
Most Common Complication: Sabay Sila
Most Common Complication: Sabay Sila
You might also like
- Hijama Consultation FormDocument2 pagesHijama Consultation Formdentistsaif100% (1)
- 9 Topnotch Internal Medicine Superexampdf PDFDocument95 pages9 Topnotch Internal Medicine Superexampdf PDFSheryl Layne Lao-Sebrio100% (1)
- Microbiology and Parasitology ReviewerDocument4 pagesMicrobiology and Parasitology ReviewerChrister Jon AcostaNo ratings yet
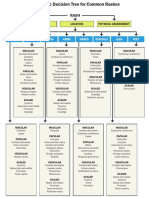
- WK 5 Rash Decision TreeDocument1 pageWK 5 Rash Decision TreeBetsy Brown ByersmithNo ratings yet
- Print Outs PDFDocument7 pagesPrint Outs PDFShanine Alexia CordovezNo ratings yet
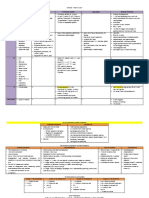
- Disease Causative Agent Diagnosis Classification/ S&S TreatmentDocument4 pagesDisease Causative Agent Diagnosis Classification/ S&S Treatmentfreya_28No ratings yet
- 01 Intro Pcol-MergedDocument19 pages01 Intro Pcol-MergedlumpiaNo ratings yet
- Anticoagulants ParamedDocument20 pagesAnticoagulants ParamedManikanta GupthaNo ratings yet
- Cardiovascular SystemDocument26 pagesCardiovascular SystemJenny Torreda100% (1)
- Li 3 Muscles and MovementsDocument3 pagesLi 3 Muscles and MovementsMei BejeranoNo ratings yet
- Decreased Hemoglobin Available For Erythrocytes Microcytic, Hypochromic Anemia More Hemoglobin Available For Erythrocytes Macrocytic AnemiaDocument2 pagesDecreased Hemoglobin Available For Erythrocytes Microcytic, Hypochromic Anemia More Hemoglobin Available For Erythrocytes Macrocytic AnemiaIB leaksNo ratings yet
- Electrolyte Imbalances Causes: Signs & Symptoms:: Physical Exam: Lab FindingsDocument4 pagesElectrolyte Imbalances Causes: Signs & Symptoms:: Physical Exam: Lab Findingsworleyb83No ratings yet
- Neuro Written III TablesDocument5 pagesNeuro Written III TablesSolomon Seth SallforsNo ratings yet
- Concept MapDocument4 pagesConcept MapDud AccNo ratings yet
- Dysrhythmias 1: Cardiac Conduc1on System Rhythm Strip Recogni1onDocument4 pagesDysrhythmias 1: Cardiac Conduc1on System Rhythm Strip Recogni1ontantalizin marieNo ratings yet
- Microscopic ExaminationDocument9 pagesMicroscopic ExaminationMariella DingleNo ratings yet
- Thorax and LungsDocument2 pagesThorax and LungsHNo ratings yet
- HEMATOLOGYDocument36 pagesHEMATOLOGYMA. ANDREA NICOLE BITOINNo ratings yet
- Gastro Intestinal Disorders:: Kawasaki DiseaseDocument6 pagesGastro Intestinal Disorders:: Kawasaki DiseaseJoanna TaylanNo ratings yet
- Patho. Reviewer On Cellular InjuryDocument21 pagesPatho. Reviewer On Cellular InjurySeff CausapinNo ratings yet
- MnemonicsDocument10 pagesMnemonicsRichard GarciaNo ratings yet
- PharmacyDocument16 pagesPharmacyJow RamosNo ratings yet
- Dingcong, Phoebe Joy M. BSN 1 - A Fundamentals of NursingDocument6 pagesDingcong, Phoebe Joy M. BSN 1 - A Fundamentals of NursingDee JeonNo ratings yet
- Diana's Renal DiseasesDocument9 pagesDiana's Renal DiseasesdhyltonNo ratings yet
- Hi Stop Hath Ology 2Document22 pagesHi Stop Hath Ology 2vivek govardhanamNo ratings yet
- Cranial+Nerves 1styearDocument2 pagesCranial+Nerves 1styearashleyyanez3100% (1)
- Cardio Block 3Document62 pagesCardio Block 3Maya LaPradeNo ratings yet
- Micro Chart #3 - Italics OnlyDocument27 pagesMicro Chart #3 - Italics Onlyapi-26938624100% (1)
