
Wooden Splinter Dermatitis, M. Chen & D. P. Sarma: Wooden Splinter Dermatitis - The Internet Journal of Dermatology. 2007 Volume 5 Number 2
Wooden Splinter Dermatitis, M. Chen & D. P. Sarma: Wooden Splinter Dermatitis - The Internet Journal of Dermatology. 2007 Volume 5 Number 2
You might also like
- Asme 19.2 1987Document145 pagesAsme 19.2 1987Popescu Alin100% (4)
- Docu58580 Data Protection Advisor 6.2 SP1 Data Collection Reference GuideDocument502 pagesDocu58580 Data Protection Advisor 6.2 SP1 Data Collection Reference GuideD_23_desNo ratings yet
- Wooden Splinter DermatitisDocument5 pagesWooden Splinter DermatitisDeba P SarmaNo ratings yet
- Fractura ExpuestaDocument5 pagesFractura ExpuestaCortanaNo ratings yet
- Orofacial Soft Tissue Injury and Wound HealingDocument38 pagesOrofacial Soft Tissue Injury and Wound HealingSabbir HossainNo ratings yet
- Paramedic Soft Tissue InjuryDocument60 pagesParamedic Soft Tissue InjuryPaulhotvw67100% (5)
- Wounds: DR - Mohanned A LshalahDocument4 pagesWounds: DR - Mohanned A Lshalahjohana_6647No ratings yet
- Burns 2Document40 pagesBurns 27vjkgkw29xNo ratings yet
- Wound CareDocument16 pagesWound CareJohn FredNo ratings yet
- Gyorgyi Szabo Classification and Management of WoundDocument50 pagesGyorgyi Szabo Classification and Management of WoundMatheis Laskar PelangiNo ratings yet
- Lecture Notes in Forensic Medicine Derrick Pounder 48pagesDocument48 pagesLecture Notes in Forensic Medicine Derrick Pounder 48pagesLuíza OpretzkaNo ratings yet
- 0 WoundDocument50 pages0 WoundMuhammad MakkiNo ratings yet
- Burn InjuryDocument7 pagesBurn InjuryPutriDundaNo ratings yet
- Environmental and Nutritional Factor in Disease: by Dr. Theresia Indah B, DRG., M.KesDocument48 pagesEnvironmental and Nutritional Factor in Disease: by Dr. Theresia Indah B, DRG., M.KesJay MNo ratings yet
- Acquired Perforating Osteoma CutisDocument5 pagesAcquired Perforating Osteoma CutisDeba P SarmaNo ratings yet
- Burn Injury PDFDocument82 pagesBurn Injury PDFFirras Salsabila100% (1)
- Safety (Wounds)Document32 pagesSafety (Wounds)kay_genius252No ratings yet
- Types of Burns ArticleDocument7 pagesTypes of Burns ArticleSeltri 'ceti' SeptianiNo ratings yet
- Wound CareDocument26 pagesWound CareRaymund Christopher Dela PeñaNo ratings yet
- Tinjauan Pustaka Incised WoundDocument12 pagesTinjauan Pustaka Incised WoundTria Ayoe SyuknaNo ratings yet
- Vetero-Legal WoundsDocument26 pagesVetero-Legal WoundsAhmadx Hassan100% (4)
- 4.wound Care IDocument46 pages4.wound Care Iamir aizatNo ratings yet
- Question Answer of Surgery Mbbs Supplementary 1st Paper CDocument296 pagesQuestion Answer of Surgery Mbbs Supplementary 1st Paper CShivam AgarwalNo ratings yet
- Types of Wounds, Soft Tissue Injuries: ClassificationDocument64 pagesTypes of Wounds, Soft Tissue Injuries: ClassificationAli ImranNo ratings yet
- Advances A. BackgroundDocument24 pagesAdvances A. Backgroundalistia andiniNo ratings yet
- AMPUTATIONDocument73 pagesAMPUTATIONmohammad farhanNo ratings yet
- Penetrating Skull Fracture by A Wooden Object: Management Dilemmas and Literature ReviewDocument4 pagesPenetrating Skull Fracture by A Wooden Object: Management Dilemmas and Literature ReviewMeycha Da FhonsaNo ratings yet
