Download as docx, pdf, or txt
You might also like
- Station 5 Example ScenariosDocument12 pagesStation 5 Example ScenariosDavidJohnsonNo ratings yet
- In The Public Interest - William Trever (1972)Document354 pagesIn The Public Interest - William Trever (1972)Ferris BuhlerNo ratings yet
- Occlusion in Complete Denture Part IIDocument48 pagesOcclusion in Complete Denture Part IIهجرسNo ratings yet
- Occlusion 2Document48 pagesOcclusion 2Dr Hajar Al samomiNo ratings yet
- Occlusion in Complete DentureDocument57 pagesOcclusion in Complete DentureSahana Rangarajan100% (1)
- Finishing and Detailing in OrthodonticsDocument172 pagesFinishing and Detailing in OrthodonticsDrParmod Tayal88% (8)
- Operative (Questions) #SumerDocument52 pagesOperative (Questions) #Sumerعلي صادق جعفرNo ratings yet
- Types of Balanced OcclusionDocument6 pagesTypes of Balanced Occlusionعلي صادق جعفرNo ratings yet
- سمنار كراونDocument6 pagesسمنار كراونعلي صادق جعفرNo ratings yet
- علي صادق جعفرDocument6 pagesعلي صادق جعفرعلي صادق جعفرNo ratings yet
- Balanced Occlusion: by Reema Talat Ayesha Final Year R.R.D.CDocument31 pagesBalanced Occlusion: by Reema Talat Ayesha Final Year R.R.D.CArunNo ratings yet
- Balanced OcclusionDocument9 pagesBalanced OcclusionDrShweta Saini100% (1)
- Balanced Occl PDFDocument31 pagesBalanced Occl PDFggNo ratings yet
- Occlusion in Complete DentureDocument35 pagesOcclusion in Complete DentureAkash Sikka100% (1)
- Prosthodontics Nov 2015Document30 pagesProsthodontics Nov 2015samikshaNo ratings yet
- Complete Denture OcclusionDocument54 pagesComplete Denture OcclusionDr. Aysha Sadaf100% (2)
- 2) OcclusionDocument31 pages2) OcclusionsofiyanaNo ratings yet
- Lec 6 Occluson of Complete Denture 2Document6 pagesLec 6 Occluson of Complete Denture 2pxb8dhqgs9No ratings yet
- Laws of Articulation - PPTX FinalDocument119 pagesLaws of Articulation - PPTX FinalParmod Gulia100% (1)
- Occlussion in Complete Dentures ProsthoDocument59 pagesOcclussion in Complete Dentures ProsthoFourthMolar.com100% (3)
- Occlusion / Orthodontic Courses by Indian Dental AcademyDocument90 pagesOcclusion / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Balanced Occlu HandoutDocument9 pagesBalanced Occlu HandoutMostafa FayadNo ratings yet
- Maxillo Mandibular Relation Records DR - Basma AlzubaidyDocument33 pagesMaxillo Mandibular Relation Records DR - Basma Alzubaidyمحمد عبدالهادي إسماعيلNo ratings yet
- LEC OcclusionDocument11 pagesLEC OcclusionFatimaNo ratings yet
- Dental Occlusion ConceptsDocument53 pagesDental Occlusion ConceptsDrShujahNo ratings yet
- 01 Balanced OcclusionDocument46 pages01 Balanced OcclusionAceNo ratings yet
- Occlusion 2022Document39 pagesOcclusion 2022Kaaroma TamoaietaNo ratings yet
- Occlusion OrthodonticsDocument84 pagesOcclusion OrthodonticsMuhammad UzairNo ratings yet
- Normal Occlusion: Presented By: DR Ghulam RasoolDocument41 pagesNormal Occlusion: Presented By: DR Ghulam RasoolAbdul MohaiminNo ratings yet
- ĐC Khớp cắnDocument13 pagesĐC Khớp cắnHùng VũNo ratings yet
- Oclusion in CD ProsthoDocument62 pagesOclusion in CD ProsthoFourthMolar.com50% (2)
- Đề Cương Khớp Cắn 2023Document23 pagesĐề Cương Khớp Cắn 2023Nguyễn Quang Trung Kiên (22100359)No ratings yet
- Occlusion in Fixed ProsthodonticsDocument14 pagesOcclusion in Fixed ProsthodonticsGayathri GangadharanNo ratings yet
- GPT 9Document37 pagesGPT 9MohamedNo ratings yet
- 3 Factorsaffectingbalancedocclusionfinal 190120212520Document100 pages3 Factorsaffectingbalancedocclusionfinal 190120212520Beniamin TicaratNo ratings yet
- OcclusionDocument49 pagesOcclusionRajsandeep SinghNo ratings yet
- OcclusionDocument14 pagesOcclusionpasser byNo ratings yet