- Miñano - (OS 204) PN 2 - Skull and MandibleDocument2 pagesMiñano - (OS 204) PN 2 - Skull and MandibleMarion Rodelle MiñanoNo ratings yet
- Pathogens of The Vagina-Annie Espinosa - This Is The Revised VersionDocument1 pagePathogens of The Vagina-Annie Espinosa - This Is The Revised VersionMicroposterNo ratings yet
- Low BP - Decreased Cardiac Output - Improved Renal Blood FlowDocument2 pagesLow BP - Decreased Cardiac Output - Improved Renal Blood Flowtantalizin marieNo ratings yet
- Shanz - Pedia Ii 2.05Document3 pagesShanz - Pedia Ii 2.05Petrina XuNo ratings yet
- Communicable Disease Nursing Part II Diseases (1) 2Document21 pagesCommunicable Disease Nursing Part II Diseases (1) 2MK LiNo ratings yet
- Pharma CompilationDocument32 pagesPharma CompilationJustin Kaye DariaNo ratings yet
- 1 Ge Stimulations Mast Cell Degeneration Asthma AttackDocument4 pages1 Ge Stimulations Mast Cell Degeneration Asthma Attacknebbie06No ratings yet
- Pharma - SkinDocument8 pagesPharma - Skinreference books100% (1)
- Electrolytes ImbalancesDocument4 pagesElectrolytes ImbalancesPeter John Ruiz100% (1)
- Case Presentation: Patient Chart - Mary JohnsonDocument12 pagesCase Presentation: Patient Chart - Mary Johnsonivoneeh_16100% (1)
- Bacterial Pneumonia PharmacologyDocument70 pagesBacterial Pneumonia PharmacologyMarc Imhotep Cray, M.D.No ratings yet
- Para Neoplastic SyndromeDocument5 pagesPara Neoplastic SyndromeSamir Sarkar100% (1)
- Approach To Anemia: - Reticulocyte Count Is Most Important TestDocument15 pagesApproach To Anemia: - Reticulocyte Count Is Most Important TestJanella SuerteNo ratings yet
- Infectious Disease (Part 1) : Viral DiseasesDocument11 pagesInfectious Disease (Part 1) : Viral Diseasesmiguel gaquitNo ratings yet
- Pathophysiology of PneumoniaDocument1 pagePathophysiology of PneumoniaMary Mathel Del RosarioNo ratings yet
- Finals Trans (Hema)Document16 pagesFinals Trans (Hema)Ayesha CaragNo ratings yet
- Hema Part 3 Final PDFDocument188 pagesHema Part 3 Final PDFH.B.ANo ratings yet
- Anemia Flow ChartDocument1 pageAnemia Flow ChartCynthiaNo ratings yet
- Do Not Copy Without Permission This Property Is Governed by Republic Act No. 386, Title II, Chapter 1, Article 429 of Property Law of The PhilippinesDocument11 pagesDo Not Copy Without Permission This Property Is Governed by Republic Act No. 386, Title II, Chapter 1, Article 429 of Property Law of The PhilippinesChrissa Mae Tumaliuan CatindoyNo ratings yet
- Pharmacotherapy of VTEDocument80 pagesPharmacotherapy of VTEAbera JamboNo ratings yet
- GI + Renal OSCE: AMSA Edinburgh X IMU Y4Document41 pagesGI + Renal OSCE: AMSA Edinburgh X IMU Y4Abby LiewNo ratings yet
- Respiratory Tract InfectionsDocument1 pageRespiratory Tract InfectionsShannon RamsumairNo ratings yet
- Communicable Disease: Clean TechniqueDocument13 pagesCommunicable Disease: Clean TechniqueRaquel M. Mendoza0% (1)
- CURRENT Diagnosis & Treatment: Nephrology & Hypertension, 2009 Chapter 46. Cystic Diseases of TH e KidneyDocument1 pageCURRENT Diagnosis & Treatment: Nephrology & Hypertension, 2009 Chapter 46. Cystic Diseases of TH e KidneyFate ChanNo ratings yet
- Dengue Virus: DescriptionDocument12 pagesDengue Virus: Descriptionpedia blue bookNo ratings yet
