Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5825)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Interpretation Cheat Sheet: VT SVTDocument1 pageInterpretation Cheat Sheet: VT SVTTracy Pope100% (1)
- CCRN AACN PremiumQs PDF PDFDocument70 pagesCCRN AACN PremiumQs PDF PDFTracy Pope100% (3)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Interpretation Cheat Sheet: V A V 20 ECG 30 40 Sys 10 15 ECG A X V yDocument1 pageInterpretation Cheat Sheet: V A V 20 ECG 30 40 Sys 10 15 ECG A X V yTracy PopeNo ratings yet
- Study Guide PathoPhysiology UCLA N 230 ADocument27 pagesStudy Guide PathoPhysiology UCLA N 230 ATracy Pope100% (1)
- New AntibioticsDocument4 pagesNew AntibioticsMylz MendozaNo ratings yet
- Infectious Diseases IDocument7 pagesInfectious Diseases ITiff VoNo ratings yet
- ACLS H:Ts IdentifyandTxDocument1 pageACLS H:Ts IdentifyandTxTracy PopeNo ratings yet
- See Full Prescribing Information For Complete Boxed WarningDocument22 pagesSee Full Prescribing Information For Complete Boxed WarningTracy PopeNo ratings yet
- Clinical Cheat Sheet: Radiographic AssessmentDocument1 pageClinical Cheat Sheet: Radiographic AssessmentTracy PopeNo ratings yet
- Campos Det. Impostos - Cadastro de ItensDocument201 pagesCampos Det. Impostos - Cadastro de ItensJônatasNo ratings yet
- Table 3. Vulvovaginal Candidiasis Treatment Options: Fluconazole 150mg PO Stat (1B)Document2 pagesTable 3. Vulvovaginal Candidiasis Treatment Options: Fluconazole 150mg PO Stat (1B)neleaNo ratings yet
- Lincosamides (Pharmacology of Antibiotics) - Group 6 PresentationDocument19 pagesLincosamides (Pharmacology of Antibiotics) - Group 6 PresentationGelmark OlivaresNo ratings yet
- RX Drugs (Controlled/Loose/Expensive/Dangerous) : Digestive Enzyme SupplementDocument9 pagesRX Drugs (Controlled/Loose/Expensive/Dangerous) : Digestive Enzyme SupplementEmmanuelle NazarenoNo ratings yet
- Obat TunggalDocument2 pagesObat TunggalAlexander PanduNo ratings yet
- 3 Konsep Terapi ARVDocument65 pages3 Konsep Terapi ARVkristinaNo ratings yet
- 1 Classification of The AntibioticsDocument5 pages1 Classification of The AntibioticsRahma WatiNo ratings yet
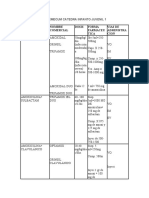
- Antibioticos Nombre Comercial Dosis Forma Farmaceu Tica Vias de Administra CionDocument10 pagesAntibioticos Nombre Comercial Dosis Forma Farmaceu Tica Vias de Administra CionLUCRECIA SUAREZ MORENONo ratings yet
- SCI 8008SEF Medical Microbiology & Virology II - Lecture 10 - OLEDocument70 pagesSCI 8008SEF Medical Microbiology & Virology II - Lecture 10 - OLEYY CheungNo ratings yet
- Dairy Trisensor Leaflet BD 1 PDFDocument2 pagesDairy Trisensor Leaflet BD 1 PDFthian_31No ratings yet
- Antibiotik (Lengkap) - Dr. HamzahDocument117 pagesAntibiotik (Lengkap) - Dr. HamzahLusi MunawarohNo ratings yet
- Anti-Fungal Compound Library (96-Well) : Product DetailsDocument1 pageAnti-Fungal Compound Library (96-Well) : Product DetailsSenuke TestNo ratings yet
- Antimikroba 2014Document36 pagesAntimikroba 2014Stella ChristyNo ratings yet
- Pharmacology Assignment 2Document3 pagesPharmacology Assignment 2Shamantha Santhana KrishnanNo ratings yet
- Antimicrobial / Antifungal Susceptibility TestingDocument6 pagesAntimicrobial / Antifungal Susceptibility TestingKetevan MigriauliNo ratings yet
- Table: Selected Antibacterial Antibiotics Antibiotics THAT . Mechanism of Action Names of Drugs Notes and ProblemsDocument4 pagesTable: Selected Antibacterial Antibiotics Antibiotics THAT . Mechanism of Action Names of Drugs Notes and ProblemsTJNo ratings yet
- DR TB Treatment Guideline of Timor Leste - REVISED 3 March 2021Document13 pagesDR TB Treatment Guideline of Timor Leste - REVISED 3 March 2021Yoan Manuel Ruiz ArencibiaNo ratings yet
- RX Meds 2Document3 pagesRX Meds 2Carla PulgarNo ratings yet
- Tabel Zona Sensitivitas Antibiotik: 1. Enterobactericeae (Klebsiella SP., E.coli, Proteus SP.,)Document7 pagesTabel Zona Sensitivitas Antibiotik: 1. Enterobactericeae (Klebsiella SP., E.coli, Proteus SP.,)puriartini-1No ratings yet
- V 6.1 EUCAST QC Tables Routine and Extended QCDocument18 pagesV 6.1 EUCAST QC Tables Routine and Extended QCLê Phuong MaiNo ratings yet
- Beta LactamDocument2 pagesBeta LactamefewtrNo ratings yet
- Peta Semester Rsud Bangil Tahun 2018Document3 pagesPeta Semester Rsud Bangil Tahun 2018pkpo dktNo ratings yet
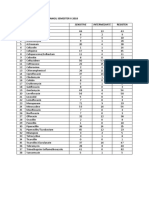
- Peta Antibiotika Rsud Bangil Semester Ii 2018 NO. Jenis Antibiotika ResistenDocument2 pagesPeta Antibiotika Rsud Bangil Semester Ii 2018 NO. Jenis Antibiotika Resistenpkpo dktNo ratings yet
- Pseudomonas Aeruginosa. Effective: Antibiotics by ClassDocument4 pagesPseudomonas Aeruginosa. Effective: Antibiotics by ClassDocFrankNo ratings yet
- Aminoglycosides: Aminoglycoside Is CategoryDocument6 pagesAminoglycosides: Aminoglycoside Is CategoryAnonymous RJwbBCkrHNo ratings yet
- Antibiotic IDocument9 pagesAntibiotic Iglorija71No ratings yet
- TTB Dtest SP-NT Deteclev 0409e2 PDFDocument3 pagesTTB Dtest SP-NT Deteclev 0409e2 PDFTairine AranhaNo ratings yet
- Antibiotics Quick ReviewDocument5 pagesAntibiotics Quick Reviewpranjl100% (5)