Download as docx, pdf, or txt
You might also like
- Gentile 2013Document18 pagesGentile 2013Desi HemavianaNo ratings yet
- ConstipationDocument33 pagesConstipationsalmawalidNo ratings yet
- Pediatric Surgery MCQDocument8 pagesPediatric Surgery MCQMohamed Al-zichrawy100% (1)
- Professor Dr Francesco Capasso, Professor Dr Timothy S. Gaginella, Professor Dr Giuliano Grandolini, Professor Dr Angelo a. Izzo (Auth.)-Phytotherapy_ a Quick Reference to Herbal Medicine-Springer-VerDocument413 pagesProfessor Dr Francesco Capasso, Professor Dr Timothy S. Gaginella, Professor Dr Giuliano Grandolini, Professor Dr Angelo a. Izzo (Auth.)-Phytotherapy_ a Quick Reference to Herbal Medicine-Springer-VerJesus Ignacio Briceño PrietoNo ratings yet
- For Hino: Tics Pump Electrical Part Resistance Value ListDocument35 pagesFor Hino: Tics Pump Electrical Part Resistance Value Listfersky90% (10)
- Pediatric EmergencyDocument66 pagesPediatric EmergencyWaseem MoukhtarNo ratings yet
- Pediatric Surgery Notes For NursesDocument8 pagesPediatric Surgery Notes For NursesAhmed SamyNo ratings yet
- 2.obstruction of The Urinary TractDocument22 pages2.obstruction of The Urinary TractAkli JahNo ratings yet
- Congenital Aganglionic Megacolon (Hirschsprung Disease) : Kristin N. Fiorino and Chris A. LiacourasDocument6 pagesCongenital Aganglionic Megacolon (Hirschsprung Disease) : Kristin N. Fiorino and Chris A. LiacourasSyakilla AuliaNo ratings yet
- Intestinal Obstruction in Pediatric SurgeryDocument69 pagesIntestinal Obstruction in Pediatric Surgeryabhinay_1712No ratings yet
- Cloacal MalformationsDocument6 pagesCloacal MalformationsRayhanun MardhatillahNo ratings yet
- HypospDocument39 pagesHypospyoussef.aziz2020No ratings yet
- Prune Belly SyndromeDocument39 pagesPrune Belly SyndromeHudaNo ratings yet
- Hirschsprun G'S Disease: Dr. Manish Kumar Gupta Assistant Professor Department of Paediatric Surgery AIIMS, RishikeshDocument48 pagesHirschsprun G'S Disease: Dr. Manish Kumar Gupta Assistant Professor Department of Paediatric Surgery AIIMS, RishikeshArchana Mahata100% (1)
- Congenital AnomaliesDocument10 pagesCongenital Anomaliesربيع ضياء ربيعNo ratings yet
- URINARY FACTSDocument3 pagesURINARY FACTSlcaguirreortegaNo ratings yet
- Anorectal MalformationDocument29 pagesAnorectal Malformationbimaindra97No ratings yet
- Pediatric Urology HDocument54 pagesPediatric Urology HAlaa A. AbdelrahimNo ratings yet
- Posterior Urethral ValveDocument6 pagesPosterior Urethral ValveMustafa AadanNo ratings yet
- Dr. Ghada Abu ShoshaDocument42 pagesDr. Ghada Abu Shoshatalaekrema01No ratings yet
- HidroceleDocument4 pagesHidroceleAnshy V. FreireNo ratings yet
- Hirschsprung Disease Case Study: Maecy P. Tarinay BSN 4-1Document5 pagesHirschsprung Disease Case Study: Maecy P. Tarinay BSN 4-1Maecy OdegaardNo ratings yet
- Urolithiasis, Acute ScrotumDocument29 pagesUrolithiasis, Acute Scrotumraed ganmNo ratings yet
- Renal AbnormalitiesDocument15 pagesRenal AbnormalitiesShambel NegeseNo ratings yet
- 04 NephrologyDocument19 pages04 NephrologyeuncieNo ratings yet
- Sick Growing Child: Hirschsprung Disease Anorectal Malformation Maluenda CamilleDocument46 pagesSick Growing Child: Hirschsprung Disease Anorectal Malformation Maluenda CamilleCamille Maluenda - TanNo ratings yet
- Neonatal Intestinal Obstruction EPSGHAN PDFDocument77 pagesNeonatal Intestinal Obstruction EPSGHAN PDFRobert ChristevenNo ratings yet
