Download as pdf or txt
You might also like
- MCQs On Complete DenturesDocument20 pagesMCQs On Complete Denturesمحمد العراقي87% (46)
- Nebosh IGC Element 1. Foundations in Health and Safety (Notes)Document7 pagesNebosh IGC Element 1. Foundations in Health and Safety (Notes)kkalvi92% (204)
- Textbook of Psychiatry - Basant K. PuriDocument478 pagesTextbook of Psychiatry - Basant K. PuriThao Pham93% (14)
- The Black Book of TattooingDocument124 pagesThe Black Book of Tattooingmind_warps80% (15)
- Extraoral Orthopaedic AppliancesDocument59 pagesExtraoral Orthopaedic AppliancesAmatullahsadiyaNo ratings yet
- Dental ImplantsDocument30 pagesDental Implantsآلاء حسن يونسNo ratings yet
- Is Manual EngDocument32 pagesIs Manual EngsfaquiraNo ratings yet
- Attachment Procedures: Attachments in DentistryDocument7 pagesAttachment Procedures: Attachments in DentistryAngela Yohana PeñaNo ratings yet
- OrthodonticsDocument123 pagesOrthodonticsAyesha Anwar90% (10)
- Library Dissertation On Dental ImplantsDocument8 pagesLibrary Dissertation On Dental ImplantsHelpWritingPapersForCollegeSalem100% (1)
- Understanding Orthodontic Bone Screws - IntechOpenDocument23 pagesUnderstanding Orthodontic Bone Screws - IntechOpenshyama pramodNo ratings yet
- Flexible Partial DentureDocument5 pagesFlexible Partial DentureDeasireeNo ratings yet
- Orthodontics: Orthopaedic Appliances Dr. Ayam A. TahaDocument13 pagesOrthodontics: Orthopaedic Appliances Dr. Ayam A. TahaQueen LiveNo ratings yet
- Microtornillos en OrtodonciaDocument6 pagesMicrotornillos en OrtodonciaAlan SernasNo ratings yet
- Attachment Procedures: Attachments in DentistryDocument7 pagesAttachment Procedures: Attachments in DentistryRohan GroverNo ratings yet
- CR October 2019Document8 pagesCR October 2019maiNo ratings yet
- Gox 10 E4359Document3 pagesGox 10 E4359gbaez.88No ratings yet
- SJODR 59 431-433 CDocument3 pagesSJODR 59 431-433 CJean-Philippe MercierNo ratings yet
- The SPEED System: An Overview of The Appliance and Clinical PerformanceDocument10 pagesThe SPEED System: An Overview of The Appliance and Clinical PerformanceMARIA NAENo ratings yet
- Seminars in Ortho Don Ics 20081454Document10 pagesSeminars in Ortho Don Ics 20081454MARIA NAENo ratings yet
- Glass Ionomer Endodontic Sealers - A Literature ReviewDocument6 pagesGlass Ionomer Endodontic Sealers - A Literature Reviewea1yd6vnNo ratings yet
- Dental Implant DissertationDocument6 pagesDental Implant DissertationHelpMeWriteAPaperUK100% (1)
- 270 Accel Tapered WebDocument4 pages270 Accel Tapered WebhaneefmdfNo ratings yet
- A To Z Orthodontics Vol 13 Fixed Appliances PDFDocument32 pagesA To Z Orthodontics Vol 13 Fixed Appliances PDFKIH 20162017No ratings yet
- PIIS2212443823000577Document7 pagesPIIS2212443823000577ALBERTO JESUS PACHECO DIAZNo ratings yet
- OrthopedicDocument41 pagesOrthopedicSibi NairNo ratings yet
- Thesis Topics in ProsthodonticsDocument6 pagesThesis Topics in ProsthodonticsSharon Collins100% (2)
- Restoring Non-Restorable With The Help of Customized Digital Solutions: A ReviewDocument4 pagesRestoring Non-Restorable With The Help of Customized Digital Solutions: A ReviewDey AzzNo ratings yet
- Technique For Fabrication of Customised Metal Mesh Reinforced Complete Dentures - Pressing Need To Avoid Complete Denture Fractures A Case ReportDocument4 pagesTechnique For Fabrication of Customised Metal Mesh Reinforced Complete Dentures - Pressing Need To Avoid Complete Denture Fractures A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Tooth Structure Removal Associated With Various PRDocument11 pagesTooth Structure Removal Associated With Various PRHector Flores SotoNo ratings yet
