Download as pdf or txt
You might also like
- Donald A. Neumann-Kinesiology of The Musculoskeletal System PDFDocument607 pagesDonald A. Neumann-Kinesiology of The Musculoskeletal System PDFSekar Ciptaningrum97% (97)
- NURS 681 Advanced Health Physical Assessment and Lab APRN 202207SUIIOL OL B 202207SUIIOL 2022Document22 pagesNURS 681 Advanced Health Physical Assessment and Lab APRN 202207SUIIOL OL B 202207SUIIOL 2022mamba.dedanNo ratings yet
- Acute PancreatitisDocument31 pagesAcute PancreatitisAmoroso, Marian Corneth D.No ratings yet
- Family Medicine 33: 28-Year-Old Female With Dizziness: Learning ObjectivesDocument6 pagesFamily Medicine 33: 28-Year-Old Female With Dizziness: Learning ObjectivesAndrea Kristin OrigenesNo ratings yet
- BS 4254Document19 pagesBS 4254gugaruban100% (4)
- Nervous System AlterationsDocument62 pagesNervous System AlterationsAsal SalahNo ratings yet
- 6 Externalities Price Quantity Regulation3Document29 pages6 Externalities Price Quantity Regulation3Arlene DaroNo ratings yet
- Prelim ExamDocument17 pagesPrelim Examsaci PTNo ratings yet
- Hydraulic Axial Piston Eaton Vickers PVB Pump: - Basic CharacteristicsDocument13 pagesHydraulic Axial Piston Eaton Vickers PVB Pump: - Basic Characteristicsjose alberto olvera gomezNo ratings yet
- O & M of Sub StationDocument94 pagesO & M of Sub StationAlbert Sekar100% (2)
- Project Report On RTS Juice PlantDocument7 pagesProject Report On RTS Juice PlantEIRI Board of Consultants and PublishersNo ratings yet
- jOURNAL THEORY TTMDocument14 pagesjOURNAL THEORY TTMTrihartuty TrihartutyNo ratings yet
- D V I C: LordosisDocument13 pagesD V I C: Lordosisdlneisha610% (1)
- Bates' Visual Guide To Physical Examination OSCE 3: Sore ThroatDocument6 pagesBates' Visual Guide To Physical Examination OSCE 3: Sore Throatgh100% (1)
- Physical Examination ChecklistDocument4 pagesPhysical Examination Checklistmonica ortiz100% (1)
- Full Chapter Volpe S Neurology of The Newborn 7Th Edition Joseph J Volpe PDFDocument53 pagesFull Chapter Volpe S Neurology of The Newborn 7Th Edition Joseph J Volpe PDFdennis.davis980No ratings yet
- EL Husseinys Essentials of PediatricsDocument253 pagesEL Husseinys Essentials of PediatricsMorozovschi VitalieNo ratings yet
- Paediatrics Notes-2017 BatchDocument102 pagesPaediatrics Notes-2017 BatchMohan EthirajanNo ratings yet
- Medical Review of Systems: General, Constitutional Heart and Cardiovascular Hematologic/LymphaticDocument1 pageMedical Review of Systems: General, Constitutional Heart and Cardiovascular Hematologic/LymphaticBola S-SNo ratings yet
- Abdominal ExaminationDocument16 pagesAbdominal ExaminationLana IbrahimNo ratings yet
- How To Document A Patient Assessment SOAP PDFDocument3 pagesHow To Document A Patient Assessment SOAP PDFaulia ekaNo ratings yet
- Vasoactive Agents For Adult Septic Shock: An Update and ReviewDocument10 pagesVasoactive Agents For Adult Septic Shock: An Update and ReviewntnquynhproNo ratings yet
- Neurologic HistoryDocument68 pagesNeurologic HistoryMerahit AberaNo ratings yet
- Assessment of The Chest and LungsDocument46 pagesAssessment of The Chest and LungsSumathi GopinathNo ratings yet
