Download as pdf or txt
You might also like
- The Sage Handbook of Organizational WellbeingDocument22 pagesThe Sage Handbook of Organizational WellbeingSamungateNo ratings yet
- Where There Is No PsychiatristDocument335 pagesWhere There Is No PsychiatristIFANI NURUL ISLAMY100% (1)
- Assessment Resources - BAMDocument4 pagesAssessment Resources - BAMandrew_carlquistNo ratings yet
- Final ThesisDocument120 pagesFinal ThesisSingh SoniyaNo ratings yet
- Psychosocial Assessment Template Social WorkDocument7 pagesPsychosocial Assessment Template Social WorkFar SultanNo ratings yet
- Domains of Psychiatric RehabilitationDocument3 pagesDomains of Psychiatric Rehabilitationsivagiri.pNo ratings yet
- Toward A Neuroscience of AttachmentDocument34 pagesToward A Neuroscience of AttachmentIoana UngurianuNo ratings yet
- CAGE QuestionnaireDocument1 pageCAGE QuestionnaireSaya MenangNo ratings yet
- Love MelancholiaDocument13 pagesLove MelancholiaalfonsougarteNo ratings yet
- Un Policy Brief-Covid and Mental Health FinalDocument17 pagesUn Policy Brief-Covid and Mental Health FinalDenise Vilas Boas100% (1)
- Bioethics in Psychiatry AnDocument18 pagesBioethics in Psychiatry Aneric faasNo ratings yet
- Psych Abnormal Child Psychology - 6th Edition (2015) - 301-350Document50 pagesPsych Abnormal Child Psychology - 6th Edition (2015) - 301-350tin_ally9059No ratings yet
- Argumentative Essay. Gift or A CurseDocument13 pagesArgumentative Essay. Gift or A Cursejsus22No ratings yet
- Durkheim, Emile. What Is A Social Fact. The Rules of The Sociological Method.Document2 pagesDurkheim, Emile. What Is A Social Fact. The Rules of The Sociological Method.musicma1n1No ratings yet
- Chapter Outline: Personality Is The Unique Pattern of Enduring Thoughts, Feelings and Actions That Characterize ADocument11 pagesChapter Outline: Personality Is The Unique Pattern of Enduring Thoughts, Feelings and Actions That Characterize AViola HastingsNo ratings yet
- Gold Essay CollectionDocument47 pagesGold Essay CollectionОйбек ХамраевNo ratings yet
- Behavioural AddictionsDocument15 pagesBehavioural AddictionsnishthasainiNo ratings yet
- Gender Inequality & Its Impact On Mental HealthDocument22 pagesGender Inequality & Its Impact On Mental Healthbanipreet kaurNo ratings yet
- ABHISHEK GANGULI - NTCC - IMPACT OF STUDENTS MENTAL HEALTHDocument36 pagesABHISHEK GANGULI - NTCC - IMPACT OF STUDENTS MENTAL HEALTHPriyanshu KumarNo ratings yet
- Child Psychiatric EmergenciesDocument8 pagesChild Psychiatric EmergenciesDanitza YhovannaNo ratings yet
- Internet AddictionDocument13 pagesInternet AddictionGerardo DamianNo ratings yet
- ICD 10 and DSM 5 Diffrence DDKFDDocument2 pagesICD 10 and DSM 5 Diffrence DDKFDEmraan Malik100% (1)
- Internet Addiction Test: Dr. Kimberly S. YoungDocument11 pagesInternet Addiction Test: Dr. Kimberly S. Youngvinita singh0% (1)
- Get Psyched! Volume 1, Fall 2011Document29 pagesGet Psyched! Volume 1, Fall 2011Danlan WhitworthNo ratings yet
- JACOBSON & GREENLEY - What Is Recovery A Conceptual Model and ExplicationDocument4 pagesJACOBSON & GREENLEY - What Is Recovery A Conceptual Model and ExplicationemaildegeorgeNo ratings yet
- National Health PolicyDocument20 pagesNational Health PolicySiyona BansodeNo ratings yet
- Experience of Caregiving and Coping in Caregivers of Patients With Alzheimer's DementiaDocument30 pagesExperience of Caregiving and Coping in Caregivers of Patients With Alzheimer's DementiaDrSankalp DixitNo ratings yet
- Male Counselling in The Context of Intimate Partner Violence Paper Draft 1 KRRP 10292014Document12 pagesMale Counselling in The Context of Intimate Partner Violence Paper Draft 1 KRRP 10292014Rina WidarsihNo ratings yet
- Religiosity and Mental Health - A Critical Reevaluation and Meta-ADocument10 pagesReligiosity and Mental Health - A Critical Reevaluation and Meta-ALorena AntonoviciNo ratings yet
- Self Measures For Marital Satisfaction MARITAL ADJUSTMENT TESTDocument4 pagesSelf Measures For Marital Satisfaction MARITAL ADJUSTMENT TESTGropeneanu Ana MNo ratings yet