- Prosthetic Rehabilitation On Resorbed Ridge: A Case ReportDocument5 pagesProsthetic Rehabilitation On Resorbed Ridge: A Case ReportIJAR JOURNALNo ratings yet
- SR Phonares II Tooth Mould ChartDocument8 pagesSR Phonares II Tooth Mould Chartcatalin_adinaNo ratings yet
- Mini Implantes en Ortodoncia .Document9 pagesMini Implantes en Ortodoncia .erika de andradeNo ratings yet
- SR Orthotyp S DCL SR Orthotyp S PE SR Vivodent S DCL SR Vivodent S PE en V01 6207Document20 pagesSR Orthotyp S DCL SR Orthotyp S PE SR Vivodent S DCL SR Vivodent S PE en V01 6207Guillaume Scala-BertolaNo ratings yet
- Liquid-Supported Denture-A Boon To Flabby RidgesDocument4 pagesLiquid-Supported Denture-A Boon To Flabby RidgesTarak ChavadaNo ratings yet
- Orthopaedic AppliancesDocument25 pagesOrthopaedic ApplianceschandanpreetNo ratings yet
- Cast Partial Denture With Attachment Boon To PreveDocument7 pagesCast Partial Denture With Attachment Boon To PreveMamta SentaNo ratings yet
- Marburg Double Crown System For Partial DentureDocument10 pagesMarburg Double Crown System For Partial DentureAhmad Shoeib100% (1)
- PSI Main Flyer Dip MoldingDocument2 pagesPSI Main Flyer Dip MoldingFaiz IbrahimNo ratings yet
- 2021 Kadambari BharaliDocument6 pages2021 Kadambari Bharali謎超人No ratings yet
- Acrylic Partial DenturesDocument6 pagesAcrylic Partial DenturesCloudcynaraaNo ratings yet
- Acrylic Partial DenturesDocument6 pagesAcrylic Partial Denturesruth graceNo ratings yet
- PG Canine Retraction Spring: Methods in MedicineDocument2 pagesPG Canine Retraction Spring: Methods in MedicineAjayNo ratings yet
- DR Ghazy 2012 MY IMPLANT LECTURE For 4th Year StudentsDocument25 pagesDR Ghazy 2012 MY IMPLANT LECTURE For 4th Year StudentsMohamed Hamed GhazyNo ratings yet
- Biomech of Lingual PDFDocument13 pagesBiomech of Lingual PDFLikhitaNo ratings yet
- FFA Flexible and Rigid Summary PDFDocument17 pagesFFA Flexible and Rigid Summary PDFrohit100% (1)
- Nam LDDocument4 pagesNam LDisha MehtaNo ratings yet
- Tongue Cave A TAD Supported Customized Habit Breaking ApplianceDocument3 pagesTongue Cave A TAD Supported Customized Habit Breaking ApplianceInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Functional AppliancesDocument67 pagesFunctional Appliancesdod.084No ratings yet
- Contemporary Ortho AppliancesDocument51 pagesContemporary Ortho AppliancesGeorge CharchNo ratings yet
- Castiblanco (2017Document12 pagesCastiblanco (2017Asesor PSSNo ratings yet
- Wjo 11 4 Gandedkar 9Document12 pagesWjo 11 4 Gandedkar 9Vijay ChinthaNo ratings yet
- Micro-Implants For Orthodontic Anchorage: A Review: July 2013Document6 pagesMicro-Implants For Orthodontic Anchorage: A Review: July 2013Vijay ChinthaNo ratings yet
- Esthetic Anterior Fixed Functional Space Maintainer: Case ReportDocument3 pagesEsthetic Anterior Fixed Functional Space Maintainer: Case ReportdeaNo ratings yet
- 3D Dental Prosthetic Tooth Crown: Re-Modeling of Customized Tooth Crown Using Additive Manufacturing and Synthesis of Bio-Compactible Tooth FillingDocument8 pages3D Dental Prosthetic Tooth Crown: Re-Modeling of Customized Tooth Crown Using Additive Manufacturing and Synthesis of Bio-Compactible Tooth FillingInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Temporary Anchorage Device (TAD's)Document121 pagesTemporary Anchorage Device (TAD's)Chandra Sekhar Reddy100% (2)
- Implant - Ortho1 PDFDocument8 pagesImplant - Ortho1 PDFradhasrNo ratings yet
- 5.richmond CrownDocument9 pages5.richmond CrownSoham DattaNo ratings yet
