Download as docx, pdf, or txt
You might also like
- A Case Study On Acute AppendicitisDocument56 pagesA Case Study On Acute AppendicitisIvy Mae Evangelio Vios92% (13)
- Esophageal AtresiaDocument18 pagesEsophageal AtresiaNeha RathoreNo ratings yet
- Pediatric Surgery MCQDocument8 pagesPediatric Surgery MCQMohamed Al-zichrawy100% (1)
- Hirschsprung Disease Case Study: Maecy P. Tarinay BSN 4-1Document5 pagesHirschsprung Disease Case Study: Maecy P. Tarinay BSN 4-1Maecy OdegaardNo ratings yet
- Melissa Kennedy, Chris A. LiacourasDocument3 pagesMelissa Kennedy, Chris A. LiacourasChristian LoyolaNo ratings yet
- Acute Abdominal Pain InInfants and ChildrenDocument14 pagesAcute Abdominal Pain InInfants and Childrenemergency.fumcNo ratings yet
- Intussuseption and Hirschprung's DiseaseDocument5 pagesIntussuseption and Hirschprung's DiseaseAris Magallanes100% (2)
- Hirschsprung DiseaseDocument25 pagesHirschsprung DiseaseMuhammad Zaniar RamadhaniNo ratings yet
- Acute AppendicitisDocument5 pagesAcute AppendicitisPrasetya Ismail PermadiNo ratings yet
- Intussusception PPTDocument29 pagesIntussusception PPTKathleen BalauagNo ratings yet
- Hirschsprung'S Disease (Megacolon) : Mrs. Smitha.M Associate Professor Vijaya College of Nursing KottarakkaraDocument6 pagesHirschsprung'S Disease (Megacolon) : Mrs. Smitha.M Associate Professor Vijaya College of Nursing KottarakkarakrishnasreeNo ratings yet
- 19-Pediatric SurgeryDocument39 pages19-Pediatric Surgerycallisto3487No ratings yet
- Congenital Aganglionic Megacolon (Hirschsprung Disease) : Kristin N. Fiorino and Chris A. LiacourasDocument6 pagesCongenital Aganglionic Megacolon (Hirschsprung Disease) : Kristin N. Fiorino and Chris A. LiacourasSyakilla AuliaNo ratings yet
- AppendicitisDocument4 pagesAppendicitisFebriyana SalehNo ratings yet
- IntussusceptionDocument10 pagesIntussusceptionshenlie100% (1)
- Ov Ov OvDocument15 pagesOv Ov OvHayyana Mae Taguba LadiaNo ratings yet
- Ped Surg Mcqs 2Document24 pagesPed Surg Mcqs 2abdurrahman100% (1)
- 12 - Paediatric Abdomen RadiologyDocument74 pages12 - Paediatric Abdomen RadiologyMaria DoukaNo ratings yet
- Appendicitis: Differential Diagnoses & Workup Treatment & Medication Follow-UpDocument12 pagesAppendicitis: Differential Diagnoses & Workup Treatment & Medication Follow-UpnetonetinNo ratings yet
- IntussusceptionDocument2 pagesIntussusceptionjesagi88No ratings yet
- Hirschsprung Disease (Aganglionic Megacolon)Document6 pagesHirschsprung Disease (Aganglionic Megacolon)Julliza Joy PandiNo ratings yet
- Appendicitis CaseDocument8 pagesAppendicitis CaseStarr NewmanNo ratings yet
- 6INVAGINASIDocument18 pages6INVAGINASIhazelelNo ratings yet
- IntussusceptionDocument4 pagesIntussusceptionBlue TechNo ratings yet
- Patient Scenario, Chapter 45, Nursing Care of A Family When A Child Has A Gastrointestinal DisorderDocument93 pagesPatient Scenario, Chapter 45, Nursing Care of A Family When A Child Has A Gastrointestinal DisorderDay MedsNo ratings yet
- Chapter X.4. Intussusception: Case Based Pediatrics For Medical Students and ResidentsDocument5 pagesChapter X.4. Intussusception: Case Based Pediatrics For Medical Students and ResidentsNawaf Rahi AlshammariNo ratings yet
- Lec 1Document52 pagesLec 1zainabd1964No ratings yet
- Intraoperative Finding in Total Colonic AganglionosisDocument12 pagesIntraoperative Finding in Total Colonic AganglionosisAtrioventrikular MilanistiNo ratings yet