- Extensive Actinomycetoma Clinical Manifestations and Histopathology 'A Case Report'Document8 pagesExtensive Actinomycetoma Clinical Manifestations and Histopathology 'A Case Report'irvan osakaNo ratings yet
- Polytrauma Lesson PlanDocument32 pagesPolytrauma Lesson PlanSwapnil MahapureNo ratings yet
- Surgery - Principle of Wound Healing and ManagementDocument39 pagesSurgery - Principle of Wound Healing and Managementjue_mardhiahNo ratings yet
- Anatomoclinical Confrontation Between Melanoma, Solar Lentigo and Seborrheic Keratosis: A Case ReportDocument4 pagesAnatomoclinical Confrontation Between Melanoma, Solar Lentigo and Seborrheic Keratosis: A Case ReportIJAR JOURNALNo ratings yet
- Introduction To BurnsDocument47 pagesIntroduction To BurnsanushavergheseNo ratings yet
- A Wound Is A Break in The Continuity of A Tissue of The BodyDocument6 pagesA Wound Is A Break in The Continuity of A Tissue of The BodyChristine Katherine LibuitNo ratings yet
- Wounds and InflammationsDocument55 pagesWounds and Inflammationsthelmaosei15No ratings yet
- Classification of Injuries FMTDocument30 pagesClassification of Injuries FMTkhadzx100% (2)
- Integumentary System: Burns and Wounds Clinical Case Study: Degree Burn Depth in Dermal Layers Description ImageDocument6 pagesIntegumentary System: Burns and Wounds Clinical Case Study: Degree Burn Depth in Dermal Layers Description ImageGabrielitoNo ratings yet
- Medico Legal Aspect of InjuryDocument24 pagesMedico Legal Aspect of InjuryCharmed Pineda Babayo100% (1)
- Case Pres PartDocument12 pagesCase Pres PartJeannezelle Anne Mariz GazaNo ratings yet
- Surgery, General, Wounds and Wound HealingDocument15 pagesSurgery, General, Wounds and Wound HealingRhazes78100% (1)
- Orofacial Soft Tissue Injury and Wound HealingDocument27 pagesOrofacial Soft Tissue Injury and Wound Healingsami azadNo ratings yet
- SDL 2 Wound and Wound HealingDocument4 pagesSDL 2 Wound and Wound HealingDn Ezrinah Dn EshamNo ratings yet
- Cat BiteDocument7 pagesCat BiteFitri Pite SiNo ratings yet
- Types & Causes of Open WoundsDocument3 pagesTypes & Causes of Open WoundsmArLoNNo ratings yet
- Cdi-2 Quiz 1 MidDocument5 pagesCdi-2 Quiz 1 Midangelo macalongNo ratings yet
- 1 s2.0 S0263931921002404 MainDocument8 pages1 s2.0 S0263931921002404 MainMarina UlfaNo ratings yet
- IJAMSCR 14 221 Pawan MittalDocument5 pagesIJAMSCR 14 221 Pawan MittalMarcoAngeloLiwanNo ratings yet
- Written Output Group 4 BurnsDocument55 pagesWritten Output Group 4 BurnsKean Debert SaladagaNo ratings yet
- Pediatric Fractures: The Exhibitors AreDocument5 pagesPediatric Fractures: The Exhibitors AreLaura OrozcoNo ratings yet
- Oral Ondansetron For Gastroenteritis in A Pediatric Emergency DepartmentDocument7 pagesOral Ondansetron For Gastroenteritis in A Pediatric Emergency DepartmentshaerizzeNo ratings yet
- Forensic PathologyDocument3 pagesForensic PathologyjmosserNo ratings yet
- Burn Terapi Topikal 1Document75 pagesBurn Terapi Topikal 1Mohamad Rizki DwikaneNo ratings yet
- MedicoDocument3 pagesMedicoATOLBA, Rizel D.No ratings yet