- Community Mental Health in India PDFDocument2 pagesCommunity Mental Health in India PDFAngela0% (1)
- Module 9-Child and AdolescentDocument64 pagesModule 9-Child and AdolescentRachelle malnawaNo ratings yet
- Cross Cultural Research MethodsDocument36 pagesCross Cultural Research MethodsJoanna MabutotNo ratings yet
- Clinical Psychology, Nature, Development and Activities of Clinical Psychologist (MAPSY 202)Document12 pagesClinical Psychology, Nature, Development and Activities of Clinical Psychologist (MAPSY 202)Sandhya Choudhary0% (1)
- Plan of DissertationDocument27 pagesPlan of DissertationPriya PuriNo ratings yet
- Uses of SociologyDocument17 pagesUses of SociologyVikas BhardwajNo ratings yet
- Understanding Psychological AbnormalityDocument21 pagesUnderstanding Psychological AbnormalityTitikshaNo ratings yet
- The Bio-Bio-Bio Model PDFDocument2 pagesThe Bio-Bio-Bio Model PDFchapasvegaNo ratings yet
- Optimism and HealthDocument5 pagesOptimism and HealthNL JsNo ratings yet
- DelusionsDocument8 pagesDelusionsvenkyreddy97No ratings yet
- Female Sexual Function, Dysfunction, and PregnancyDocument9 pagesFemale Sexual Function, Dysfunction, and PregnancyDiana Sofia Castillo CabreraNo ratings yet
- Mental Health Care in INdiaDocument17 pagesMental Health Care in INdiaAaditya BhattNo ratings yet
- Harm Reduction Week 7Document17 pagesHarm Reduction Week 7daedalusx99100% (1)
- Maed - English: Educ 202 - Foundation of Education (Philosophical, Sociological and Psychological)Document24 pagesMaed - English: Educ 202 - Foundation of Education (Philosophical, Sociological and Psychological)mhyka RiegoNo ratings yet
- Note AssertiveDocument26 pagesNote AssertivenuramirasidikNo ratings yet
- Organizational Behavior SEMESTER I 2010/2011: Individual EssayDocument6 pagesOrganizational Behavior SEMESTER I 2010/2011: Individual EssayxaraprotocolNo ratings yet
- CHAPTER 4 MCQS Psychology NcertDocument2 pagesCHAPTER 4 MCQS Psychology NcertHemaline RoseNo ratings yet
- Psychiatry Online - American Journal of Psychiatry - Psychiatric Disorders inDocument13 pagesPsychiatry Online - American Journal of Psychiatry - Psychiatric Disorders inAnnemarie AppletonNo ratings yet
- Thinking Healthy: A Manual For Psychosocial Management of Perinatal DepressionDocument180 pagesThinking Healthy: A Manual For Psychosocial Management of Perinatal Depressionariny oktavianyNo ratings yet
- Schizotipy Review and Relationship With SchizophreniaDocument11 pagesSchizotipy Review and Relationship With Schizophreniasofian2pNo ratings yet
- Research MethodologyDocument30 pagesResearch MethodologyHursh MaheshwariNo ratings yet
- Impact of Digital Technology On Early ChildhoodDocument34 pagesImpact of Digital Technology On Early ChildhoodJatin KanojiaNo ratings yet
- Attitude and ChangeDocument12 pagesAttitude and Changearchanasingh1767% (6)
- Module 3. Unit 1 - The PERMA ModelDocument5 pagesModule 3. Unit 1 - The PERMA ModelNicole Anne ViernesNo ratings yet
- CDC Connectiveness BookletDocument24 pagesCDC Connectiveness BookletDominique Harmon100% (1)
- Clinical Psychology 1Document8 pagesClinical Psychology 1Rineeta BanerjeeNo ratings yet
- APSAC FI Guidelines 2012Document28 pagesAPSAC FI Guidelines 2012gdlo72No ratings yet
- Understanding The Psycho-Social, Health and Livelihood Problems of People Recovered From Covid-19: An Empirical StudyDocument20 pagesUnderstanding The Psycho-Social, Health and Livelihood Problems of People Recovered From Covid-19: An Empirical StudyMutluri Abraham100% (1)
- Evidence Based PscychodynamicDocument46 pagesEvidence Based PscychodynamicSnowdrops Genevie Tan100% (1)
- Sugar: An AddictionDocument6 pagesSugar: An AddictionAditiNo ratings yet
- Pattamaporn Kittayapong #: AbstrakDocument23 pagesPattamaporn Kittayapong #: AbstrakAlfa KaromahNo ratings yet
- Peccatori2013 PDFDocument11 pagesPeccatori2013 PDFAlfa KaromahNo ratings yet