- Pemeriksaan Rontgen Toraks, Elektrokardiogram (EKG), USG Abdomen Dan EchocardiografiDocument5 pagesPemeriksaan Rontgen Toraks, Elektrokardiogram (EKG), USG Abdomen Dan EchocardiografigorodoeNo ratings yet
- Hirschprung DiseaseDocument9 pagesHirschprung DiseaseJonathan ObañaNo ratings yet
- Hirschprung DiseaseDocument61 pagesHirschprung DiseaseAdditi Satyal100% (1)
- Case 22: Total Colonic Aganglionosis - Long-Segment Hirschsprung DiseaseDocument4 pagesCase 22: Total Colonic Aganglionosis - Long-Segment Hirschsprung DiseaseRahmat MuliaNo ratings yet
- Hirschprung's DiseaseDocument26 pagesHirschprung's DiseaseAbdur RaqibNo ratings yet
- Jaundice in Infants and Children: Ultrasound ClinicsDocument11 pagesJaundice in Infants and Children: Ultrasound Clinics5206329No ratings yet
- Abdominal Wall DefectsDocument4 pagesAbdominal Wall Defectsbox officeNo ratings yet
- Abdominal X-Rays PT 1Document20 pagesAbdominal X-Rays PT 1sb medexNo ratings yet
- Ileal Atresia ReferenceDocument50 pagesIleal Atresia ReferenceOvamelia JulioNo ratings yet
- Sigmoid Volvulus (Autosaved)Document34 pagesSigmoid Volvulus (Autosaved)msichiliinnocent7No ratings yet
- Colon, Rectum and AnusDocument30 pagesColon, Rectum and AnusKiara GovenderNo ratings yet
- Hirschsprung DiseaseDocument25 pagesHirschsprung DiseaseMuhammad Zaniar RamadhaniNo ratings yet
- Imaging of Congenital Anomalies of The Gastrointestinal TractDocument12 pagesImaging of Congenital Anomalies of The Gastrointestinal TractMateen ShukriNo ratings yet
- Anomalies of The Upper Urinary TractDocument6 pagesAnomalies of The Upper Urinary TractMohamed Al-zichrawyNo ratings yet
- Curs Fetal Abdominal AnomaliesDocument137 pagesCurs Fetal Abdominal AnomaliesCristi SoareceNo ratings yet
- Anorectal MalformationsDocument19 pagesAnorectal MalformationsJumrotun Ni'mahNo ratings yet
- Lec 1Document52 pagesLec 1zainabd1964No ratings yet
- Congenital Anomalies of The KidneyDocument21 pagesCongenital Anomalies of The KidneyRaghu Rajan100% (1)
- Gyno Review: Final Surgery Exam 2011Document36 pagesGyno Review: Final Surgery Exam 2011Zee TeeNo ratings yet
- 20 - Pediatric Urinary DisordersDocument62 pages20 - Pediatric Urinary DisordersKhaalid AbdirahmanNo ratings yet
- Anorectal Malformations in Children - A Review: Amrish Vaidya, Kishore AdyanthayaDocument4 pagesAnorectal Malformations in Children - A Review: Amrish Vaidya, Kishore Adyanthayasangvi_tvNo ratings yet
- Disorders of The IntestinesDocument64 pagesDisorders of The IntestinesCharmaine Torio PastorNo ratings yet
- Hirschsprung's Disease: (Congenital Aganglionic Megacolon)Document16 pagesHirschsprung's Disease: (Congenital Aganglionic Megacolon)umiNo ratings yet
- Hirsch SprungDocument6 pagesHirsch SprunghakimNo ratings yet
- Meckels DiverticulumDocument5 pagesMeckels DiverticulumKevean Kimi LimNo ratings yet
- SG3 Paediatric Surgical EmergenciesDocument69 pagesSG3 Paediatric Surgical EmergenciesDiyana ZatyNo ratings yet
- Anal AtresiaDocument13 pagesAnal AtresiaAhmad Ihsan100% (1)
- Colonic and Small Intestine Disorders-1Document28 pagesColonic and Small Intestine Disorders-1YIKI ISAACNo ratings yet
- 19-Pediatric SurgeryDocument39 pages19-Pediatric Surgerycallisto3487No ratings yet
- HerniaDocument29 pagesHerniaAnonymous BzS0RF1qyNo ratings yet
- Seminarduodenalatresia 170505174313Document30 pagesSeminarduodenalatresia 170505174313Amirhossein SheikhiNo ratings yet