- Open FractureDocument9 pagesOpen FractureAnnyl LaurelNo ratings yet
- BurnDocument47 pagesBurnJoanna EdenNo ratings yet
- 223 2nd ExamDocument28 pages223 2nd ExamJohnzkie Gonzales123No ratings yet
- Medico-Legal Aspects of Physical InjuriesDocument9 pagesMedico-Legal Aspects of Physical InjuriesRhem Rick Corpuz100% (1)
- Surgery - Lect.1Document12 pagesSurgery - Lect.1sohaib197No ratings yet
- Medical Jurisprudence - Iat IiDocument2 pagesMedical Jurisprudence - Iat IiAadhithya KrishnanNo ratings yet
- Suspected Brown Recluse EnvenomationDocument7 pagesSuspected Brown Recluse EnvenomationCamelia AlexandraNo ratings yet
- Dermatology Notes for Medical StudentsFrom EverandDermatology Notes for Medical StudentsRating: 4 out of 5 stars4/5 (5)
- Pilar Cyst With CrystalsDocument2 pagesPilar Cyst With CrystalsDeba P SarmaNo ratings yet
- Acantholytic Dermatosis With DyskeratosisDocument11 pagesAcantholytic Dermatosis With DyskeratosisDeba P SarmaNo ratings yet
- Acantholytic Solar Keratosis, M 67, Forehead PDFDocument6 pagesAcantholytic Solar Keratosis, M 67, Forehead PDFDeba P SarmaNo ratings yet
- Acantholytic Bullous DiseaseDocument4 pagesAcantholytic Bullous DiseaseDeba P SarmaNo ratings yet
- Accessory TragusDocument3 pagesAccessory TragusDeba P SarmaNo ratings yet
- Acantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Document3 pagesAcantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Deba P SarmaNo ratings yet
- Xanthogranuloma PPT DSDocument9 pagesXanthogranuloma PPT DSDeba P SarmaNo ratings yet
- Acantholytic Acanthoma. M 60, ScrotumDocument8 pagesAcantholytic Acanthoma. M 60, ScrotumDeba P SarmaNo ratings yet
- Acantholytic Actinic KeratosisDocument4 pagesAcantholytic Actinic KeratosisDeba P SarmaNo ratings yet
- Results of Search in Google Scholar On 'Deba P Sarma'Document28 pagesResults of Search in Google Scholar On 'Deba P Sarma'Deba P SarmaNo ratings yet
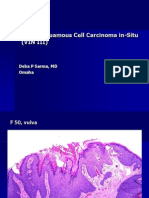
- Vulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDocument6 pagesVulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDeba P SarmaNo ratings yet
- Balanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Document6 pagesBalanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Deba P SarmaNo ratings yet
- Xanthogranuloma, M 30, Right ElbowDocument4 pagesXanthogranuloma, M 30, Right ElbowDeba P SarmaNo ratings yet
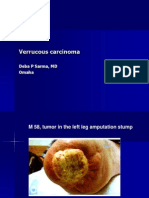
- Verrucous Carcinoma., M 58, Left Leg Amputation StumpDocument7 pagesVerrucous Carcinoma., M 58, Left Leg Amputation StumpDeba P SarmaNo ratings yet
- Xanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDocument7 pagesXanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDeba P SarmaNo ratings yet
- Verrucous Epidermal Nevus. F 43, ScalpDocument4 pagesVerrucous Epidermal Nevus. F 43, ScalpDeba P SarmaNo ratings yet
- Verrucous Carcinoma of The Foot, M 63, Left FootDocument8 pagesVerrucous Carcinoma of The Foot, M 63, Left FootDeba P Sarma100% (1)
- Verruca Vulgaris., M 22.,PPTDocument2 pagesVerruca Vulgaris., M 22.,PPTDeba P SarmaNo ratings yet
- Material: Lecture-10 Mian Ahmad Farhan (ACA)Document27 pagesMaterial: Lecture-10 Mian Ahmad Farhan (ACA)mc190402450 HASSAN AMIRNo ratings yet
