Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
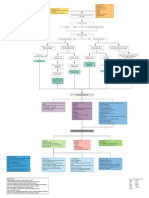
- Myocardial Infarction With CABG Concept MapDocument1 pageMyocardial Infarction With CABG Concept MapMaria Therese100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Cna Sample TestDocument19 pagesCna Sample TestArnie Gadaingan100% (2)
- The Passions of The Soul - René Descartes PDFDocument90 pagesThe Passions of The Soul - René Descartes PDFJimini MochiNo ratings yet
- Acute and Suppurative AppendicitisDocument25 pagesAcute and Suppurative AppendicitisSheba Ibabao-Alayon Moradilla0% (1)
- Fundamentals of Cardiology For The USMLE and General Medics PDFDocument287 pagesFundamentals of Cardiology For The USMLE and General Medics PDFMaria Patitu100% (2)
- ZoologyDocument32 pagesZoologyChrisshalyn Sy PinedaNo ratings yet
- Central Retinal Vein Occlusion Differential DiagnosisDocument12 pagesCentral Retinal Vein Occlusion Differential Diagnosismina2085No ratings yet
- IV TherapyDocument136 pagesIV TherapyJulie May Suganob100% (2)
- PBL DiscussionsDocument70 pagesPBL DiscussionsMaria ThereseNo ratings yet
- Case Study: Ethical DilemmaDocument2 pagesCase Study: Ethical DilemmaMaria ThereseNo ratings yet
- Malnutrition NCPDocument1 pageMalnutrition NCPMaria Therese100% (1)
- Case Analysis: Medical Surgical NursingDocument7 pagesCase Analysis: Medical Surgical NursingMaria ThereseNo ratings yet
- Case Analysis: Pre-OperativeDocument12 pagesCase Analysis: Pre-OperativeMaria ThereseNo ratings yet
- Duty Requirements: Operating RoomDocument16 pagesDuty Requirements: Operating RoomMaria ThereseNo ratings yet
- Nursing Care Plan #1: IndependentDocument3 pagesNursing Care Plan #1: IndependentMaria ThereseNo ratings yet
- Growing FetusDocument4 pagesGrowing FetusMaria ThereseNo ratings yet
- Ehealth ReportDocument6 pagesEhealth ReportMaria ThereseNo ratings yet
- MalariaDocument7 pagesMalariaMaria ThereseNo ratings yet
- To Be Submitted By: Ma. Therese P. Ballares BSN 2 - NCDocument6 pagesTo Be Submitted By: Ma. Therese P. Ballares BSN 2 - NCMaria ThereseNo ratings yet
- Physical AssessmentDocument14 pagesPhysical AssessmentMaria ThereseNo ratings yet
- Gyne Case StudyDocument46 pagesGyne Case StudyMaria Therese100% (1)
- Pedia Case StudyDocument55 pagesPedia Case StudyMaria Therese100% (1)
- Physical AssessmentDocument37 pagesPhysical AssessmentMaria ThereseNo ratings yet
- Brain Drain Concept PaperDocument4 pagesBrain Drain Concept PaperMaria ThereseNo ratings yet
- LEC ArticleDocument2 pagesLEC ArticleMaria ThereseNo ratings yet
- OB Case StudyDocument52 pagesOB Case StudyMaria ThereseNo ratings yet
- LEC Gallery WalkDocument1 pageLEC Gallery WalkMaria ThereseNo ratings yet
- Adequacy of Scrubbing, Gowning and Gloving Among Operating Room NursesDocument4 pagesAdequacy of Scrubbing, Gowning and Gloving Among Operating Room NursesMaria ThereseNo ratings yet
- Share RateDocument26 pagesShare Ratevirtualpop3No ratings yet
- Supply and DemandDocument9 pagesSupply and DemandKulfi BarfiNo ratings yet
- Out 9Document7 pagesOut 9Ilvita MayasariNo ratings yet
- Module 3 Fetal DevelopmentDocument7 pagesModule 3 Fetal DevelopmentRichel TalattagNo ratings yet
- Disturbances of CirculationDocument10 pagesDisturbances of CirculationSuhan HasanNo ratings yet
- Seventh Grade Circulatory SystemDocument8 pagesSeventh Grade Circulatory SystemCarlo MakilingNo ratings yet
- Myocardial Infarction Covid Heart Failure Quiz RLE 5-6-2021Document58 pagesMyocardial Infarction Covid Heart Failure Quiz RLE 5-6-2021MuhyeeSalaIdjadNo ratings yet
- O Level Biology Notes With SpecDocument66 pagesO Level Biology Notes With Specshaayaa71% (7)
- ParticipantManual ECATDocument74 pagesParticipantManual ECATMuhammad ArifinNo ratings yet
- EMBRYOLOGYDocument30 pagesEMBRYOLOGYMSc. PreviousNo ratings yet
- Labelling (Answers)Document12 pagesLabelling (Answers)红熊红熊No ratings yet
- Venepuncture Delegate Notes 0118Document27 pagesVenepuncture Delegate Notes 0118Rohit ShindeNo ratings yet
- TACNDocument20 pagesTACNthuypham652004No ratings yet
- First Quarterly Assessment in Science Grade 5 Sses Table of SpecificationDocument8 pagesFirst Quarterly Assessment in Science Grade 5 Sses Table of SpecificationJaquelyn GaluaNo ratings yet
- Biology 5090 12 Paper 1 Question Paper Mayjue 2013Document16 pagesBiology 5090 12 Paper 1 Question Paper Mayjue 2013Raja Muda Raja NgahNo ratings yet
- Chapter 1. Historical Perspective On The Development of Mechanical VentilationDocument2 pagesChapter 1. Historical Perspective On The Development of Mechanical VentilationHussam GujjarNo ratings yet
- Diabetic FootDocument13 pagesDiabetic FootSafoora RafeeqNo ratings yet
- Blood Supply of Long BonesDocument4 pagesBlood Supply of Long BonesmainehoonaNo ratings yet
- Biology Paper-2Document12 pagesBiology Paper-2sollu786_889163149No ratings yet
- 3j Cuci - The Circulatory System WorksheetDocument6 pages3j Cuci - The Circulatory System Worksheetcharmaine nwankwoNo ratings yet
- Periodical Test in Science 6Document4 pagesPeriodical Test in Science 6jocelynberlin100% (2)
- Structure of Blood Vessels - WorksheetDocument2 pagesStructure of Blood Vessels - WorksheetRamya MalariniNo ratings yet
- Circulatory SystemDocument30 pagesCirculatory SystemScheherazade CNo ratings yet