Download as pdf or txt
You might also like
- Guard Retention-FlowChartDocument1 pageGuard Retention-FlowChartthedananti0% (1)
- Endodontic Therapy - (6th Ed.)Document1,744 pagesEndodontic Therapy - (6th Ed.)Ahmad100% (3)
- Risk Intelligence Map Health Care Providers PDFDocument1 pageRisk Intelligence Map Health Care Providers PDFYasserAl-mansourNo ratings yet
- Segregation of Duties Matrix SampleDocument3 pagesSegregation of Duties Matrix SampleNijith p.nNo ratings yet
- Corrective Action Plan TemplateDocument1 pageCorrective Action Plan TemplateSamsung JosephNo ratings yet
- HS Training Matrix 18.04.16Document1 pageHS Training Matrix 18.04.16Asad AwanNo ratings yet
- SmallgroupresultsreportDocument1 pageSmallgroupresultsreportapi-392364749No ratings yet
- Batteries: Color Code For Schematic LinesDocument2 pagesBatteries: Color Code For Schematic LinesIsaac NewtonNo ratings yet
- Von Willebrand Factor Antigen - 0020002300: Limitations/interfering SubstancesDocument3 pagesVon Willebrand Factor Antigen - 0020002300: Limitations/interfering Substances28850No ratings yet
- HIRADC - Pekerjaan 20 KV - PLTGU - Update 5 March 2018Document5 pagesHIRADC - Pekerjaan 20 KV - PLTGU - Update 5 March 2018ghieee100% (2)
- TNA TemplateDocument4 pagesTNA TemplateSwapon KumarNo ratings yet
- TrakCare Overview 09012015Document5 pagesTrakCare Overview 09012015keziajessNo ratings yet
- Von Willebrand Factor Activity - 0020004700: in Vitro Diagnostic Medical Device In-Vitro DiagnostikumDocument3 pagesVon Willebrand Factor Activity - 0020004700: in Vitro Diagnostic Medical Device In-Vitro Diagnostikum28850No ratings yet
- A380 Family Maintenance ConceptDocument1 pageA380 Family Maintenance Conceptyazan999100% (1)
- JEC Health Chart 11-7-09Document1 pageJEC Health Chart 11-7-09Stix1972No ratings yet
- Matrik PelatihanDocument1 pageMatrik PelatihanYogi RadityaNo ratings yet
- Failure Mode and Effects Analysis by BoschDocument52 pagesFailure Mode and Effects Analysis by Boschwawawa1100% (1)
- Amino Acid Analysis in Plasma-Serum and Urine Brochure en 4Document6 pagesAmino Acid Analysis in Plasma-Serum and Urine Brochure en 4yousrazeidan1979No ratings yet
- Rivoningo T Safety ConsultantsDocument4 pagesRivoningo T Safety ConsultantsZiadSutton100% (1)
- Score Card BNI April 2023Document1 pageScore Card BNI April 2023Al - AminNo ratings yet
- Indonesia ERT TrainingnExercise Matrix-Rev 04 - March 2017Document2 pagesIndonesia ERT TrainingnExercise Matrix-Rev 04 - March 2017sepri manerson sinagaNo ratings yet
- Federal Child Welfare Grant Program Matrix TableDocument2 pagesFederal Child Welfare Grant Program Matrix TableBeverly TranNo ratings yet
- Health Technology ManagementDocument26 pagesHealth Technology Managementhaseeb JuttNo ratings yet
- 016 SkillFront ISO IEC 27001 Information SecurityDocument63 pages016 SkillFront ISO IEC 27001 Information SecurityAbNo ratings yet
- 016 SkillFront ISO IEC 27001 Information SecurityDocument63 pages016 SkillFront ISO IEC 27001 Information Securitythiyaga1988No ratings yet
- Risk Assment (Version 1) .XLSBDocument4 pagesRisk Assment (Version 1) .XLSBDanie PretoriusNo ratings yet
- Orchestrating A Winning Strategy: End-To-End Supply Chain SynchronizationDocument52 pagesOrchestrating A Winning Strategy: End-To-End Supply Chain SynchronizationANGELICANo ratings yet
- SWOT-Analyse ISO /TS 16949:2009Document1 pageSWOT-Analyse ISO /TS 16949:2009Nedra DebbechNo ratings yet