- Company Introduction (Part)Document29 pagesCompany Introduction (Part)Lokender YadavNo ratings yet
- Twin Block Appliance ThesisDocument6 pagesTwin Block Appliance Thesisjessicahillnewyork100% (2)
- Isra AljalyDocument11 pagesIsra AljalyAbady SharifNo ratings yet
- JCO11 19pendulisDocument12 pagesJCO11 19pendulisVishal VijNo ratings yet
- DENTURES: The Ultimate Guide to Dentures & Denture Care for a Beautifully Restored SmileFrom EverandDENTURES: The Ultimate Guide to Dentures & Denture Care for a Beautifully Restored SmileNo ratings yet
- UncompleteDocument75 pagesUncompleteمحمد العراقيNo ratings yet
- HHS Public Access: Association of Periodontitis and Human Papillomavirus in Oral Rinse Specimens NHANES 2009-2012Document13 pagesHHS Public Access: Association of Periodontitis and Human Papillomavirus in Oral Rinse Specimens NHANES 2009-2012محمد العراقيNo ratings yet
- Periodontal Diseases and Risk of Oral Cancer in Southern India: Results From The Hence Life StudyDocument8 pagesPeriodontal Diseases and Risk of Oral Cancer in Southern India: Results From The Hence Life Studyمحمد العراقيNo ratings yet
- Multiple Choice Questions-Mechanical Plaque ControlDocument18 pagesMultiple Choice Questions-Mechanical Plaque Controlمحمد العراقيNo ratings yet
- Patho mcq20Document30 pagesPatho mcq20محمد العراقيNo ratings yet
- Both Statements Are False: Your Answer Is WrongDocument3 pagesBoth Statements Are False: Your Answer Is Wrongمحمد العراقيNo ratings yet
- Centrifug VVVVDocument1 pageCentrifug VVVVمحمد العراقيNo ratings yet
- Alimentary Canal of HumanDocument37 pagesAlimentary Canal of Humanمحمد العراقيNo ratings yet
- Patho mcq16Document9 pagesPatho mcq16محمد العراقيNo ratings yet
- Tooth Discoloration: DR Bindu Kumari (BDS)Document32 pagesTooth Discoloration: DR Bindu Kumari (BDS)محمد العراقيNo ratings yet
- Intrinsic DiscolorationDocument6 pagesIntrinsic Discolorationمحمد العراقيNo ratings yet
- Reverse Facial Mask: لعزخ يؤل نسح University of Kirkuk College of DentistryDocument5 pagesReverse Facial Mask: لعزخ يؤل نسح University of Kirkuk College of Dentistryمحمد العراقيNo ratings yet
- Gingival Enlargment: Maryam Aziz Ahmed Fourth Stage Group - CDocument15 pagesGingival Enlargment: Maryam Aziz Ahmed Fourth Stage Group - Cمحمد العراقيNo ratings yet
- Alveolar Bone: and It's Associated PathologiesDocument7 pagesAlveolar Bone: and It's Associated Pathologiesمحمد العراقيNo ratings yet
- Alanine 55 PDFDocument3 pagesAlanine 55 PDFمحمد العراقيNo ratings yet
- Plaque Control: Ameen Fadhel Group (D)Document31 pagesPlaque Control: Ameen Fadhel Group (D)محمد العراقيNo ratings yet
- Reverse Facial Mask: Prepared by Shafa Fwad FaeeqDocument5 pagesReverse Facial Mask: Prepared by Shafa Fwad Faeeqمحمد العراقيNo ratings yet
- My Study10Document12 pagesMy Study10محمد العراقيNo ratings yet
- Gingiva Diseases Of89Document3 pagesGingiva Diseases Of89محمد العراقيNo ratings yet
- My Study5Document50 pagesMy Study5محمد العراقيNo ratings yet
- DevelopmentalDocument27 pagesDevelopmentalمحمد العراقيNo ratings yet
- Orthodontic Studies123Document6 pagesOrthodontic Studies123محمد العراقيNo ratings yet
- Human Anatomy Mandibular NerveDocument23 pagesHuman Anatomy Mandibular Nerveمحمد العراقيNo ratings yet
- Final Impression: Objectives and MaterialsDocument28 pagesFinal Impression: Objectives and Materialsمحمد العراقيNo ratings yet
- My Study1Document11 pagesMy Study1محمد العراقيNo ratings yet
- Histo - Respiratory System - TheoryDocument12 pagesHisto - Respiratory System - Theoryمحمد العراقيNo ratings yet
- My Study4Document9 pagesMy Study4محمد العراقيNo ratings yet
- Centrifuge Aug2011Document1 pageCentrifuge Aug2011محمد العراقيNo ratings yet