- Lecture 1 HirschprungDocument18 pagesLecture 1 HirschprungsharmeenNo ratings yet
- Intussusception 161007042729 PDFDocument44 pagesIntussusception 161007042729 PDFDina MarselinaNo ratings yet
- 31 Uro Hydrocele 111211112520 Phpapp02Document6 pages31 Uro Hydrocele 111211112520 Phpapp02ppc_20No ratings yet
- 3 Common Pediatric Surgery ContinuedDocument5 pages3 Common Pediatric Surgery ContinuedMohamed Al-zichrawyNo ratings yet
- Diseases of the Liver and Biliary TreeFrom EverandDiseases of the Liver and Biliary TreeAnnarosa FloreaniNo ratings yet
- Guide to Pediatric Urology and Surgery in Clinical PracticeFrom EverandGuide to Pediatric Urology and Surgery in Clinical PracticeNo ratings yet
- 1 ScrotumDocument7 pages1 ScrotumMohamed Al-zichrawyNo ratings yet
- 1 Urinary StonesDocument11 pages1 Urinary StonesMohamed Al-zichrawyNo ratings yet
- Rheumatology and Bone DiseaseDocument8 pagesRheumatology and Bone DiseaseMohamed Al-zichrawyNo ratings yet
- Septic Arthritis: Clinical FeaturesDocument4 pagesSeptic Arthritis: Clinical FeaturesMohamed Al-zichrawyNo ratings yet
- Anomalies of The Upper Urinary TractDocument6 pagesAnomalies of The Upper Urinary TractMohamed Al-zichrawyNo ratings yet
- Renal Tumors RCC Renal Cells Carcinoma Renal Adenocarcinoma HypernephromaDocument5 pagesRenal Tumors RCC Renal Cells Carcinoma Renal Adenocarcinoma HypernephromaMohamed Al-zichrawyNo ratings yet
- Neuromuscular Junction Disorders - 1Document30 pagesNeuromuscular Junction Disorders - 1Mohamed Al-zichrawyNo ratings yet
- Rheumatology and Bone DiseaseDocument32 pagesRheumatology and Bone DiseaseMohamed Al-zichrawyNo ratings yet
- Fibromyalgia: PathophysiologyDocument4 pagesFibromyalgia: PathophysiologyMohamed Al-zichrawyNo ratings yet
- Gyn MCQ ..Group E PDFDocument15 pagesGyn MCQ ..Group E PDFMohamed Al-zichrawyNo ratings yet
- Acute Pelvic Pain: HistoryDocument4 pagesAcute Pelvic Pain: HistoryMohamed Al-zichrawyNo ratings yet
- Cerebral Edema: BBB (Blood Brain Barrier)Document4 pagesCerebral Edema: BBB (Blood Brain Barrier)Mohamed Al-zichrawyNo ratings yet
- Smart Study مهم جداDocument328 pagesSmart Study مهم جداMohamed Al-zichrawy100% (2)
- Neurological Assessment in Head Trauma: 1-Vital Sign MonitoringDocument4 pagesNeurological Assessment in Head Trauma: 1-Vital Sign MonitoringMohamed Al-zichrawyNo ratings yet
- Latest Gynecology Multiple Choice Questions and Answers For PDFDocument10 pagesLatest Gynecology Multiple Choice Questions and Answers For PDFMohamed Al-zichrawy100% (1)
- Brain Tumors: Primary BTDocument5 pagesBrain Tumors: Primary BTMohamed Al-zichrawyNo ratings yet
- Head Injury: Classification of Head Injury A-Scalp Injuries B-Skull FracturesDocument6 pagesHead Injury: Classification of Head Injury A-Scalp Injuries B-Skull FracturesMohamed Al-zichrawyNo ratings yet
- Thalassemia Syndromes: Clinical Features and ComplicationsDocument22 pagesThalassemia Syndromes: Clinical Features and ComplicationsMohamed Al-zichrawyNo ratings yet
- 3 Common Pediatric Surgery ContinuedDocument5 pages3 Common Pediatric Surgery ContinuedMohamed Al-zichrawyNo ratings yet
- Chest+heart+medistinum RadiologyDocument4 pagesChest+heart+medistinum RadiologyMohamed Al-zichrawyNo ratings yet
- Evaluation of Antimicrobial and Antioxidant Activity of Crude Methanol Extract and Its Fractions of Mussaenda Philippica LeavesDocument14 pagesEvaluation of Antimicrobial and Antioxidant Activity of Crude Methanol Extract and Its Fractions of Mussaenda Philippica Leavesiaset123No ratings yet