- Major Process Safety Incident Vs Root Cause Map: (Quick Reference Guide)Document1 pageMajor Process Safety Incident Vs Root Cause Map: (Quick Reference Guide)Sheik BenasudeenNo ratings yet
- Tan 2001Document6 pagesTan 2001t123medNo ratings yet
- Agiba Safety Workshop June 2019Document5 pagesAgiba Safety Workshop June 2019QHSE Manager100% (1)
- 3.8.1. Training MatrixDocument1 page3.8.1. Training MatrixblackcoutureconsultationsNo ratings yet
- Cardiovascular Pharmacology] 03 Heparin - KeyDocument1 pageCardiovascular Pharmacology] 03 Heparin - KeyRubie Ann TillorNo ratings yet
- Appendix 5 Hazmat Inventory SheetDocument1 pageAppendix 5 Hazmat Inventory Sheetaldrb hospitalNo ratings yet
- Rapid Object Detection Using A Boosted Cascade of Simple FeaturesDocument9 pagesRapid Object Detection Using A Boosted Cascade of Simple FeaturesYuvraj NegiNo ratings yet
- Operating Processes: HistoryDocument23 pagesOperating Processes: HistoryFadel MuhammadNo ratings yet
- Stroke 2014 Flowchart A3-FormatDocument2 pagesStroke 2014 Flowchart A3-FormateliansubiratsNo ratings yet
- జీవితమే సఫలము మొదటి సంపుటి వి వి రామారావుDocument305 pagesజీవితమే సఫలము మొదటి సంపుటి వి వి రామారావుKishore KNo ratings yet
- Final CB Risk Register v27-11-2019Document18 pagesFinal CB Risk Register v27-11-2019Job Chaclan0% (1)
- SAS Banking - Basel II SolutionsDocument12 pagesSAS Banking - Basel II Solutionsashfaqultanim007No ratings yet
- Cardiovascular Pharmacology) 03 Heparin - KeyDocument1 pageCardiovascular Pharmacology) 03 Heparin - Keyhasanatiya41No ratings yet
- Weightlifting App Features ComparisonDocument2 pagesWeightlifting App Features ComparisonMariusNo ratings yet
- S, D Table: Zone Actions To Be InitiatedDocument1 pageS, D Table: Zone Actions To Be InitiatedkrishnakumarNo ratings yet
- HS Training Matrix 18.04.16Document1 pageHS Training Matrix 18.04.16Fares Fares100% (1)
- It Disaster Recovery Plan TemplateDocument51 pagesIt Disaster Recovery Plan TemplateDwdroo DiwokNo ratings yet
- Real-Time Alerting System For COVID-19 and Other Stress Events Using Wearable DataDocument26 pagesReal-Time Alerting System For COVID-19 and Other Stress Events Using Wearable DataLuiz Folha FlaskNo ratings yet
- TOR-Finance Data Analyst (NHM-Fin, MoH&FW)Document4 pagesTOR-Finance Data Analyst (NHM-Fin, MoH&FW)aadi1127No ratings yet
- Major Process Safety Incident Vs Rooat CauseDocument1 pageMajor Process Safety Incident Vs Rooat Causensikakabasi Okon100% (1)
- Module 7 (Maintenance Practices) Sub Module 7.3 (Tools)Document99 pagesModule 7 (Maintenance Practices) Sub Module 7.3 (Tools)Ahsan Malik100% (2)
- Tool Selector V2Document1 pageTool Selector V2Mohammed MuzakkirNo ratings yet
- Report Google BusinessDocument1 pageReport Google BusinesskarismalicensingNo ratings yet
- Aspikinesn Last7days Analytics ReportDocument1 pageAspikinesn Last7days Analytics ReportLahad DiaNo ratings yet
- Documentation PHENIX LIBERTY Anglais V05.00Document2 pagesDocumentation PHENIX LIBERTY Anglais V05.00Jose HernandezNo ratings yet
- Documentation PHENIX LIBERTY Anglais V05.00Document2 pagesDocumentation PHENIX LIBERTY Anglais V05.00klemionka2No ratings yet
- Checklist SHE Mr. RaymonDocument12 pagesChecklist SHE Mr. RaymonRizky RamadhanNo ratings yet
- UntitledDocument2 pagesUntitledRaj MohamadNo ratings yet
- Matrix History Training MaintenanceDocument2 pagesMatrix History Training MaintenanceReza SyailendraNo ratings yet