- Appendicitis Lec2023Document6 pagesAppendicitis Lec2023Taha MuhammedNo ratings yet
- Hirschsprun G'S Disease: Dr. Manish Kumar Gupta Assistant Professor Department of Paediatric Surgery AIIMS, RishikeshDocument48 pagesHirschsprun G'S Disease: Dr. Manish Kumar Gupta Assistant Professor Department of Paediatric Surgery AIIMS, RishikeshArchana Mahata100% (1)
- Congenital AnomaliesDocument10 pagesCongenital Anomaliesربيع ضياء ربيعNo ratings yet
- Pyloric Stenosis WDocument11 pagesPyloric Stenosis WKlaue Neiv CallaNo ratings yet
- لقطة شاشة 2022-04-21 في 11.10.40 صDocument55 pagesلقطة شاشة 2022-04-21 في 11.10.40 صEngi KazangyNo ratings yet
- Pyloric Stenosis ChibuezeDocument12 pagesPyloric Stenosis ChibuezeChibueze AfugbuomNo ratings yet
- Neonatal Acute Abdomen. 7th YrDocument54 pagesNeonatal Acute Abdomen. 7th YrFreeburn SimunchembuNo ratings yet
- Pediatric (S) 2023 Final 7th SemDocument226 pagesPediatric (S) 2023 Final 7th SemSyed NoorNo ratings yet
- Colon, Rectum and AnusDocument30 pagesColon, Rectum and AnusKiara GovenderNo ratings yet
- Afrisya Bimo Siwendro Marisha Yadian Putri Preceptor: DR - Liza Nursanty, Spb. FinacsDocument32 pagesAfrisya Bimo Siwendro Marisha Yadian Putri Preceptor: DR - Liza Nursanty, Spb. FinacsirmaNo ratings yet
- Appendicitis: Made By: Madhurpreet KaurDocument46 pagesAppendicitis: Made By: Madhurpreet KaurRAJAT DUGGALNo ratings yet
- Pyloric Stenosis: EpidemiologyDocument6 pagesPyloric Stenosis: EpidemiologyNeil AlviarNo ratings yet
- Neonates and Periparturient Mares 2023 VepDocument29 pagesNeonates and Periparturient Mares 2023 VepAristoteles Esteban Cine VelazquezNo ratings yet
- Peritonitis. Classifications. Open Abdomen and Staged Abdominal Repair.Document7 pagesPeritonitis. Classifications. Open Abdomen and Staged Abdominal Repair.Ibraheem SairiNo ratings yet
- Presentation - IntussusceptionDocument9 pagesPresentation - IntussusceptionAme NasokiaNo ratings yet
- 18-Month-Old Boy With Abdominal Pain and Rectal Bleeding BackgroundDocument5 pages18-Month-Old Boy With Abdominal Pain and Rectal Bleeding Backgroundcamille nina jane navarroNo ratings yet
- 20 PediatricDocument31 pages20 PediatricMahmoud AbuAwadNo ratings yet
- Intussusception - A Case ReportDocument3 pagesIntussusception - A Case ReportAgustinus HuangNo ratings yet
- Paediatric Surgery 2Document38 pagesPaediatric Surgery 2عمار عارفNo ratings yet
- Intussusception: PathophysiologyDocument8 pagesIntussusception: PathophysiologyNaufal AndaluNo ratings yet
- PBL No Bowel Output in NeonatesDocument24 pagesPBL No Bowel Output in NeonatesOTOH RAYA OMARNo ratings yet
- Heurn Et Al-2014-British Journal of Surgery-1Document10 pagesHeurn Et Al-2014-British Journal of Surgery-1sebastianNo ratings yet
- Pyloric StenosisDocument3 pagesPyloric Stenosismagisasamundo100% (1)
- AppendicitisDocument17 pagesAppendicitisAhmed Halaby100% (1)
- Nursing Care of The Child With A Gastrointestinal DisordersDocument46 pagesNursing Care of The Child With A Gastrointestinal Disorderstalaekrema01No ratings yet
- Gastroschisis - ClinicalKeyDocument33 pagesGastroschisis - ClinicalKeyjpma2197No ratings yet
- Presentation 1Document13 pagesPresentation 1Monica PramanaNo ratings yet
- Pyloric StenosisDocument47 pagesPyloric StenosisgeethsreesatNo ratings yet
- General Care of The (Peritonitis) Patient: Summary Box 58.1Document7 pagesGeneral Care of The (Peritonitis) Patient: Summary Box 58.1RadenJeremySoeriawidjajaNo ratings yet