- RevalidaDocument5 pagesRevalidaHawkins FletcherNo ratings yet
- Hematological Systems - Lecture NotesDocument15 pagesHematological Systems - Lecture NotesAmiel Francisco ReyesNo ratings yet
- Covid 19 (Case 1)Document53 pagesCovid 19 (Case 1)cendy andestriaNo ratings yet
- Group Case Study - Pulmonary TBDocument8 pagesGroup Case Study - Pulmonary TBCj NiñalNo ratings yet
- Cardiac ImDocument22 pagesCardiac ImmetNo ratings yet
- Concept MapDocument4 pagesConcept MapMersiya SarapuddinNo ratings yet
- NURSING CARE OF ADULTS II: Passbooks Study GuideFrom EverandNURSING CARE OF ADULTS II: Passbooks Study GuideNo ratings yet
- Community in Tables AllTalabaDocument14 pagesCommunity in Tables AllTalabaAhmed MansourNo ratings yet
- Del Rosario Ryan D. BSN 4C1-7 Mr. Daniel Mon Mamanao: Measles Pre-Eruptive StageDocument5 pagesDel Rosario Ryan D. BSN 4C1-7 Mr. Daniel Mon Mamanao: Measles Pre-Eruptive Stageryandelrosario9yahooNo ratings yet
- Cardio - ECGDocument13 pagesCardio - ECGSheryl Layne Lao-SebrioNo ratings yet
- Patho OB - Breech DeliveryDocument7 pagesPatho OB - Breech DeliverySheryl Layne Lao-SebrioNo ratings yet
- 1.acute Respiratory Disease: DDX: Kawasaki, Strep. InfectionDocument5 pages1.acute Respiratory Disease: DDX: Kawasaki, Strep. InfectionSheryl Layne Lao-SebrioNo ratings yet
- Finals PHARMACOTHERAPHY OF DIABETES MELLITUS 2017Document8 pagesFinals PHARMACOTHERAPHY OF DIABETES MELLITUS 2017Sheryl Layne Lao-SebrioNo ratings yet
- 3.0 Grand Physiology Finals Compilation - Batch 2017Document89 pages3.0 Grand Physiology Finals Compilation - Batch 2017Sheryl Layne Lao-SebrioNo ratings yet
- EndoDocument8 pagesEndoSheryl Layne Lao-SebrioNo ratings yet
- Death in Infancy and Young Children: Dato' DR Zahari Bin NoorDocument32 pagesDeath in Infancy and Young Children: Dato' DR Zahari Bin NoorfahmiNo ratings yet
- DD FeverDocument9 pagesDD FeverAnisa WahyuniartiNo ratings yet
- Nama ObatDocument23 pagesNama ObatIsmul 'D' SadlyNo ratings yet
- Stok Opname Ok Feb 2021Document14 pagesStok Opname Ok Feb 2021fiannysjahjadiNo ratings yet
- Meropenem Drug StudyDocument2 pagesMeropenem Drug StudyKullin Rain100% (1)
- ةلجسملا تارضحتسملا Tablets: ليجستلا خيرات مقر ليجستلا Trade Name Trade Name NoDocument2 pagesةلجسملا تارضحتسملا Tablets: ليجستلا خيرات مقر ليجستلا Trade Name Trade Name Noahmed kindiNo ratings yet
- Prescription Medications&Weight GainDocument6 pagesPrescription Medications&Weight GainLorena IbarrolaNo ratings yet
- 40th DITF Catalogue 2016Document85 pages40th DITF Catalogue 2016Michael HansenNo ratings yet
- Nursing Care Plan For: Diabetes, High Blood Sugar, Hyperglycemia, DKA, Diabetic Ketoacidosis, Fluid and Electrolytes ImbalanceDocument2 pagesNursing Care Plan For: Diabetes, High Blood Sugar, Hyperglycemia, DKA, Diabetic Ketoacidosis, Fluid and Electrolytes ImbalanceFhai EscioNo ratings yet
- Daftar Obat Yang Dimusnahkan Tahun 2020Document10 pagesDaftar Obat Yang Dimusnahkan Tahun 2020Agie ArieNo ratings yet
- POLYMYOLITISDocument4 pagesPOLYMYOLITISAlexa Lexington Rae ZagadoNo ratings yet
- ProposalDocument3 pagesProposalFebry LuthunananaNo ratings yet
- Abortion Womens Clinic in Randburg 0736613276Document2 pagesAbortion Womens Clinic in Randburg 0736613276MaamaTitiNo ratings yet