- The Stomach: Second Phase of Digestion, Following Mastication in The Mouth (Chewing) - It SecretesDocument9 pagesThe Stomach: Second Phase of Digestion, Following Mastication in The Mouth (Chewing) - It Secretesمحمد العراقيNo ratings yet
- Sorghum AntiviralDocument5 pagesSorghum Antiviralnugraha widyatmonoNo ratings yet
- Metered Dose Inhaler Use Technique and Its Association With Asthma Control Among Adult Asthmatic Patients Attending Outpatient ClinicDocument12 pagesMetered Dose Inhaler Use Technique and Its Association With Asthma Control Among Adult Asthmatic Patients Attending Outpatient ClinicbezieNo ratings yet
- Imaging For Neuro-Ophthalmic and Orbital Disease - A ReviewDocument24 pagesImaging For Neuro-Ophthalmic and Orbital Disease - A ReviewMashhoor AlfayezNo ratings yet
- Vital SignDocument15 pagesVital SignJalabs YouNo ratings yet
- Dr. Ali Khamis - CVDocument2 pagesDr. Ali Khamis - CVAli KhamisNo ratings yet
- Chaves 2020Document10 pagesChaves 2020Matheus CastroNo ratings yet
- JAdvPharmTechRes24236-4617086 124930Document5 pagesJAdvPharmTechRes24236-4617086 124930Reena SapruNo ratings yet
- Homeopathic Repertory of Modern Drugs Volume III Completo 2 Ed 2021Document808 pagesHomeopathic Repertory of Modern Drugs Volume III Completo 2 Ed 2021Mohit KanjwaniNo ratings yet
- Lazareto Elementary School Detailed Lesson Plan Subject: Health Date: December 11,2018 Grade Level: VIDocument7 pagesLazareto Elementary School Detailed Lesson Plan Subject: Health Date: December 11,2018 Grade Level: VILimwell Villanueva100% (2)
- NCP PediaDocument2 pagesNCP PediaJoey JoseNo ratings yet
- Theories of Ageing: DR Prema BalusamyDocument19 pagesTheories of Ageing: DR Prema Balusamyprema balusamyNo ratings yet
- Investigatory Project ON Diabetes Mellitus: Name: Sagnik KulaviDocument22 pagesInvestigatory Project ON Diabetes Mellitus: Name: Sagnik Kulavisancharini kulaviNo ratings yet
- MCI ResponseDocument57 pagesMCI ResponseAGUSTINNo ratings yet
- Nursingcrib Com NURSING CARE PLAN Hepatitis A PDFDocument2 pagesNursingcrib Com NURSING CARE PLAN Hepatitis A PDFswapnilazarusNo ratings yet
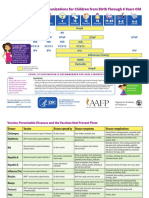
- Parent Ver SCH 0 6yrsDocument2 pagesParent Ver SCH 0 6yrsSrinivasamurthy KamarthiNo ratings yet
- Elisabeth Kübler-Ross - Five Stages of GriefDocument8 pagesElisabeth Kübler-Ross - Five Stages of Griefaastha jainNo ratings yet
- PAMA NursingCaseStudy Revised PDFDocument77 pagesPAMA NursingCaseStudy Revised PDFJeofy PamaNo ratings yet
- PathologyDocument32 pagesPathologyShashanka PoudelNo ratings yet
- Cognitive Impairment in Late-Life Generalized Anxiety DisorderDocument7 pagesCognitive Impairment in Late-Life Generalized Anxiety DisorderAnais UrdanetaNo ratings yet
- A. Cotton Blue: False TrueDocument5 pagesA. Cotton Blue: False TrueDevinViscars100% (1)
- np4 TestDocument8 pagesnp4 TestNayrbryan RamirezNo ratings yet
- Case PresentationDocument18 pagesCase PresentationNoli Galope IINo ratings yet
- Cancer Prediction Using Machine LearningDocument5 pagesCancer Prediction Using Machine LearningNoel BinoyNo ratings yet
- 三民高三上第二次月考複習 教師卷Document12 pages三民高三上第二次月考複習 教師卷黃紘志No ratings yet
- FLCCC Summary of The Evidence of Ivermectin in COVID 19Document3 pagesFLCCC Summary of The Evidence of Ivermectin in COVID 19Muhamad ZaidNo ratings yet
- TAPSE AgainDocument8 pagesTAPSE Againomotola ajayiNo ratings yet
- APA - DSM5 - Severity Measure For Separation Anxiety Disorder Adult PDFDocument3 pagesAPA - DSM5 - Severity Measure For Separation Anxiety Disorder Adult PDFMelissandreNo ratings yet