- Case Series of Intussusception in Paediatric SurgeryDocument39 pagesCase Series of Intussusception in Paediatric SurgeryRajkiran AmbarapuNo ratings yet
- Tubular Ileal Duplication Causing Small Bowel Obstruction in A ChildDocument5 pagesTubular Ileal Duplication Causing Small Bowel Obstruction in A ChildDiego Leonardo Herrera OjedaNo ratings yet
- Intussuscept ION: in The Paediatric PatientDocument30 pagesIntussuscept ION: in The Paediatric PatientSuneil R AlsNo ratings yet
- Dysphagia, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandDysphagia, A Simple Guide To The Condition, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- 1 Urinary StonesDocument11 pages1 Urinary StonesMohamed Al-zichrawyNo ratings yet
- 1 ScrotumDocument7 pages1 ScrotumMohamed Al-zichrawyNo ratings yet
- Rheumatology and Bone DiseaseDocument32 pagesRheumatology and Bone DiseaseMohamed Al-zichrawyNo ratings yet
- Anomalies of The Upper Urinary TractDocument6 pagesAnomalies of The Upper Urinary TractMohamed Al-zichrawyNo ratings yet
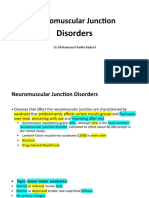
- Neuromuscular Junction Disorders - 1Document30 pagesNeuromuscular Junction Disorders - 1Mohamed Al-zichrawyNo ratings yet
- Renal Tumors RCC Renal Cells Carcinoma Renal Adenocarcinoma HypernephromaDocument5 pagesRenal Tumors RCC Renal Cells Carcinoma Renal Adenocarcinoma HypernephromaMohamed Al-zichrawyNo ratings yet
- Fibromyalgia: PathophysiologyDocument4 pagesFibromyalgia: PathophysiologyMohamed Al-zichrawyNo ratings yet
- Rheumatology and Bone DiseaseDocument8 pagesRheumatology and Bone DiseaseMohamed Al-zichrawyNo ratings yet
- Septic Arthritis: Clinical FeaturesDocument4 pagesSeptic Arthritis: Clinical FeaturesMohamed Al-zichrawyNo ratings yet
- Acute Pelvic Pain: HistoryDocument4 pagesAcute Pelvic Pain: HistoryMohamed Al-zichrawyNo ratings yet
- Smart Study مهم جداDocument328 pagesSmart Study مهم جداMohamed Al-zichrawy100% (2)
- Gyn MCQ ..Group E PDFDocument15 pagesGyn MCQ ..Group E PDFMohamed Al-zichrawyNo ratings yet
- Latest Gynecology Multiple Choice Questions and Answers For PDFDocument10 pagesLatest Gynecology Multiple Choice Questions and Answers For PDFMohamed Al-zichrawy100% (1)
- Chest+heart+medistinum RadiologyDocument4 pagesChest+heart+medistinum RadiologyMohamed Al-zichrawyNo ratings yet
- Cerebral Edema: BBB (Blood Brain Barrier)Document4 pagesCerebral Edema: BBB (Blood Brain Barrier)Mohamed Al-zichrawyNo ratings yet
- Head Injury: Classification of Head Injury A-Scalp Injuries B-Skull FracturesDocument6 pagesHead Injury: Classification of Head Injury A-Scalp Injuries B-Skull FracturesMohamed Al-zichrawyNo ratings yet
- 5 Congenital Malformation (Continue)Document4 pages5 Congenital Malformation (Continue)Mohamed Al-zichrawyNo ratings yet
- Neurological Assessment in Head Trauma: 1-Vital Sign MonitoringDocument4 pagesNeurological Assessment in Head Trauma: 1-Vital Sign MonitoringMohamed Al-zichrawyNo ratings yet
- Brain Tumors: Primary BTDocument5 pagesBrain Tumors: Primary BTMohamed Al-zichrawyNo ratings yet
- Thalassemia Syndromes: Clinical Features and ComplicationsDocument22 pagesThalassemia Syndromes: Clinical Features and ComplicationsMohamed Al-zichrawyNo ratings yet
- Quiz 1 Med Surg SummerDocument8 pagesQuiz 1 Med Surg SummerMc Harris VinasoyNo ratings yet
