
Neuropathic Pain Needs Systematic Classification.
Neuropathic Pain Needs Systematic Classification.
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Blueprint - 4 - Workbook - Answer - Key 17Document52 pagesBlueprint - 4 - Workbook - Answer - Key 17Adam Ali100% (8)
- NURS - FPX 5005 - Brendan Madden - Assessment - 2-1Document9 pagesNURS - FPX 5005 - Brendan Madden - Assessment - 2-1SohaibNo ratings yet
- Public: Ydt Mini Deneme Sinavi 50 SoruDocument8 pagesPublic: Ydt Mini Deneme Sinavi 50 SoruGustavo GaviriaNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Sheri Van Dijk - Relationship Skills 101 For Teens PDFDocument209 pagesSheri Van Dijk - Relationship Skills 101 For Teens PDFWesley Riann50% (2)
- Emergencies in Palliative CareDocument3 pagesEmergencies in Palliative CareJorge Cortina GonzalesNo ratings yet
- Systemic Administration of Local Anesthetic Agents To Relieve Neuropathic PainDocument3 pagesSystemic Administration of Local Anesthetic Agents To Relieve Neuropathic PainJorge Cortina GonzalesNo ratings yet
- Opioids For Neuropathic PainDocument3 pagesOpioids For Neuropathic PainJorge Cortina GonzalesNo ratings yet
- Animal Therapy For Elderly With Memory DisordersDocument67 pagesAnimal Therapy For Elderly With Memory DisordersJorge Cortina GonzalesNo ratings yet
- ''Serious and Complex Illness'' in Quality Improvement and Policy Reform For End of Life CareDocument5 pages''Serious and Complex Illness'' in Quality Improvement and Policy Reform For End of Life CareJorge Cortina GonzalesNo ratings yet
- Cochrane Handbook 21-2019Document24 pagesCochrane Handbook 21-2019Gilda BBTTNo ratings yet
- Ecircular - 4166 - New Products LaunchDocument3 pagesEcircular - 4166 - New Products LaunchLim you enNo ratings yet
- A Real Time Case Study - The Training Manager PDFDocument2 pagesA Real Time Case Study - The Training Manager PDFUsha SinghNo ratings yet
- Research 4Document11 pagesResearch 4Arjane SalongaNo ratings yet
- 1 s2.0 S0169500221000453 MainDocument4 pages1 s2.0 S0169500221000453 MainNoman M HasanNo ratings yet
- 1631 DN4 QuestionnaireDocument2 pages1631 DN4 QuestionnaireRaywa 217100% (1)
- Actividad 2-U3 - (English 4)Document3 pagesActividad 2-U3 - (English 4)Atsuko_lucyNo ratings yet
- Module 7 WK 7 Death Final File - StudentDocument9 pagesModule 7 WK 7 Death Final File - StudentLilowsNo ratings yet
- COVID-19 Waste Management Sourcebook Ver 09232021Document103 pagesCOVID-19 Waste Management Sourcebook Ver 09232021Christopher de LeonNo ratings yet
- Chandima de Alwis Seneviratne Healthcare ResumeDocument1 pageChandima de Alwis Seneviratne Healthcare Resumechandima.senevi23No ratings yet
- J8 Family Violence and Covid 19 Increased VulnerabilityDocument4 pagesJ8 Family Violence and Covid 19 Increased VulnerabilityJimena Barra GutiérrezNo ratings yet
- Capstone Project Proposal Draft FillableDocument9 pagesCapstone Project Proposal Draft Fillableapi-565971189No ratings yet
- Laboratorios Valores EndocrinoDocument88 pagesLaboratorios Valores EndocrinoS ONo ratings yet
- Physical DependenceDocument7 pagesPhysical Dependencehasan jamiNo ratings yet
- Case Study: Interventions 1Document23 pagesCase Study: Interventions 1Ketoki MazumdarNo ratings yet
- Health Guard Proposal Form PrintDocument4 pagesHealth Guard Proposal Form Printrock_on_rupz99No ratings yet
- Chapters 1 3Document44 pagesChapters 1 3Azriel Mae BaylonNo ratings yet
- Rayagada 2nd SUBDocument3 pagesRayagada 2nd SUBsitikantha sahooNo ratings yet
- EmpathyDocument5 pagesEmpathyHijaab KhaanNo ratings yet
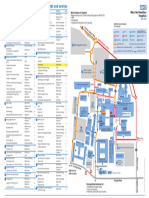
- WGH Site MapDocument1 pageWGH Site MapLuizaNo ratings yet
- Eilan Brand Book SmallDocument28 pagesEilan Brand Book SmallMadushanNo ratings yet
- OSH Manual Medium Risk EntitiesDocument122 pagesOSH Manual Medium Risk EntitiesNitika SinhaNo ratings yet
- Series in Transpersonal and Humanistic Psychology) Stanislav Grof - Beyond The Brain - Birth, Death, and Transcendence in Psychotherapy-State University of New York Press (1985)Document484 pagesSeries in Transpersonal and Humanistic Psychology) Stanislav Grof - Beyond The Brain - Birth, Death, and Transcendence in Psychotherapy-State University of New York Press (1985)Darzan ConstantinNo ratings yet
- Aims and Objectives and Literature ReviewDocument4 pagesAims and Objectives and Literature ReviewMomin AhsanNo ratings yet
- HSE Advisor The Role:: Occupational HealthDocument3 pagesHSE Advisor The Role:: Occupational Healthmohamed atefNo ratings yet