- GonorrheaDocument9 pagesGonorrheaPencenk AzznewNo ratings yet
- Kantor Cabang: BANJARMASIN - 1701 FKTP: Kertak Hanyar - 17040601Document78 pagesKantor Cabang: BANJARMASIN - 1701 FKTP: Kertak Hanyar - 17040601Ic-tika Siee ChuabbieNo ratings yet
- Exfoliative CheilitisDocument2 pagesExfoliative CheilitiswyndinkNo ratings yet
- Evidence-Based Case Report Ceftriaxone Verus Penicillin For Treatment of Leptopspirosis in AdultsDocument7 pagesEvidence-Based Case Report Ceftriaxone Verus Penicillin For Treatment of Leptopspirosis in AdultsWinson JosNo ratings yet
- W LDocument30 pagesW LAditya PrabawaNo ratings yet
- Form Self Assessment Review 144 Diagnosa Layanan Primer: 1 Abortus Spontan Komplit O03.9 707Document78 pagesForm Self Assessment Review 144 Diagnosa Layanan Primer: 1 Abortus Spontan Komplit O03.9 707Rani AprianiNo ratings yet
- Cancer Drugs Drugs Indication Adverse Effects Interaction and ContraindicationDocument5 pagesCancer Drugs Drugs Indication Adverse Effects Interaction and ContraindicationOndari gisemba OSINDENo ratings yet
- What Causes Nettle Rash?Document2 pagesWhat Causes Nettle Rash?Ardave Laurente100% (1)
- Endokarditis, Miokarditis Perikarditis: Blok KardiovaskularDocument31 pagesEndokarditis, Miokarditis Perikarditis: Blok KardiovaskularTiara RamliNo ratings yet
- Tarif RS Yarsi RevisiDocument20 pagesTarif RS Yarsi RevisiWhen Ren DhyNo ratings yet
- Name of Drug Classification Action Indication Side Effects Intervention and EvaluationDocument3 pagesName of Drug Classification Action Indication Side Effects Intervention and EvaluationMikz JocomNo ratings yet
- What To Expect After VaccinationsDocument2 pagesWhat To Expect After Vaccinationsmunshimbwe munshimbweNo ratings yet
- TonsillitisDocument44 pagesTonsillitisBheru Lal100% (1)
- Atsp Re:: DR Gillian Jackson DR Fran Bennett DR Tom HannanDocument24 pagesAtsp Re:: DR Gillian Jackson DR Fran Bennett DR Tom HannanSagarJobanNo ratings yet
- iTIJ:: P4Yicai. Etfal - Uati OnDocument4 pagesiTIJ:: P4Yicai. Etfal - Uati OnBartolome MercadoNo ratings yet
- Ada-Montefiore Dka Protcol Version 3.0 5 22 20Document3 pagesAda-Montefiore Dka Protcol Version 3.0 5 22 20ibnuNo ratings yet





























































































Download as pdf or txt
You might also like
- Hijama Consultation FormDocument2 pagesHijama Consultation Formdentistsaif100% (1)
- 9 Topnotch Internal Medicine Superexampdf PDFDocument95 pages9 Topnotch Internal Medicine Superexampdf PDFSheryl Layne Lao-Sebrio100% (1)
- Microbiology and Parasitology ReviewerDocument4 pagesMicrobiology and Parasitology ReviewerChrister Jon AcostaNo ratings yet
- WK 5 Rash Decision TreeDocument1 pageWK 5 Rash Decision TreeBetsy Brown ByersmithNo ratings yet
- Print Outs PDFDocument7 pagesPrint Outs PDFShanine Alexia CordovezNo ratings yet
- Disease Causative Agent Diagnosis Classification/ S&S TreatmentDocument4 pagesDisease Causative Agent Diagnosis Classification/ S&S Treatmentfreya_28No ratings yet
- 01 Intro Pcol-MergedDocument19 pages01 Intro Pcol-MergedlumpiaNo ratings yet
- Anticoagulants ParamedDocument20 pagesAnticoagulants ParamedManikanta GupthaNo ratings yet
- Cardiovascular SystemDocument26 pagesCardiovascular SystemJenny Torreda100% (1)