- Philippine History Chapter 23: The Third Philippine RebuplicDocument20 pagesPhilippine History Chapter 23: The Third Philippine RebuplicAnnie Vinoray Balmaceda43% (7)
- Qualitative Research Synthesis and ReflectionDocument20 pagesQualitative Research Synthesis and ReflectionDun SusuNo ratings yet
- MCS052Document8 pagesMCS052AasNo ratings yet
- RULE 69 Partition CasesDocument43 pagesRULE 69 Partition CasesSamantha ReyesNo ratings yet
- Detailed Profile - Mashahed Hassan Simanta (Bangladesh) - 2024Document17 pagesDetailed Profile - Mashahed Hassan Simanta (Bangladesh) - 2024Mohetosh KantiNo ratings yet
- Worksheet - 1: Diversity in Living OrganismsDocument6 pagesWorksheet - 1: Diversity in Living OrganismsDharmendra SinghNo ratings yet
- Urea Cycle DisordersDocument23 pagesUrea Cycle DisordersIsabela BurculetNo ratings yet
- Vacancy Announcement (/2021 Advertisement) - Reannouncement!Document7 pagesVacancy Announcement (/2021 Advertisement) - Reannouncement!Htet Lynn HtunNo ratings yet
- Feeding A BudgieDocument4 pagesFeeding A BudgieMd. Nazmul Hasan Reza ChowdhuryNo ratings yet
- Summer Holidays Homework Class - Xi (Science) : Dear ParentDocument14 pagesSummer Holidays Homework Class - Xi (Science) : Dear ParentEr. ShivamNo ratings yet
- The CollarDocument2 pagesThe CollarlosoloresNo ratings yet
- Dlom Analysis Presentation From The IRS 2009Document116 pagesDlom Analysis Presentation From The IRS 2009Michael Cannon100% (1)
- Narrative Perspective AFDocument1 pageNarrative Perspective AFAngel AndersonNo ratings yet
- NSTPDocument2 pagesNSTPahppLe07No ratings yet
- Pearson Chemistry TeachingDocument67 pagesPearson Chemistry TeachingZheng JoeyNo ratings yet
- Sivapuranam Lyrics in English With MeaningDocument12 pagesSivapuranam Lyrics in English With MeaningRaman MohanadasNo ratings yet
- Science Fiction EssayDocument5 pagesScience Fiction Essayyezfvwwhd100% (2)
- Note 8 Electric Actuators: Lecture Notes of ME 475: Introduction To MechatronicsDocument13 pagesNote 8 Electric Actuators: Lecture Notes of ME 475: Introduction To MechatronicsSapath Narsingh BogatiNo ratings yet
- The Analysis of Organizational Culture For Improving Corporate Performance at PT. XYZ DiscreetDocument10 pagesThe Analysis of Organizational Culture For Improving Corporate Performance at PT. XYZ DiscreetTsweeg OnlineNo ratings yet
- Harnack A. - Marcion. The Gospel of The Alien GodDocument186 pagesHarnack A. - Marcion. The Gospel of The Alien GodDomenico CatalanoNo ratings yet
- Using Perl 6Document133 pagesUsing Perl 6Hussain AhmedNo ratings yet
- Wireless Networks - 802.11Document43 pagesWireless Networks - 802.11Pranali ChavanNo ratings yet
- AXA Report 2007Document480 pagesAXA Report 2007dindaaynNo ratings yet
- Judicial Activism Draft1Document15 pagesJudicial Activism Draft1vijay sathyaNo ratings yet
- Lab 13 Marshall Mix DesignDocument32 pagesLab 13 Marshall Mix DesignOtomen Yan Yan100% (9)
- Teaching Practice-ELT619: Assignment 4-Week 3 Lesson Plan Spring 2020 Total Marks: 5 6 - 30Document6 pagesTeaching Practice-ELT619: Assignment 4-Week 3 Lesson Plan Spring 2020 Total Marks: 5 6 - 30waqar javaid0% (1)