- Gastrointestinal Bleeding in NewbornDocument28 pagesGastrointestinal Bleeding in NewbornHafiz AwaisNo ratings yet
- Laxatives AND Antidiarrheals: DR Mohd Suhaimi Jabatan FarmakologiDocument31 pagesLaxatives AND Antidiarrheals: DR Mohd Suhaimi Jabatan FarmakologiChokJunHoongNo ratings yet
- Diverticular Disease and Diverticulitis: Anish A. Sheth, M.D., Walter Longo, M.D., and Martin H. Floch, M.DDocument7 pagesDiverticular Disease and Diverticulitis: Anish A. Sheth, M.D., Walter Longo, M.D., and Martin H. Floch, M.DIrma Suriani DarwisNo ratings yet
- Delayed Passage of MeconiumDocument15 pagesDelayed Passage of MeconiumMohammed Ezz El RegalNo ratings yet
- Cleft Lip-Palate KhambhatDocument6 pagesCleft Lip-Palate KhambhatSachinsinh DhummadNo ratings yet
- E2 Pendaftaran Income Harian 16 November 2023Document169 pagesE2 Pendaftaran Income Harian 16 November 2023Dede Yudi SatriaNo ratings yet
- Proctitis Is Inflammation of The Lining of The RectumDocument2 pagesProctitis Is Inflammation of The Lining of The RectumEllysabet DianNo ratings yet
- English TaskDocument5 pagesEnglish Taskshelly70514576No ratings yet
- Lower GI BleedingDocument3 pagesLower GI BleedingTaleb AliNo ratings yet
- Postop Drug2Document3 pagesPostop Drug2zbestgurlNo ratings yet
- Bowel Obstruction - ppt1Document30 pagesBowel Obstruction - ppt1Elfrida Aulia100% (1)
- Internal MedicineDocument195 pagesInternal Medicineصقر حورانNo ratings yet
- Inflammatory Bowel Diseases: Dr. Evelyn Angie M. BiomedDocument36 pagesInflammatory Bowel Diseases: Dr. Evelyn Angie M. BiomedAnnis100% (1)
- TM RepsDocument21 pagesTM Repsdrae syNo ratings yet
- Separate Hard Lumps, Like Nuts: Constipated Stool - Types 1 or 2 Diarrheal Stool - Types 6 or 7Document2 pagesSeparate Hard Lumps, Like Nuts: Constipated Stool - Types 1 or 2 Diarrheal Stool - Types 6 or 7nicky_lauw5885No ratings yet
- Upper Gastrointestinal BleedingDocument3 pagesUpper Gastrointestinal BleedingcheyzerrlNo ratings yet
- Laporan-Diagnosa Januari 2021Document231 pagesLaporan-Diagnosa Januari 2021Putri AnnisaNo ratings yet
- Recognizing SBO, LBO and IleusDocument51 pagesRecognizing SBO, LBO and IleusLanny Dwi ChandraNo ratings yet
- 20-Year History of Diarrhea With Intermittent ConstipationDocument2 pages20-Year History of Diarrhea With Intermittent Constipationhossein kasiriNo ratings yet
- Radiology of Gastrointestinal Tract: (GIT) Bachtiar MurtalaDocument53 pagesRadiology of Gastrointestinal Tract: (GIT) Bachtiar MurtalaMichael HusainNo ratings yet
- 14 - Barium Studies For GIT With NotesDocument50 pages14 - Barium Studies For GIT With NotesSunil ThomasNo ratings yet
- Upper Gastrointestinal BleedingDocument7 pagesUpper Gastrointestinal BleedingironNo ratings yet
- S10 PII Procineticos T-Dra PajueloDocument36 pagesS10 PII Procineticos T-Dra PajueloMarllo RoggeroNo ratings yet
- Lower Gastrointestinal Bleeding (LGIB)Document41 pagesLower Gastrointestinal Bleeding (LGIB)api-196413370% (1)
- ColitisDocument2 pagesColitisyuvi087No ratings yet
- Daftar Pustaka: Option Com - Journal - Review&idDocument2 pagesDaftar Pustaka: Option Com - Journal - Review&idYogi OktiandiNo ratings yet
- Sindroma Dispepsia: Dr. Rifqa RahmiDocument36 pagesSindroma Dispepsia: Dr. Rifqa RahmiK-gant ParasitNo ratings yet
- Drug Study - LactuloseDocument2 pagesDrug Study - LactuloseCath Bril100% (1)
- Internal Medicine II II MidtermDocument11 pagesInternal Medicine II II MidtermJerin XavierNo ratings yet