- Li 3 Muscles and MovementsDocument3 pagesLi 3 Muscles and MovementsMei BejeranoNo ratings yet
- Decreased Hemoglobin Available For Erythrocytes Microcytic, Hypochromic Anemia More Hemoglobin Available For Erythrocytes Macrocytic AnemiaDocument2 pagesDecreased Hemoglobin Available For Erythrocytes Microcytic, Hypochromic Anemia More Hemoglobin Available For Erythrocytes Macrocytic AnemiaIB leaksNo ratings yet
- Electrolyte Imbalances Causes: Signs & Symptoms:: Physical Exam: Lab FindingsDocument4 pagesElectrolyte Imbalances Causes: Signs & Symptoms:: Physical Exam: Lab Findingsworleyb83No ratings yet
- Neuro Written III TablesDocument5 pagesNeuro Written III TablesSolomon Seth SallforsNo ratings yet
- Concept MapDocument4 pagesConcept MapDud AccNo ratings yet
- Dysrhythmias 1: Cardiac Conduc1on System Rhythm Strip Recogni1onDocument4 pagesDysrhythmias 1: Cardiac Conduc1on System Rhythm Strip Recogni1ontantalizin marieNo ratings yet
- Microscopic ExaminationDocument9 pagesMicroscopic ExaminationMariella DingleNo ratings yet
- Thorax and LungsDocument2 pagesThorax and LungsHNo ratings yet
- HEMATOLOGYDocument36 pagesHEMATOLOGYMA. ANDREA NICOLE BITOINNo ratings yet
- Gastro Intestinal Disorders:: Kawasaki DiseaseDocument6 pagesGastro Intestinal Disorders:: Kawasaki DiseaseJoanna TaylanNo ratings yet
- Patho. Reviewer On Cellular InjuryDocument21 pagesPatho. Reviewer On Cellular InjurySeff CausapinNo ratings yet
- MnemonicsDocument10 pagesMnemonicsRichard GarciaNo ratings yet
- PharmacyDocument16 pagesPharmacyJow RamosNo ratings yet
- Dingcong, Phoebe Joy M. BSN 1 - A Fundamentals of NursingDocument6 pagesDingcong, Phoebe Joy M. BSN 1 - A Fundamentals of NursingDee JeonNo ratings yet
- Diana's Renal DiseasesDocument9 pagesDiana's Renal DiseasesdhyltonNo ratings yet
- Hi Stop Hath Ology 2Document22 pagesHi Stop Hath Ology 2vivek govardhanamNo ratings yet
- Cranial+Nerves 1styearDocument2 pagesCranial+Nerves 1styearashleyyanez3100% (1)
- Cardio Block 3Document62 pagesCardio Block 3Maya LaPradeNo ratings yet
- Micro Chart #3 - Italics OnlyDocument27 pagesMicro Chart #3 - Italics Onlyapi-26938624100% (1)
- Miñano - (OS 204) PN 2 - Skull and MandibleDocument2 pagesMiñano - (OS 204) PN 2 - Skull and MandibleMarion Rodelle MiñanoNo ratings yet
- Pathogens of The Vagina-Annie Espinosa - This Is The Revised VersionDocument1 pagePathogens of The Vagina-Annie Espinosa - This Is The Revised VersionMicroposterNo ratings yet
- Low BP - Decreased Cardiac Output - Improved Renal Blood FlowDocument2 pagesLow BP - Decreased Cardiac Output - Improved Renal Blood Flowtantalizin marieNo ratings yet
- Shanz - Pedia Ii 2.05Document3 pagesShanz - Pedia Ii 2.05Petrina XuNo ratings yet
- Communicable Disease Nursing Part II Diseases (1) 2Document21 pagesCommunicable Disease Nursing Part II Diseases (1) 2MK LiNo ratings yet
- Pharma CompilationDocument32 pagesPharma CompilationJustin Kaye DariaNo ratings yet
- 1 Ge Stimulations Mast Cell Degeneration Asthma AttackDocument4 pages1 Ge Stimulations Mast Cell Degeneration Asthma Attacknebbie06No ratings yet
- Pharma - SkinDocument8 pagesPharma - Skinreference books100% (1)
- Electrolytes ImbalancesDocument4 pagesElectrolytes ImbalancesPeter John Ruiz100% (1)