- OSH Roles and Responsibilities ProcedureDocument10 pagesOSH Roles and Responsibilities ProcedureSanjeet SinghNo ratings yet










































































Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Blueprint - 4 - Workbook - Answer - Key 17Document52 pagesBlueprint - 4 - Workbook - Answer - Key 17Adam Ali100% (8)
- NURS - FPX 5005 - Brendan Madden - Assessment - 2-1Document9 pagesNURS - FPX 5005 - Brendan Madden - Assessment - 2-1SohaibNo ratings yet
- Public: Ydt Mini Deneme Sinavi 50 SoruDocument8 pagesPublic: Ydt Mini Deneme Sinavi 50 SoruGustavo GaviriaNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Sheri Van Dijk - Relationship Skills 101 For Teens PDFDocument209 pagesSheri Van Dijk - Relationship Skills 101 For Teens PDFWesley Riann50% (2)
- Emergencies in Palliative CareDocument3 pagesEmergencies in Palliative CareJorge Cortina GonzalesNo ratings yet
- Systemic Administration of Local Anesthetic Agents To Relieve Neuropathic PainDocument3 pagesSystemic Administration of Local Anesthetic Agents To Relieve Neuropathic PainJorge Cortina GonzalesNo ratings yet
- Opioids For Neuropathic PainDocument3 pagesOpioids For Neuropathic PainJorge Cortina GonzalesNo ratings yet
- Animal Therapy For Elderly With Memory DisordersDocument67 pagesAnimal Therapy For Elderly With Memory DisordersJorge Cortina GonzalesNo ratings yet
- ''Serious and Complex Illness'' in Quality Improvement and Policy Reform For End of Life CareDocument5 pages''Serious and Complex Illness'' in Quality Improvement and Policy Reform For End of Life CareJorge Cortina GonzalesNo ratings yet
- Cochrane Handbook 21-2019Document24 pagesCochrane Handbook 21-2019Gilda BBTTNo ratings yet
- Ecircular - 4166 - New Products LaunchDocument3 pagesEcircular - 4166 - New Products LaunchLim you enNo ratings yet
- A Real Time Case Study - The Training Manager PDFDocument2 pagesA Real Time Case Study - The Training Manager PDFUsha SinghNo ratings yet
- Research 4Document11 pagesResearch 4Arjane SalongaNo ratings yet
- 1 s2.0 S0169500221000453 MainDocument4 pages1 s2.0 S0169500221000453 MainNoman M HasanNo ratings yet
- 1631 DN4 QuestionnaireDocument2 pages1631 DN4 QuestionnaireRaywa 217100% (1)
- Actividad 2-U3 - (English 4)Document3 pagesActividad 2-U3 - (English 4)Atsuko_lucyNo ratings yet
- Module 7 WK 7 Death Final File - StudentDocument9 pagesModule 7 WK 7 Death Final File - StudentLilowsNo ratings yet
- COVID-19 Waste Management Sourcebook Ver 09232021Document103 pagesCOVID-19 Waste Management Sourcebook Ver 09232021Christopher de LeonNo ratings yet
- Chandima de Alwis Seneviratne Healthcare ResumeDocument1 pageChandima de Alwis Seneviratne Healthcare Resumechandima.senevi23No ratings yet
- J8 Family Violence and Covid 19 Increased VulnerabilityDocument4 pagesJ8 Family Violence and Covid 19 Increased VulnerabilityJimena Barra GutiérrezNo ratings yet
- Capstone Project Proposal Draft FillableDocument9 pagesCapstone Project Proposal Draft Fillableapi-565971189No ratings yet
- Laboratorios Valores EndocrinoDocument88 pagesLaboratorios Valores EndocrinoS ONo ratings yet
- Physical DependenceDocument7 pagesPhysical Dependencehasan jamiNo ratings yet
- Case Study: Interventions 1Document23 pagesCase Study: Interventions 1Ketoki MazumdarNo ratings yet
- Health Guard Proposal Form PrintDocument4 pagesHealth Guard Proposal Form Printrock_on_rupz99No ratings yet
- Chapters 1 3Document44 pagesChapters 1 3Azriel Mae BaylonNo ratings yet
- Rayagada 2nd SUBDocument3 pagesRayagada 2nd SUBsitikantha sahooNo ratings yet
- EmpathyDocument5 pagesEmpathyHijaab KhaanNo ratings yet
- WGH Site MapDocument1 pageWGH Site MapLuizaNo ratings yet
- Eilan Brand Book SmallDocument28 pagesEilan Brand Book SmallMadushanNo ratings yet
- OSH Manual Medium Risk EntitiesDocument122 pagesOSH Manual Medium Risk EntitiesNitika SinhaNo ratings yet
- Series in Transpersonal and Humanistic Psychology) Stanislav Grof - Beyond The Brain - Birth, Death, and Transcendence in Psychotherapy-State University of New York Press (1985)Document484 pagesSeries in Transpersonal and Humanistic Psychology) Stanislav Grof - Beyond The Brain - Birth, Death, and Transcendence in Psychotherapy-State University of New York Press (1985)Darzan ConstantinNo ratings yet
- Aims and Objectives and Literature ReviewDocument4 pagesAims and Objectives and Literature ReviewMomin AhsanNo ratings yet
- HSE Advisor The Role:: Occupational HealthDocument3 pagesHSE Advisor The Role:: Occupational Healthmohamed atefNo ratings yet
- OSH Roles and Responsibilities ProcedureDocument10 pagesOSH Roles and Responsibilities ProcedureSanjeet SinghNo ratings yet