- Anti-Sexual Harrassment ActDocument30 pagesAnti-Sexual Harrassment ActJ Velasco PeraltaNo ratings yet










































































































Download as pdf or txt
You might also like
- Asme 19.2 1987Document145 pagesAsme 19.2 1987Popescu Alin100% (4)
- Docu58580 Data Protection Advisor 6.2 SP1 Data Collection Reference GuideDocument502 pagesDocu58580 Data Protection Advisor 6.2 SP1 Data Collection Reference GuideD_23_desNo ratings yet
- Wooden Splinter DermatitisDocument5 pagesWooden Splinter DermatitisDeba P SarmaNo ratings yet
- Fractura ExpuestaDocument5 pagesFractura ExpuestaCortanaNo ratings yet
- Orofacial Soft Tissue Injury and Wound HealingDocument38 pagesOrofacial Soft Tissue Injury and Wound HealingSabbir HossainNo ratings yet
- Paramedic Soft Tissue InjuryDocument60 pagesParamedic Soft Tissue InjuryPaulhotvw67100% (5)
- Wounds: DR - Mohanned A LshalahDocument4 pagesWounds: DR - Mohanned A Lshalahjohana_6647No ratings yet
- Burns 2Document40 pagesBurns 27vjkgkw29xNo ratings yet
- Wound CareDocument16 pagesWound CareJohn FredNo ratings yet
- Gyorgyi Szabo Classification and Management of WoundDocument50 pagesGyorgyi Szabo Classification and Management of WoundMatheis Laskar PelangiNo ratings yet
- Lecture Notes in Forensic Medicine Derrick Pounder 48pagesDocument48 pagesLecture Notes in Forensic Medicine Derrick Pounder 48pagesLuíza OpretzkaNo ratings yet
- 0 WoundDocument50 pages0 WoundMuhammad MakkiNo ratings yet
- Burn InjuryDocument7 pagesBurn InjuryPutriDundaNo ratings yet
- Environmental and Nutritional Factor in Disease: by Dr. Theresia Indah B, DRG., M.KesDocument48 pagesEnvironmental and Nutritional Factor in Disease: by Dr. Theresia Indah B, DRG., M.KesJay MNo ratings yet
- Acquired Perforating Osteoma CutisDocument5 pagesAcquired Perforating Osteoma CutisDeba P SarmaNo ratings yet
- Burn Injury PDFDocument82 pagesBurn Injury PDFFirras Salsabila100% (1)
- Safety (Wounds)Document32 pagesSafety (Wounds)kay_genius252No ratings yet
- Types of Burns ArticleDocument7 pagesTypes of Burns ArticleSeltri 'ceti' SeptianiNo ratings yet
- Wound CareDocument26 pagesWound CareRaymund Christopher Dela PeñaNo ratings yet
- Tinjauan Pustaka Incised WoundDocument12 pagesTinjauan Pustaka Incised WoundTria Ayoe SyuknaNo ratings yet
- Vetero-Legal WoundsDocument26 pagesVetero-Legal WoundsAhmadx Hassan100% (4)
- 4.wound Care IDocument46 pages4.wound Care Iamir aizatNo ratings yet
- Question Answer of Surgery Mbbs Supplementary 1st Paper CDocument296 pagesQuestion Answer of Surgery Mbbs Supplementary 1st Paper CShivam AgarwalNo ratings yet
- Types of Wounds, Soft Tissue Injuries: ClassificationDocument64 pagesTypes of Wounds, Soft Tissue Injuries: ClassificationAli ImranNo ratings yet
- Advances A. BackgroundDocument24 pagesAdvances A. Backgroundalistia andiniNo ratings yet
- AMPUTATIONDocument73 pagesAMPUTATIONmohammad farhanNo ratings yet
- Penetrating Skull Fracture by A Wooden Object: Management Dilemmas and Literature ReviewDocument4 pagesPenetrating Skull Fracture by A Wooden Object: Management Dilemmas and Literature ReviewMeycha Da FhonsaNo ratings yet