- Lee 2018Document13 pagesLee 2018Alfa KaromahNo ratings yet
- Huguelet2006 PDFDocument7 pagesHuguelet2006 PDFAlfa KaromahNo ratings yet
- 293 1050 2 PBDocument9 pages293 1050 2 PBAlfa KaromahNo ratings yet
- No Smoking in The TriangleDocument60 pagesNo Smoking in The TriangleThomas L HaydenNo ratings yet
- Identifikasi Miskonsepsi Materi IPA Kelas VII SMP N 1 Gunung Sugih Lampung TengahDocument12 pagesIdentifikasi Miskonsepsi Materi IPA Kelas VII SMP N 1 Gunung Sugih Lampung TengahMawarniwati Waruwu Undiksha 2019No ratings yet
- Prahlad 123 PDFDocument24 pagesPrahlad 123 PDFPrahlad Singh Bundela100% (1)
- SafeBoda Data Intern JDDocument2 pagesSafeBoda Data Intern JDMusah100% (1)
- Employment Tribunals: Claimant RespondentDocument42 pagesEmployment Tribunals: Claimant RespondentMichael SmithNo ratings yet
- Practical Tools For Attackers and Defenders: 6.1 Steps To Launch An AttackDocument42 pagesPractical Tools For Attackers and Defenders: 6.1 Steps To Launch An AttackRaghu Vamsi PNo ratings yet
- DRUG STUDY CefuroximeDocument2 pagesDRUG STUDY CefuroximeParado Cabañal Skyliegh50% (2)
- Bonding QuizDocument7 pagesBonding Quiz卜一斐No ratings yet
- Ce Booklet Fall 14Document28 pagesCe Booklet Fall 14api-279863771No ratings yet
- RPD QuestionsDocument77 pagesRPD QuestionsDontoNo ratings yet
- Albumina 1Document2 pagesAlbumina 1Vale FrancoNo ratings yet
- Goodman ss-gsz16Document36 pagesGoodman ss-gsz16nam nguyenNo ratings yet
- Measure of Central Tendency (Mean, Median, Mode)Document12 pagesMeasure of Central Tendency (Mean, Median, Mode)Najia SalmanNo ratings yet
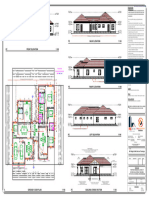
- MR Regis N MRS Dorcas Taruvinga - 050209Document1 pageMR Regis N MRS Dorcas Taruvinga - 050209pzarchitectural99No ratings yet
- ElicitingDocument4 pagesElicitingikomang agus sutejaNo ratings yet
- Identification, Storage, and Handling of Geosynthetic Rolls: Standard Guide ForDocument2 pagesIdentification, Storage, and Handling of Geosynthetic Rolls: Standard Guide ForSebastián RodríguezNo ratings yet
- 3 Math 550 Decimals Worksheets 2Document21 pages3 Math 550 Decimals Worksheets 2Havoc Subash RajNo ratings yet
- Waypa G. and Schumacker P. O2 Sensing in Hypoxic Pulmonary Vasoconstriction The Mitochondrial Door Re-Opens. Respir. Physiol. Neurobiol. (2002)Document11 pagesWaypa G. and Schumacker P. O2 Sensing in Hypoxic Pulmonary Vasoconstriction The Mitochondrial Door Re-Opens. Respir. Physiol. Neurobiol. (2002)benjabmbNo ratings yet
- Unit-7: Iot SecurityDocument21 pagesUnit-7: Iot SecuritySAMPANo ratings yet
- Major Fractures of The Pilon The Talus and The Calcaneus Current Concepts of TreatmentDocument241 pagesMajor Fractures of The Pilon The Talus and The Calcaneus Current Concepts of TreatmentPaul Radulescu - FizioterapeutNo ratings yet
- Chapter 5 - Elasticity and Its ApplicationDocument37 pagesChapter 5 - Elasticity and Its ApplicationOktaviana MuktiNo ratings yet
- "134-S" Series: Optional Gasket KitDocument45 pages"134-S" Series: Optional Gasket KitginoNo ratings yet
- All About Zookeeper and ClickHouse KeeperDocument45 pagesAll About Zookeeper and ClickHouse KeeperomyeudaihiepNo ratings yet
- Trompenaars' Cultural Dimensions in France: February 2021Document15 pagesTrompenaars' Cultural Dimensions in France: February 2021Như Hảo Nguyễn NgọcNo ratings yet
- Op AmpDocument36 pagesOp AmpLord Nafaryus100% (1)
- p103-Stts-gec-Asi-ms-ele-009 - Method Statement For Installation of Light Fitting FixtureDocument5 pagesp103-Stts-gec-Asi-ms-ele-009 - Method Statement For Installation of Light Fitting FixtureAnandu AshokanNo ratings yet
- Monash UniversityDocument17 pagesMonash Universityimmanuel nauk elokpereNo ratings yet
- H11 Heat TreatmentDocument6 pagesH11 Heat Treatmentshunmu_scribNo ratings yet
- Biology HL Student GuideDocument134 pagesBiology HL Student GuideYesenia JassoNo ratings yet
- HOPE 12 Budget of WorkDocument2 pagesHOPE 12 Budget of WorkRonald Francis Sanchez VirayNo ratings yet