- Occlusion in Complete DentureDocument6 pagesOcclusion in Complete DentureSaif HashimNo ratings yet
- The Function and Importance of Incisal Guidance inDocument75 pagesThe Function and Importance of Incisal Guidance inPragya Jain100% (1)
- تقرير crownDocument3 pagesتقرير crownمحمد نعيمNo ratings yet
- Normal OcclusionDocument33 pagesNormal OcclusionFatimah Az-ZahrahNo ratings yet
- L1&2 Occlusion ProsDocument10 pagesL1&2 Occlusion ProsMaria EvergardenNo ratings yet
- Lec8 ArangementDocument5 pagesLec8 ArangementHassan BotaniNo ratings yet
- Assignment - 4: The Saying Goes 'He/ She Who Knows Occlusion Knows Dentistry 'Document19 pagesAssignment - 4: The Saying Goes 'He/ She Who Knows Occlusion Knows Dentistry 'nivitha naidu100% (1)
- Orthodontic TERMINOLOGY: OverjetDocument5 pagesOrthodontic TERMINOLOGY: OverjetMohammedNo ratings yet
- Occlusion in FPDDocument108 pagesOcclusion in FPDVishal ReddyNo ratings yet
- 6.occlusion in OperativeDocument33 pages6.occlusion in OperativeشيماءNo ratings yet
- Protrusive Occlusal BalanceDocument5 pagesProtrusive Occlusal BalanceMohamed YounisNo ratings yet
- Occlusal SchemesDocument19 pagesOcclusal Schemesامل سالمNo ratings yet
- Mandibular MovementsDocument110 pagesMandibular MovementsNeha Aggarwal100% (1)
- Fundamentals of Occlusion: Reference: Shillingburg Funamentals of Fixed Prosthodontics, Third Edition Chapter TwoDocument44 pagesFundamentals of Occlusion: Reference: Shillingburg Funamentals of Fixed Prosthodontics, Third Edition Chapter Twoوا إسلاماه100% (2)
- Balanced OcclusionDocument120 pagesBalanced Occlusionrahel sukma100% (5)
- OcclusionDocument56 pagesOcclusionKush PathakNo ratings yet
- Anterior - GuidanceDocument21 pagesAnterior - GuidanceAayushi VaidyaNo ratings yet
- Concept of OcclusionDocument81 pagesConcept of Occlusionchawalito27100% (1)
- 1,2-Prosthodontic - Docx (1,2) Fifth ClassDocument6 pages1,2-Prosthodontic - Docx (1,2) Fifth Classjbkw2hcnfpNo ratings yet
- Setting Teeth On The ArticulatorDocument81 pagesSetting Teeth On The Articulatorameer mousaNo ratings yet
- Occlusion 1 (Autosaved)Document70 pagesOcclusion 1 (Autosaved)ShreyaNo ratings yet
- Occlusion Concepts in DentistryDocument81 pagesOcclusion Concepts in Dentistrydorasani99No ratings yet
- Oral Pathology: Hyperplasia of Oral MucosaDocument7 pagesOral Pathology: Hyperplasia of Oral Mucosaعلي صادق جعفرNo ratings yet
- Lec-18 - Diseases of Saivary GlandsDocument7 pagesLec-18 - Diseases of Saivary Glandsعلي صادق جعفرNo ratings yet
- Oral Pathology: 2-Mesenchymal Origin Tumors A - Odontogenic FibromaDocument4 pagesOral Pathology: 2-Mesenchymal Origin Tumors A - Odontogenic Fibromaعلي صادق جعفرNo ratings yet
- Periapical PeriodontitisDocument7 pagesPeriapical Periodontitisعلي صادق جعفرNo ratings yet
- Ceramic Crown For Children PDFDocument5 pagesCeramic Crown For Children PDFعلي صادق جعفرNo ratings yet
- Oral Pathology: Odontogenic TumorsDocument5 pagesOral Pathology: Odontogenic Tumorsعلي صادق جعفرNo ratings yet
- Oral Pathology: Non-Epithelialized Primary Bone CystDocument4 pagesOral Pathology: Non-Epithelialized Primary Bone Cystعلي صادق جعفرNo ratings yet
- سمنار كراونDocument6 pagesسمنار كراونعلي صادق جعفرNo ratings yet
- PHSW CME Sedation Answer KeyDocument10 pagesPHSW CME Sedation Answer Keyعلي صادق جعفرNo ratings yet
- Paranasal SinusesDocument18 pagesParanasal Sinusesعلي صادق جعفرNo ratings yet
- Endodontic Mishaps 1Document10 pagesEndodontic Mishaps 1علي صادق جعفرNo ratings yet
- 5th Stage: - NazhatDocument11 pages5th Stage: - Nazhatعلي صادق جعفرNo ratings yet
- علي صادق جعفرDocument6 pagesعلي صادق جعفرعلي صادق جعفرNo ratings yet