- Case Presentation: Patient Chart - Mary JohnsonDocument12 pagesCase Presentation: Patient Chart - Mary Johnsonivoneeh_16100% (1)
- Bacterial Pneumonia PharmacologyDocument70 pagesBacterial Pneumonia PharmacologyMarc Imhotep Cray, M.D.No ratings yet
- Para Neoplastic SyndromeDocument5 pagesPara Neoplastic SyndromeSamir Sarkar100% (1)
- Approach To Anemia: - Reticulocyte Count Is Most Important TestDocument15 pagesApproach To Anemia: - Reticulocyte Count Is Most Important TestJanella SuerteNo ratings yet
- Infectious Disease (Part 1) : Viral DiseasesDocument11 pagesInfectious Disease (Part 1) : Viral Diseasesmiguel gaquitNo ratings yet
- Pathophysiology of PneumoniaDocument1 pagePathophysiology of PneumoniaMary Mathel Del RosarioNo ratings yet
- Finals Trans (Hema)Document16 pagesFinals Trans (Hema)Ayesha CaragNo ratings yet
- Hema Part 3 Final PDFDocument188 pagesHema Part 3 Final PDFH.B.ANo ratings yet
- Anemia Flow ChartDocument1 pageAnemia Flow ChartCynthiaNo ratings yet
- Do Not Copy Without Permission This Property Is Governed by Republic Act No. 386, Title II, Chapter 1, Article 429 of Property Law of The PhilippinesDocument11 pagesDo Not Copy Without Permission This Property Is Governed by Republic Act No. 386, Title II, Chapter 1, Article 429 of Property Law of The PhilippinesChrissa Mae Tumaliuan CatindoyNo ratings yet
- Pharmacotherapy of VTEDocument80 pagesPharmacotherapy of VTEAbera JamboNo ratings yet
- GI + Renal OSCE: AMSA Edinburgh X IMU Y4Document41 pagesGI + Renal OSCE: AMSA Edinburgh X IMU Y4Abby LiewNo ratings yet
- Respiratory Tract InfectionsDocument1 pageRespiratory Tract InfectionsShannon RamsumairNo ratings yet
- Communicable Disease: Clean TechniqueDocument13 pagesCommunicable Disease: Clean TechniqueRaquel M. Mendoza0% (1)
- CURRENT Diagnosis & Treatment: Nephrology & Hypertension, 2009 Chapter 46. Cystic Diseases of TH e KidneyDocument1 pageCURRENT Diagnosis & Treatment: Nephrology & Hypertension, 2009 Chapter 46. Cystic Diseases of TH e KidneyFate ChanNo ratings yet
- Dengue Virus: DescriptionDocument12 pagesDengue Virus: Descriptionpedia blue bookNo ratings yet
- RevalidaDocument5 pagesRevalidaHawkins FletcherNo ratings yet
- Hematological Systems - Lecture NotesDocument15 pagesHematological Systems - Lecture NotesAmiel Francisco ReyesNo ratings yet
- Covid 19 (Case 1)Document53 pagesCovid 19 (Case 1)cendy andestriaNo ratings yet
- Group Case Study - Pulmonary TBDocument8 pagesGroup Case Study - Pulmonary TBCj NiñalNo ratings yet
- Cardiac ImDocument22 pagesCardiac ImmetNo ratings yet
- Concept MapDocument4 pagesConcept MapMersiya SarapuddinNo ratings yet
- NURSING CARE OF ADULTS II: Passbooks Study GuideFrom EverandNURSING CARE OF ADULTS II: Passbooks Study GuideNo ratings yet
- Community in Tables AllTalabaDocument14 pagesCommunity in Tables AllTalabaAhmed MansourNo ratings yet
- Del Rosario Ryan D. BSN 4C1-7 Mr. Daniel Mon Mamanao: Measles Pre-Eruptive StageDocument5 pagesDel Rosario Ryan D. BSN 4C1-7 Mr. Daniel Mon Mamanao: Measles Pre-Eruptive Stageryandelrosario9yahooNo ratings yet
- Cardio - ECGDocument13 pagesCardio - ECGSheryl Layne Lao-SebrioNo ratings yet
- Patho OB - Breech DeliveryDocument7 pagesPatho OB - Breech DeliverySheryl Layne Lao-SebrioNo ratings yet