- Extensive Actinomycetoma Clinical Manifestations and Histopathology 'A Case Report'Document8 pagesExtensive Actinomycetoma Clinical Manifestations and Histopathology 'A Case Report'irvan osakaNo ratings yet
- Polytrauma Lesson PlanDocument32 pagesPolytrauma Lesson PlanSwapnil MahapureNo ratings yet
- Surgery - Principle of Wound Healing and ManagementDocument39 pagesSurgery - Principle of Wound Healing and Managementjue_mardhiahNo ratings yet
- Anatomoclinical Confrontation Between Melanoma, Solar Lentigo and Seborrheic Keratosis: A Case ReportDocument4 pagesAnatomoclinical Confrontation Between Melanoma, Solar Lentigo and Seborrheic Keratosis: A Case ReportIJAR JOURNALNo ratings yet
- Introduction To BurnsDocument47 pagesIntroduction To BurnsanushavergheseNo ratings yet
- A Wound Is A Break in The Continuity of A Tissue of The BodyDocument6 pagesA Wound Is A Break in The Continuity of A Tissue of The BodyChristine Katherine LibuitNo ratings yet
- Wounds and InflammationsDocument55 pagesWounds and Inflammationsthelmaosei15No ratings yet
- Classification of Injuries FMTDocument30 pagesClassification of Injuries FMTkhadzx100% (2)
- Integumentary System: Burns and Wounds Clinical Case Study: Degree Burn Depth in Dermal Layers Description ImageDocument6 pagesIntegumentary System: Burns and Wounds Clinical Case Study: Degree Burn Depth in Dermal Layers Description ImageGabrielitoNo ratings yet
- Medico Legal Aspect of InjuryDocument24 pagesMedico Legal Aspect of InjuryCharmed Pineda Babayo100% (1)
- Case Pres PartDocument12 pagesCase Pres PartJeannezelle Anne Mariz GazaNo ratings yet
- Surgery, General, Wounds and Wound HealingDocument15 pagesSurgery, General, Wounds and Wound HealingRhazes78100% (1)
- Orofacial Soft Tissue Injury and Wound HealingDocument27 pagesOrofacial Soft Tissue Injury and Wound Healingsami azadNo ratings yet
- SDL 2 Wound and Wound HealingDocument4 pagesSDL 2 Wound and Wound HealingDn Ezrinah Dn EshamNo ratings yet
- Cat BiteDocument7 pagesCat BiteFitri Pite SiNo ratings yet
- Types & Causes of Open WoundsDocument3 pagesTypes & Causes of Open WoundsmArLoNNo ratings yet
- Cdi-2 Quiz 1 MidDocument5 pagesCdi-2 Quiz 1 Midangelo macalongNo ratings yet
- 1 s2.0 S0263931921002404 MainDocument8 pages1 s2.0 S0263931921002404 MainMarina UlfaNo ratings yet
- IJAMSCR 14 221 Pawan MittalDocument5 pagesIJAMSCR 14 221 Pawan MittalMarcoAngeloLiwanNo ratings yet
- Written Output Group 4 BurnsDocument55 pagesWritten Output Group 4 BurnsKean Debert SaladagaNo ratings yet
- Pediatric Fractures: The Exhibitors AreDocument5 pagesPediatric Fractures: The Exhibitors AreLaura OrozcoNo ratings yet
- Oral Ondansetron For Gastroenteritis in A Pediatric Emergency DepartmentDocument7 pagesOral Ondansetron For Gastroenteritis in A Pediatric Emergency DepartmentshaerizzeNo ratings yet
- Forensic PathologyDocument3 pagesForensic PathologyjmosserNo ratings yet
- Burn Terapi Topikal 1Document75 pagesBurn Terapi Topikal 1Mohamad Rizki DwikaneNo ratings yet
- MedicoDocument3 pagesMedicoATOLBA, Rizel D.No ratings yet
- Open FractureDocument9 pagesOpen FractureAnnyl LaurelNo ratings yet