- Instant Assessments for Data Tracking, Grade 4: Language ArtsFrom EverandInstant Assessments for Data Tracking, Grade 4: Language ArtsRating: 5 out of 5 stars5/5 (1)
- How To Build Csars: For OpentoscaDocument25 pagesHow To Build Csars: For OpentoscaVaibhav DafaleNo ratings yet
- Chapter I PsychologyDocument8 pagesChapter I PsychologyVaibhav DafaleNo ratings yet
- Anssi Profil PP 2015 01à06Document215 pagesAnssi Profil PP 2015 01à06Vaibhav DafaleNo ratings yet
- Gs Nfv-Sol004v020501pDocument21 pagesGs Nfv-Sol004v020501pVaibhav DafaleNo ratings yet
- CsarDocument56 pagesCsarVaibhav DafaleNo ratings yet
- Banking Technology and Service Quality: Evidence From Private Sector Banks in KeralaDocument6 pagesBanking Technology and Service Quality: Evidence From Private Sector Banks in KeralaVaibhav DafaleNo ratings yet
- An Introduction To The CSAR Package: Jose M Muino May 19, 2021Document5 pagesAn Introduction To The CSAR Package: Jose M Muino May 19, 2021Vaibhav DafaleNo ratings yet
- Functional Abilities FormDocument2 pagesFunctional Abilities FormVaibhav DafaleNo ratings yet
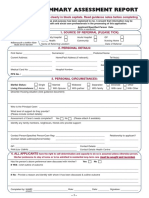
- Common Summary Assessment ReportDocument4 pagesCommon Summary Assessment ReportVaibhav DafaleNo ratings yet
- Guidelines For Attorneys On The Protection of Personal Information ActDocument31 pagesGuidelines For Attorneys On The Protection of Personal Information ActVaibhav DafaleNo ratings yet
- CSARGuidance DocumentDocument11 pagesCSARGuidance DocumentVaibhav DafaleNo ratings yet
- Joju Charging Emergency Services BrochureDocument8 pagesJoju Charging Emergency Services BrochureVaibhav DafaleNo ratings yet
- Hydrogeological Report: Atal Bhujal Yojana (Ataljal)Document17 pagesHydrogeological Report: Atal Bhujal Yojana (Ataljal)Vaibhav DafaleNo ratings yet
- Personal Information (Popi) Act: Protection ofDocument2 pagesPersonal Information (Popi) Act: Protection ofVaibhav DafaleNo ratings yet
- Hydrogeological Report: Atal Bhujal Yojana (Ataljal)Document15 pagesHydrogeological Report: Atal Bhujal Yojana (Ataljal)Vaibhav DafaleNo ratings yet
- Talukawise GWA2008-09Document166 pagesTalukawise GWA2008-09Vaibhav DafaleNo ratings yet
- Hydrogeological Report: Atal Bhujal Yojana (Atal Jal)Document16 pagesHydrogeological Report: Atal Bhujal Yojana (Atal Jal)Vaibhav DafaleNo ratings yet
- Functional Abilities FormDocument4 pagesFunctional Abilities FormVaibhav DafaleNo ratings yet
- Em 602Document23 pagesEm 602Vaibhav DafaleNo ratings yet
- 297 Authors: Institution: Department of Urology, Eulji University, College of Medicine TitleDocument1 page297 Authors: Institution: Department of Urology, Eulji University, College of Medicine TitleVaibhav DafaleNo ratings yet
- 2102 13225Document19 pages2102 13225Vaibhav DafaleNo ratings yet
- BIS Working Papers: The Dollar, Bank Leverage and Real Economic Activity: An Evolving RelationshipDocument18 pagesBIS Working Papers: The Dollar, Bank Leverage and Real Economic Activity: An Evolving RelationshipVaibhav DafaleNo ratings yet
- Hemani Neil SNR Thesis WebDocument89 pagesHemani Neil SNR Thesis WebVaibhav DafaleNo ratings yet
- Dec 2016Document72 pagesDec 2016Vaibhav DafaleNo ratings yet
- Fluid and Electrolytes ImbalanceDocument49 pagesFluid and Electrolytes ImbalanceMohamed Na3eemNo ratings yet
- Types of BiasDocument2 pagesTypes of BiasAli GhanemNo ratings yet
- 2017 AbbankDocument5 pages2017 AbbankVincent ReyesNo ratings yet
- Wikipedia HyperparathyroidismDocument7 pagesWikipedia Hyperparathyroidismkeith andriesNo ratings yet
