNo ratings yet
- Appendix 4 - Example Birth HistoryDocument2 pagesAppendix 4 - Example Birth HistorySriMathi Kasi Malini ArmugamNo ratings yet
- Neurologist Doctor Near MeDocument2 pagesNeurologist Doctor Near MesnaayuNo ratings yet
- Final Course in The WardDocument4 pagesFinal Course in The WardMichael Boado100% (1)
- Ccare Pro Les Waye FeatureDocument10 pagesCcare Pro Les Waye Featureapi-604638740No ratings yet
- Oxygenation Problem Notes and Nursing InterventionsDocument7 pagesOxygenation Problem Notes and Nursing InterventionsAnna TaylorNo ratings yet
- Book-Based: Pathophysiology of Allergic RhinitisDocument2 pagesBook-Based: Pathophysiology of Allergic RhinitisJeraldine Corpuz PascualNo ratings yet
- APC-Associated Polyposis Conditions - GeneReviews® - NCBI BookshelfDocument38 pagesAPC-Associated Polyposis Conditions - GeneReviews® - NCBI BookshelfKostantinos EmmNo ratings yet
- Health CertificateDocument3 pagesHealth CertificateĐĂNG TRỊNH HẢINo ratings yet
- Compendium Dermatologie RomanaDocument207 pagesCompendium Dermatologie RomanaRusu Bianca Elena67% (3)
- 03 Muscle and Neuromuscular Junction Disorders PDFDocument325 pages03 Muscle and Neuromuscular Junction Disorders PDFOTTO JESUS VEGA VEGA100% (2)
- AIDS Is Real and It's in Our Church: HIV/AIDS and The Church in AfricaDocument327 pagesAIDS Is Real and It's in Our Church: HIV/AIDS and The Church in AfricaMike BlythNo ratings yet
- MCQs PulmonologyDocument2 pagesMCQs PulmonologySadia Batool86% (7)
- Children: Asthma's Impact On The NationDocument4 pagesChildren: Asthma's Impact On The NationNycoNo ratings yet
- Dr. Rasul Dr. Orencia: Surgery ER Orthopedics Ward OR ENT OPD Ophthalmology ClerkDocument12 pagesDr. Rasul Dr. Orencia: Surgery ER Orthopedics Ward OR ENT OPD Ophthalmology ClerkApmc Schwartz100% (1)
- Medsurg AdhdDocument3 pagesMedsurg AdhdminniprkNo ratings yet
- Tuberculosis of The Spine An OverviewDocument6 pagesTuberculosis of The Spine An OverviewSattvik SpineNo ratings yet
- 1.who Shall Be Considered As Having Community-Acquired Pneumonia?Document6 pages1.who Shall Be Considered As Having Community-Acquired Pneumonia?Kristine Jade OdtujanNo ratings yet
- Disorders of Speech & EmotionDocument10 pagesDisorders of Speech & EmotionBoris ThingbaijamNo ratings yet
- Stress Hyperglycemia: Anand MosesDocument4 pagesStress Hyperglycemia: Anand MosesDaeng Arya01No ratings yet
- Pediatric Traumatic Brain Injury: Characteristic Features, Diagnosis, and ManagementDocument12 pagesPediatric Traumatic Brain Injury: Characteristic Features, Diagnosis, and ManagementsylvetriNo ratings yet
- Intrathecal Injection (LP) ENGDocument1 pageIntrathecal Injection (LP) ENGAlina RadescuNo ratings yet
- (Impetigo) : Erbil Polythecnic University Soran Technical Insititute Nuraing Department First StageDocument14 pages(Impetigo) : Erbil Polythecnic University Soran Technical Insititute Nuraing Department First StageKubra ĖdrisNo ratings yet
- NSTP 2 Midterm ReviewerDocument6 pagesNSTP 2 Midterm ReviewerTrexy NorialNo ratings yet
- Fluids and Electrolytes IV FluidsDocument1 pageFluids and Electrolytes IV Fluidsnursing concept mapsNo ratings yet
- Thyroid DiseaseDocument17 pagesThyroid DiseaseCharlz ZipaganNo ratings yet