- BurnDocument47 pagesBurnJoanna EdenNo ratings yet
- 223 2nd ExamDocument28 pages223 2nd ExamJohnzkie Gonzales123No ratings yet
- Medico-Legal Aspects of Physical InjuriesDocument9 pagesMedico-Legal Aspects of Physical InjuriesRhem Rick Corpuz100% (1)
- Surgery - Lect.1Document12 pagesSurgery - Lect.1sohaib197No ratings yet
- Medical Jurisprudence - Iat IiDocument2 pagesMedical Jurisprudence - Iat IiAadhithya KrishnanNo ratings yet
- Suspected Brown Recluse EnvenomationDocument7 pagesSuspected Brown Recluse EnvenomationCamelia AlexandraNo ratings yet
- Dermatology Notes for Medical StudentsFrom EverandDermatology Notes for Medical StudentsRating: 4 out of 5 stars4/5 (5)
- Pilar Cyst With CrystalsDocument2 pagesPilar Cyst With CrystalsDeba P SarmaNo ratings yet
- Acantholytic Dermatosis With DyskeratosisDocument11 pagesAcantholytic Dermatosis With DyskeratosisDeba P SarmaNo ratings yet
- Acantholytic Solar Keratosis, M 67, Forehead PDFDocument6 pagesAcantholytic Solar Keratosis, M 67, Forehead PDFDeba P SarmaNo ratings yet
- Acantholytic Bullous DiseaseDocument4 pagesAcantholytic Bullous DiseaseDeba P SarmaNo ratings yet
- Accessory TragusDocument3 pagesAccessory TragusDeba P SarmaNo ratings yet
- Acantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Document3 pagesAcantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Deba P SarmaNo ratings yet
- Xanthogranuloma PPT DSDocument9 pagesXanthogranuloma PPT DSDeba P SarmaNo ratings yet
- Acantholytic Acanthoma. M 60, ScrotumDocument8 pagesAcantholytic Acanthoma. M 60, ScrotumDeba P SarmaNo ratings yet
- Acantholytic Actinic KeratosisDocument4 pagesAcantholytic Actinic KeratosisDeba P SarmaNo ratings yet
- Results of Search in Google Scholar On 'Deba P Sarma'Document28 pagesResults of Search in Google Scholar On 'Deba P Sarma'Deba P SarmaNo ratings yet
- Vulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDocument6 pagesVulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDeba P SarmaNo ratings yet
- Balanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Document6 pagesBalanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Deba P SarmaNo ratings yet
- Xanthogranuloma, M 30, Right ElbowDocument4 pagesXanthogranuloma, M 30, Right ElbowDeba P SarmaNo ratings yet
- Verrucous Carcinoma., M 58, Left Leg Amputation StumpDocument7 pagesVerrucous Carcinoma., M 58, Left Leg Amputation StumpDeba P SarmaNo ratings yet
- Xanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDocument7 pagesXanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDeba P SarmaNo ratings yet
- Verrucous Epidermal Nevus. F 43, ScalpDocument4 pagesVerrucous Epidermal Nevus. F 43, ScalpDeba P SarmaNo ratings yet
- Verrucous Carcinoma of The Foot, M 63, Left FootDocument8 pagesVerrucous Carcinoma of The Foot, M 63, Left FootDeba P Sarma100% (1)
- Verruca Vulgaris., M 22.,PPTDocument2 pagesVerruca Vulgaris., M 22.,PPTDeba P SarmaNo ratings yet
- Material: Lecture-10 Mian Ahmad Farhan (ACA)Document27 pagesMaterial: Lecture-10 Mian Ahmad Farhan (ACA)mc190402450 HASSAN AMIRNo ratings yet