- Week1 CombineDocument91 pagesWeek1 CombineraleyNo ratings yet
- Physics AS Level Formulas and DefinitionsDocument5 pagesPhysics AS Level Formulas and DefinitionsCharlene DaneekaNo ratings yet
- Shreya Shukla Case Study-2Document41 pagesShreya Shukla Case Study-2Rishabh UpadhyayNo ratings yet
- Create Request For QuotationDocument18 pagesCreate Request For QuotationAdauto PolizeliNo ratings yet
- Instruction SMA TripowerDocument10 pagesInstruction SMA TripowerMirea AurelNo ratings yet
- Z-Transform Theory: Itm, GurgaonDocument85 pagesZ-Transform Theory: Itm, GurgaonkanchiNo ratings yet
- Ricky C. Alfon: - Individual Differences - (Prof Ed 6) Facilitating Learner-Centered TeachingDocument8 pagesRicky C. Alfon: - Individual Differences - (Prof Ed 6) Facilitating Learner-Centered TeachingMark Joseph DacubaNo ratings yet
- M50-2014 V6Document334 pagesM50-2014 V6Dragan MilosevicNo ratings yet
- Ganesh Balasubramanian (Eds.) - Advances in Nanomaterials - Fundamentals, Properties and Applications-Springer International Publishing (2018)Document181 pagesGanesh Balasubramanian (Eds.) - Advances in Nanomaterials - Fundamentals, Properties and Applications-Springer International Publishing (2018)Jesus Moreno Castillo100% (1)
- Materials Science II Chapter 10Document41 pagesMaterials Science II Chapter 10Rebeca CremonezNo ratings yet
- I. Objectives: Computer System ServicingDocument4 pagesI. Objectives: Computer System ServicingCatherine Mae Lammag BuananNo ratings yet
- Legislative Counsel's Digest: Section 1 of This Bill Authorizes A Person Who Is Not Under Arrest or in TheDocument9 pagesLegislative Counsel's Digest: Section 1 of This Bill Authorizes A Person Who Is Not Under Arrest or in TheFOX5 VegasNo ratings yet
- A Guide To The Management of Tuberculosis in Patients With Chronic Liver DiseaseDocument12 pagesA Guide To The Management of Tuberculosis in Patients With Chronic Liver DiseaseMeldaNo ratings yet
- Sample Assignment 1-1Document20 pagesSample Assignment 1-1Nir IslamNo ratings yet
- Ch06 Solations Brigham 10th EDocument32 pagesCh06 Solations Brigham 10th ERafay HussainNo ratings yet
- General Characteristics of Fungi. Details AbcdefDocument9 pagesGeneral Characteristics of Fungi. Details Abcdefabdul hadiNo ratings yet
- Problem SetDocument12 pagesProblem SetJohn Lade Tan NacionalNo ratings yet
- Pdms 12 HvacDocument4 pagesPdms 12 HvacsadeghmsgNo ratings yet
- Assembly of PartsDocument29 pagesAssembly of PartsthirumalaikumaranNo ratings yet
- A. RAPID Research Grant: Total Faculty Costs 0Document3 pagesA. RAPID Research Grant: Total Faculty Costs 0Uzma TahirNo ratings yet
- Buildability ScoreDocument6 pagesBuildability ScoreVachara PeansupapNo ratings yet
- Activity 6Document4 pagesActivity 6Junior SmithNo ratings yet
- Yeastar P-Series PBX System Datasheet enDocument7 pagesYeastar P-Series PBX System Datasheet enYemen BrokerNo ratings yet
- Policy - Task 2 ContentDocument6 pagesPolicy - Task 2 ContentJadhav AmitNo ratings yet
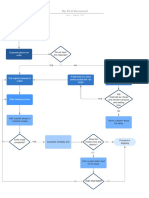
- User Flow DiagramDocument1 pageUser Flow DiagramjimNo ratings yet
- Introductory Entomology: Third Semester Lamjung CampusDocument206 pagesIntroductory Entomology: Third Semester Lamjung Campusnishan khatriNo ratings yet