- Human Anatomy-Skeleton and MusclesDocument47 pagesHuman Anatomy-Skeleton and Musclesshahla aymanNo ratings yet
- Cardiovascular BigDocument37 pagesCardiovascular Bigfaiz nasirNo ratings yet
- Abdominal Examination For PSIII Edited-1Document33 pagesAbdominal Examination For PSIII Edited-1myarjddbzNo ratings yet
- Bates Thorax Lungs With TermsDocument4 pagesBates Thorax Lungs With Termscrystalshe100% (1)
- Head To Toe Checklist (Masroni)Document13 pagesHead To Toe Checklist (Masroni)hillary elsaNo ratings yet
- Bate's Guide To Physical examination+MCQsDocument4 pagesBate's Guide To Physical examination+MCQsRaden Adjeng PalupiNo ratings yet
- History Taking and Physical Examination of Cardiovascular System-The EssentialsDocument72 pagesHistory Taking and Physical Examination of Cardiovascular System-The EssentialsReena Joanella TimbreNo ratings yet
- Clinical Examination in Neonates: Yurita Handoyo DR., SpaDocument60 pagesClinical Examination in Neonates: Yurita Handoyo DR., SpaFebri ChristallagoNo ratings yet
- Complete Physical ExamDocument10 pagesComplete Physical ExamSohayb Abu TabanjehNo ratings yet
- Fetal ArrhythmiasDocument18 pagesFetal ArrhythmiasKarin Stefanny Muñoz CastilloNo ratings yet
- 10.history Taking (DR - Hani)Document17 pages10.history Taking (DR - Hani)علي. احمدNo ratings yet
- Internal Medicine Sample Osce Examination Component Questions eDocument2 pagesInternal Medicine Sample Osce Examination Component Questions eGhada ElhassanNo ratings yet
- Thrombocytopenia in PregnancyDocument13 pagesThrombocytopenia in PregnancyJhuli Elizabeth CNo ratings yet
- Anterior Shoulder Pain: What Questions Would You Ask in The Subjective Examination?Document3 pagesAnterior Shoulder Pain: What Questions Would You Ask in The Subjective Examination?Kanwal KhanNo ratings yet
- Pediatrics Recommended BooksDocument1 pagePediatrics Recommended BooksJared Khoo Er HauNo ratings yet
- Study Guide #10 With HEENT ChecklistDocument4 pagesStudy Guide #10 With HEENT ChecklistPrince DuNo ratings yet
- MED 1.17 - Gastrointestinal CancersDocument6 pagesMED 1.17 - Gastrointestinal CancersZazaNo ratings yet
- Case Summary Pediatrics03 3-Year-ODocument10 pagesCase Summary Pediatrics03 3-Year-OJeffNo ratings yet
- The Newborn ExaminationDocument132 pagesThe Newborn ExaminationdevilstNo ratings yet
- Clinical CasesDocument12 pagesClinical CasesAndreea HanuNo ratings yet
- Week 2 InitialDocument2 pagesWeek 2 InitialSara NielsenNo ratings yet
- PE - A Practical Guide To Clinical MedicineDocument3 pagesPE - A Practical Guide To Clinical MedicineavracadavraNo ratings yet
- Neuroscience I - Neurologic History Taking and Examination (POBLETE)Document9 pagesNeuroscience I - Neurologic History Taking and Examination (POBLETE)Johanna Hamnia PobleteNo ratings yet
- Common Bacteria by Site of Infection: Mouth Skin/Soft Tissue Bone and JointDocument72 pagesCommon Bacteria by Site of Infection: Mouth Skin/Soft Tissue Bone and JointMuthia FadhilaNo ratings yet
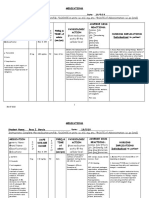
- Instructions: Complete The Medication Profile. DOSAGE in Units: I.E. ML/, MG, Etc. ROUTE of Administration: I.E. Po (Oral)Document12 pagesInstructions: Complete The Medication Profile. DOSAGE in Units: I.E. ML/, MG, Etc. ROUTE of Administration: I.E. Po (Oral)Rosa Garcia100% (1)