- PrachishaDocument13 pagesPrachishaRahul GilgilanNo ratings yet
- Assessments of Safe Medication Administration in Nursing EducationDocument12 pagesAssessments of Safe Medication Administration in Nursing EducationMichael AmandyNo ratings yet
- Lecture 17 - Thyroid Disorders (Including Struma and CA Thyroid) - Dr. M. Robikhul Ikhsan, SP - PD-KEMD (2021)Document21 pagesLecture 17 - Thyroid Disorders (Including Struma and CA Thyroid) - Dr. M. Robikhul Ikhsan, SP - PD-KEMD (2021)Ivan AditamaNo ratings yet
- Review of Aetiology and Management of Testicular Abscess and Case Reports On Testicle Sparing Management of Testicular AbscessDocument5 pagesReview of Aetiology and Management of Testicular Abscess and Case Reports On Testicle Sparing Management of Testicular AbscessBodat BodatsNo ratings yet
- 7.3 Test Taking SkillsDocument15 pages7.3 Test Taking SkillsHannah RealuyoNo ratings yet
- Religious Fanaticism and Poly-Behavioral Addiction: by Dr. James SlobodzienDocument6 pagesReligious Fanaticism and Poly-Behavioral Addiction: by Dr. James SlobodzienMuhammad Zakie ArfiansyahNo ratings yet
- What Are The Factors That Put A Pregnancy at RiskDocument3 pagesWhat Are The Factors That Put A Pregnancy at RiskWindySeptianiIshakNo ratings yet
- Infection Control Program Flow ChartDocument1 pageInfection Control Program Flow ChartAnonymous ORleRrNo ratings yet
- PiracetamDocument2 pagesPiracetamPaolo MastrovitiNo ratings yet
- The Five Eras of ChiropracticDocument8 pagesThe Five Eras of ChiropracticSam100% (1)
- Forceps Delivery: Potential Benefits and A Call For Continued TrainingDocument2 pagesForceps Delivery: Potential Benefits and A Call For Continued TrainingTyron ChuaNo ratings yet
- Bài Thuyết Trình HealthcareDocument2 pagesBài Thuyết Trình HealthcareNguyen Khac DucNo ratings yet
- Vitamin K Deficiency in InfantsDocument20 pagesVitamin K Deficiency in InfantsAnne TjanNo ratings yet
- Avipattikar ChurnaDocument3 pagesAvipattikar ChurnadrbhaveshpNo ratings yet
- Spine Fracture and DislocationDocument74 pagesSpine Fracture and DislocationLydiaKainamaa100% (2)
- Evaluation For Module 1Document4 pagesEvaluation For Module 1Patricia PascuaNo ratings yet
- Leukodystrophies in Children Diagnosis, Care, and TreatmentDocument15 pagesLeukodystrophies in Children Diagnosis, Care, and TreatmentEduardo Rios DuboisNo ratings yet
- Becker, 1997Document8 pagesBecker, 1997DijuNo ratings yet
- Health Certificate: Personal Details: Section ADocument3 pagesHealth Certificate: Personal Details: Section APrashob SugathanNo ratings yet
- Cardiac Resynchronization TherapyDocument3 pagesCardiac Resynchronization TherapyassumptaNo ratings yet
- Kidney TransplantDocument3 pagesKidney TransplantSuneel Kumar PrajapatiNo ratings yet
- Caalm Citizen Petition To FDADocument23 pagesCaalm Citizen Petition To FDAZerohedge JanitorNo ratings yet
- Drug Study: Nursing DepartmentDocument1 pageDrug Study: Nursing Departmentgiselle chloeNo ratings yet
- CHN 1st and 2nd Level 2nd SemDocument9 pagesCHN 1st and 2nd Level 2nd SemCharlaine Gripal SudlaNo ratings yet
- 2010 NHIS Public Use Variable Summary: Filename - Section: Document Vers Ion DateDocument27 pages2010 NHIS Public Use Variable Summary: Filename - Section: Document Vers Ion DateJin SiclonNo ratings yet































![Cardiovascular Pharmacology] 03 Heparin - Key](https://imgv2-2-f.scribdassets.com/img/document/747791383/149x198/8cd3843a2c/1720070291?v=1)