- Philippine History Chapter 23: The Third Philippine RebuplicDocument20 pagesPhilippine History Chapter 23: The Third Philippine RebuplicAnnie Vinoray Balmaceda43% (7)
- Qualitative Research Synthesis and ReflectionDocument20 pagesQualitative Research Synthesis and ReflectionDun SusuNo ratings yet
- MCS052Document8 pagesMCS052AasNo ratings yet
- RULE 69 Partition CasesDocument43 pagesRULE 69 Partition CasesSamantha ReyesNo ratings yet
- Detailed Profile - Mashahed Hassan Simanta (Bangladesh) - 2024Document17 pagesDetailed Profile - Mashahed Hassan Simanta (Bangladesh) - 2024Mohetosh KantiNo ratings yet
- Worksheet - 1: Diversity in Living OrganismsDocument6 pagesWorksheet - 1: Diversity in Living OrganismsDharmendra SinghNo ratings yet
- Urea Cycle DisordersDocument23 pagesUrea Cycle DisordersIsabela BurculetNo ratings yet
- Vacancy Announcement (/2021 Advertisement) - Reannouncement!Document7 pagesVacancy Announcement (/2021 Advertisement) - Reannouncement!Htet Lynn HtunNo ratings yet
- Feeding A BudgieDocument4 pagesFeeding A BudgieMd. Nazmul Hasan Reza ChowdhuryNo ratings yet
- Summer Holidays Homework Class - Xi (Science) : Dear ParentDocument14 pagesSummer Holidays Homework Class - Xi (Science) : Dear ParentEr. ShivamNo ratings yet
- The CollarDocument2 pagesThe CollarlosoloresNo ratings yet
- Dlom Analysis Presentation From The IRS 2009Document116 pagesDlom Analysis Presentation From The IRS 2009Michael Cannon100% (1)
- Narrative Perspective AFDocument1 pageNarrative Perspective AFAngel AndersonNo ratings yet
- NSTPDocument2 pagesNSTPahppLe07No ratings yet
- Pearson Chemistry TeachingDocument67 pagesPearson Chemistry TeachingZheng JoeyNo ratings yet
- Sivapuranam Lyrics in English With MeaningDocument12 pagesSivapuranam Lyrics in English With MeaningRaman MohanadasNo ratings yet
- Science Fiction EssayDocument5 pagesScience Fiction Essayyezfvwwhd100% (2)
- Note 8 Electric Actuators: Lecture Notes of ME 475: Introduction To MechatronicsDocument13 pagesNote 8 Electric Actuators: Lecture Notes of ME 475: Introduction To MechatronicsSapath Narsingh BogatiNo ratings yet
- The Analysis of Organizational Culture For Improving Corporate Performance at PT. XYZ DiscreetDocument10 pagesThe Analysis of Organizational Culture For Improving Corporate Performance at PT. XYZ DiscreetTsweeg OnlineNo ratings yet
- Harnack A. - Marcion. The Gospel of The Alien GodDocument186 pagesHarnack A. - Marcion. The Gospel of The Alien GodDomenico CatalanoNo ratings yet
- Using Perl 6Document133 pagesUsing Perl 6Hussain AhmedNo ratings yet
- Wireless Networks - 802.11Document43 pagesWireless Networks - 802.11Pranali ChavanNo ratings yet
- AXA Report 2007Document480 pagesAXA Report 2007dindaaynNo ratings yet
- Judicial Activism Draft1Document15 pagesJudicial Activism Draft1vijay sathyaNo ratings yet
- Lab 13 Marshall Mix DesignDocument32 pagesLab 13 Marshall Mix DesignOtomen Yan Yan100% (9)
- Teaching Practice-ELT619: Assignment 4-Week 3 Lesson Plan Spring 2020 Total Marks: 5 6 - 30Document6 pagesTeaching Practice-ELT619: Assignment 4-Week 3 Lesson Plan Spring 2020 Total Marks: 5 6 - 30waqar javaid0% (1)
- Anti-Sexual Harrassment ActDocument30 pagesAnti-Sexual Harrassment ActJ Velasco PeraltaNo ratings yet