- Philosophy of NursingDocument8 pagesPhilosophy of Nursingapi-430575435No ratings yet
- Community-Acquired Pneumoniaandhospital-Acquiredpneumonia: Charles W. Lanks,, Ali I. Musani,, David W. HsiaDocument15 pagesCommunity-Acquired Pneumoniaandhospital-Acquiredpneumonia: Charles W. Lanks,, Ali I. Musani,, David W. HsiaMajo EscobarNo ratings yet
- Fetal and Neonatal Physiology PDFDocument33 pagesFetal and Neonatal Physiology PDFObsaNo ratings yet
- Clinical Examination of CVSDocument33 pagesClinical Examination of CVSmahnoorNo ratings yet
- Neurological SheetDocument70 pagesNeurological SheetKlb ElbnatNo ratings yet
- Bates Outline of Chapter 8Document15 pagesBates Outline of Chapter 8KatherynSotoNo ratings yet
- Pediatric Eye DiseasesDocument5 pagesPediatric Eye DiseasesfrnksusNo ratings yet
- Methods of ExaminationDocument53 pagesMethods of ExaminationTeodor ŞişianuNo ratings yet
- Health HistoryDocument19 pagesHealth HistoryAngelene Caliva100% (1)
- Shift of Heart and Trachea To Left: Tension PneumothoraxDocument44 pagesShift of Heart and Trachea To Left: Tension PneumothoraxlettasamudraNo ratings yet
- Abdominal Masses in Pediatrics - 2015Document5 pagesAbdominal Masses in Pediatrics - 2015Jéssica VazNo ratings yet
- Ectopic PregnancyDocument76 pagesEctopic PregnancyVivian Jean TapayaNo ratings yet
- Topnotch Surgery For Moonlighters Part 1 of 2Document83 pagesTopnotch Surgery For Moonlighters Part 1 of 2Joan SolomonNo ratings yet
- Physical Examination Techniques and ManueversDocument160 pagesPhysical Examination Techniques and ManueversMa-anJaneDiamosNo ratings yet
- Chapter 30 StudyGuide WorkbookDocument5 pagesChapter 30 StudyGuide WorkbookJacqueline GreerNo ratings yet
- Abdominal AssessmentDocument7 pagesAbdominal AssessmentGlen Dale100% (1)
- Ebstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandEbstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Bookstore Order: RCBC Commercial Fairview Branch Order Status: Account Name: Account Number: Swift CodeDocument1 pageBookstore Order: RCBC Commercial Fairview Branch Order Status: Account Name: Account Number: Swift CodeArlene DaroNo ratings yet
- PARA 11 Intro To ParasitologyDocument9 pagesPARA 11 Intro To ParasitologyArlene DaroNo ratings yet
- The Former Philippines Thru Foreign EyesDocument45 pagesThe Former Philippines Thru Foreign EyesArlene DaroNo ratings yet
- (Para) Introduction To Parasitology and Protozoology-Dr. Dela Rosa (Tiglao)Document7 pages(Para) Introduction To Parasitology and Protozoology-Dr. Dela Rosa (Tiglao)Arlene DaroNo ratings yet
- Fault Tolerant Quiz Module: Before The ExamDocument2 pagesFault Tolerant Quiz Module: Before The ExamArlene DaroNo ratings yet
- GalactosemiaDocument41 pagesGalactosemiaArlene DaroNo ratings yet
- Sta. Lucia High School: A School VisitDocument3 pagesSta. Lucia High School: A School VisitArlene DaroNo ratings yet
- The Incidental Fertility Effects of School Condom Distribution ProgramsDocument43 pagesThe Incidental Fertility Effects of School Condom Distribution ProgramsArlene DaroNo ratings yet
- Sector Specific FactorDocument48 pagesSector Specific FactorArlene DaroNo ratings yet