- Oral Surgery: Ankylosis ofDocument9 pagesOral Surgery: Ankylosis ofعلي صادق جعفرNo ratings yet
- رفعج قداص يلع بلاطلا رانمس Group D Pollution in dental clinic (radiation pollution)Document10 pagesرفعج قداص يلع بلاطلا رانمس Group D Pollution in dental clinic (radiation pollution)علي صادق جعفرNo ratings yet
- TMJ 2Document8 pagesTMJ 2علي صادق جعفرNo ratings yet
- Types of Balanced OcclusionDocument6 pagesTypes of Balanced Occlusionعلي صادق جعفرNo ratings yet
- Dr. Steevens' Hospital Dublin 8: Nurses and Midwives With The Nursing and Midwifery Board of IrelandDocument2 pagesDr. Steevens' Hospital Dublin 8: Nurses and Midwives With The Nursing and Midwifery Board of IrelandLexNo ratings yet
- Nursing Process in PharmacologyDocument8 pagesNursing Process in PharmacologyQueeny Anne ApilNo ratings yet
- Dianne - DrugsDocument5 pagesDianne - DrugsJeaniel Joy Babol BS CRIMNo ratings yet
- Current Concepts in Plastic Surgery - AgulloDocument273 pagesCurrent Concepts in Plastic Surgery - AgulloAnonymous LnWIBo1GNo ratings yet
- Client Intake FormDocument1 pageClient Intake Formapi-162312216No ratings yet
- Immediate Implant Placement PDFDocument11 pagesImmediate Implant Placement PDFFerdinan PasaribuNo ratings yet
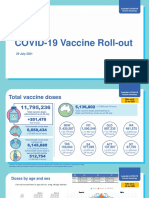
- Australian Covid 19 Vaccine Rollout Update 29 July 2021Document15 pagesAustralian Covid 19 Vaccine Rollout Update 29 July 2021Tom BurtonNo ratings yet
- Vis AnneDocument22 pagesVis AnneImelda AtikaNo ratings yet
- HEALTH EDUCATION Nursing Process PNCDocument2 pagesHEALTH EDUCATION Nursing Process PNCbaby100% (1)
- Nanda 2018Document5 pagesNanda 2018Arizal SetyawanNo ratings yet
- Wftemplate YourPCNCodeHereDocument4 pagesWftemplate YourPCNCodeHereCrissie TolentinoNo ratings yet
- Final Round Case PDFDocument20 pagesFinal Round Case PDFTahiratul ElmaNo ratings yet
- Applied KinesiologyDocument5 pagesApplied KinesiologyPierre SERPAGGINo ratings yet
- Health Care DeliveryDocument51 pagesHealth Care DeliveryUmesh KawalkarNo ratings yet
- Flabex CapsuleDocument3 pagesFlabex Capsulehk_scribdNo ratings yet
- Master Problem List (MPL) : España BLVD., Manila 1015 Tel Nos. 731-3001 To 29Document1 pageMaster Problem List (MPL) : España BLVD., Manila 1015 Tel Nos. 731-3001 To 29Jolaine ValloNo ratings yet
- Splinting of Teeth Following TraumaDocument73 pagesSplinting of Teeth Following TraumaSHRINIVAS GARJENo ratings yet
- 2015 NYUCD Bench Test Prep CourseDocument1 page2015 NYUCD Bench Test Prep CourseAnonymous GyqTkXMwMNo ratings yet
- Henry Nnorom. Electronic Health Records (2021SU) Summer 2021Document4 pagesHenry Nnorom. Electronic Health Records (2021SU) Summer 2021henry nnoromNo ratings yet
- Actual NleDocument22 pagesActual NleRuan MarchessaNo ratings yet
- Ortodoncia Brackets inDocument17 pagesOrtodoncia Brackets injavierNo ratings yet
- Anti Streptolysin ODocument16 pagesAnti Streptolysin Ochippai100% (1)
- Effects of Homelessness On The ElderlyDocument18 pagesEffects of Homelessness On The ElderlyLoganGeren100% (1)
- Resume FinalDocument2 pagesResume Finalapi-360930964No ratings yet
- 3.7 Organ Transplantation PDFDocument3 pages3.7 Organ Transplantation PDFbrownieallennNo ratings yet
- A Comparative Study of Two Nebulizers in The Emergency Department Breath-Actuated Nebulizer and Handheld NebulizerDocument7 pagesA Comparative Study of Two Nebulizers in The Emergency Department Breath-Actuated Nebulizer and Handheld Nebulizerfachrudin arNo ratings yet
- Evaluation of Diagnostic Criteria For Crohn's Disease in JapanDocument8 pagesEvaluation of Diagnostic Criteria For Crohn's Disease in JapanBobby Faisyal RakhmanNo ratings yet
- Unit 29 Surgical PTDocument3 pagesUnit 29 Surgical PTKarla GattisNo ratings yet