- Feenstra Taylor Econ CH04Document66 pagesFeenstra Taylor Econ CH04Arlene DaroNo ratings yet
- Trade and Technology: The Ricardian ModelDocument74 pagesTrade and Technology: The Ricardian ModelArlene DaroNo ratings yet
- Coastal Clean Up PlanDocument2 pagesCoastal Clean Up PlanArlene DaroNo ratings yet
- EDH 170 AustrailiaDocument18 pagesEDH 170 AustrailiaArlene DaroNo ratings yet
- The Study of Demography Encompasses The Following: A. Size and Shape of PopulationDocument1 pageThe Study of Demography Encompasses The Following: A. Size and Shape of PopulationArlene DaroNo ratings yet
- Muscular Triangles of The NeckDocument3 pagesMuscular Triangles of The NeckSam TagardaNo ratings yet
- IPC in Family PlanningDocument12 pagesIPC in Family PlanningHari MurtiNo ratings yet
- Job Hazard AnalysisDocument1 pageJob Hazard AnalysisZaul tatingNo ratings yet
- ..Document11 pages..Rizka Nur FadhilahNo ratings yet
- S100X220YAJ Panduit Datasheet 5314981Document2 pagesS100X220YAJ Panduit Datasheet 5314981Ilham MaurizaNo ratings yet
- Cadet College Skardu One Year Model Question PaperDocument5 pagesCadet College Skardu One Year Model Question PaperashrafNo ratings yet
- GRES Integrated Energy Storage SystemDocument33 pagesGRES Integrated Energy Storage SystemVadim PopovichNo ratings yet
- CSF PDFDocument58 pagesCSF PDFVas KannanNo ratings yet
- Trial Salary SlipDocument5 pagesTrial Salary SlipTvs12346No ratings yet
- Dec. 4 2021 Bldg. Tech ReviewDocument58 pagesDec. 4 2021 Bldg. Tech Reviewadyjoy antonioNo ratings yet
- Microbial Ecology of Sourdough Fermentations: Diverse or Uniform?Document19 pagesMicrobial Ecology of Sourdough Fermentations: Diverse or Uniform?roadrunner100% (1)
- Short Table of Muscle Control Exercises - The MaxaldingDocument48 pagesShort Table of Muscle Control Exercises - The MaxaldingHugo Mantilla90% (10)
- Brochure DM96Document12 pagesBrochure DM96Paul Avelino CallupeNo ratings yet
- Model: Stored Energy Solutions For A Demanding World: Dimensions MM InchDocument2 pagesModel: Stored Energy Solutions For A Demanding World: Dimensions MM Incheddywidjaya9No ratings yet
- Safeway SWOT AnalysisDocument9 pagesSafeway SWOT AnalysisAlbertWhatmoughNo ratings yet
- CHINT Installation Operation Manual For Inverter of 50-60KTLDocument98 pagesCHINT Installation Operation Manual For Inverter of 50-60KTLr.pimentel.souzaNo ratings yet
- Department of Education: Learning Activity SheetDocument7 pagesDepartment of Education: Learning Activity SheetKaren May UrlandaNo ratings yet
- Gothic Arch Tracing PDFDocument9 pagesGothic Arch Tracing PDFSimran SahniNo ratings yet
- Acupressure Points GuidelinesDocument6 pagesAcupressure Points Guidelinesshahisk100% (1)
- Kiambu CidpDocument342 pagesKiambu CidpCharles ZihiNo ratings yet
- Module 7Document11 pagesModule 7Arlyn DatuinNo ratings yet
- Benzene - It'S Characteristics and Safety in Handling, Storing & TransportationDocument6 pagesBenzene - It'S Characteristics and Safety in Handling, Storing & TransportationEhab SaadNo ratings yet
- Bicycle ProjectDocument4 pagesBicycle Projectgaming channelNo ratings yet
- Sentinel Collim Rev1.2 CompressedDocument2 pagesSentinel Collim Rev1.2 CompressedBauyrzhanNo ratings yet