- 1.acute Respiratory Disease: DDX: Kawasaki, Strep. InfectionDocument5 pages1.acute Respiratory Disease: DDX: Kawasaki, Strep. InfectionSheryl Layne Lao-SebrioNo ratings yet
- Finals PHARMACOTHERAPHY OF DIABETES MELLITUS 2017Document8 pagesFinals PHARMACOTHERAPHY OF DIABETES MELLITUS 2017Sheryl Layne Lao-SebrioNo ratings yet
- 3.0 Grand Physiology Finals Compilation - Batch 2017Document89 pages3.0 Grand Physiology Finals Compilation - Batch 2017Sheryl Layne Lao-SebrioNo ratings yet
- EndoDocument8 pagesEndoSheryl Layne Lao-SebrioNo ratings yet
- Death in Infancy and Young Children: Dato' DR Zahari Bin NoorDocument32 pagesDeath in Infancy and Young Children: Dato' DR Zahari Bin NoorfahmiNo ratings yet
- DD FeverDocument9 pagesDD FeverAnisa WahyuniartiNo ratings yet
- Nama ObatDocument23 pagesNama ObatIsmul 'D' SadlyNo ratings yet
- Stok Opname Ok Feb 2021Document14 pagesStok Opname Ok Feb 2021fiannysjahjadiNo ratings yet
- Meropenem Drug StudyDocument2 pagesMeropenem Drug StudyKullin Rain100% (1)
- ةلجسملا تارضحتسملا Tablets: ليجستلا خيرات مقر ليجستلا Trade Name Trade Name NoDocument2 pagesةلجسملا تارضحتسملا Tablets: ليجستلا خيرات مقر ليجستلا Trade Name Trade Name Noahmed kindiNo ratings yet
- Prescription Medications&Weight GainDocument6 pagesPrescription Medications&Weight GainLorena IbarrolaNo ratings yet
- 40th DITF Catalogue 2016Document85 pages40th DITF Catalogue 2016Michael HansenNo ratings yet
- Nursing Care Plan For: Diabetes, High Blood Sugar, Hyperglycemia, DKA, Diabetic Ketoacidosis, Fluid and Electrolytes ImbalanceDocument2 pagesNursing Care Plan For: Diabetes, High Blood Sugar, Hyperglycemia, DKA, Diabetic Ketoacidosis, Fluid and Electrolytes ImbalanceFhai EscioNo ratings yet
- Daftar Obat Yang Dimusnahkan Tahun 2020Document10 pagesDaftar Obat Yang Dimusnahkan Tahun 2020Agie ArieNo ratings yet
- POLYMYOLITISDocument4 pagesPOLYMYOLITISAlexa Lexington Rae ZagadoNo ratings yet
- ProposalDocument3 pagesProposalFebry LuthunananaNo ratings yet
- Abortion Womens Clinic in Randburg 0736613276Document2 pagesAbortion Womens Clinic in Randburg 0736613276MaamaTitiNo ratings yet
- GonorrheaDocument9 pagesGonorrheaPencenk AzznewNo ratings yet
- Kantor Cabang: BANJARMASIN - 1701 FKTP: Kertak Hanyar - 17040601Document78 pagesKantor Cabang: BANJARMASIN - 1701 FKTP: Kertak Hanyar - 17040601Ic-tika Siee ChuabbieNo ratings yet
- Exfoliative CheilitisDocument2 pagesExfoliative CheilitiswyndinkNo ratings yet
- Evidence-Based Case Report Ceftriaxone Verus Penicillin For Treatment of Leptopspirosis in AdultsDocument7 pagesEvidence-Based Case Report Ceftriaxone Verus Penicillin For Treatment of Leptopspirosis in AdultsWinson JosNo ratings yet
- W LDocument30 pagesW LAditya PrabawaNo ratings yet
- Form Self Assessment Review 144 Diagnosa Layanan Primer: 1 Abortus Spontan Komplit O03.9 707Document78 pagesForm Self Assessment Review 144 Diagnosa Layanan Primer: 1 Abortus Spontan Komplit O03.9 707Rani AprianiNo ratings yet
- Cancer Drugs Drugs Indication Adverse Effects Interaction and ContraindicationDocument5 pagesCancer Drugs Drugs Indication Adverse Effects Interaction and ContraindicationOndari gisemba OSINDENo ratings yet
- What Causes Nettle Rash?Document2 pagesWhat Causes Nettle Rash?Ardave Laurente100% (1)
- Endokarditis, Miokarditis Perikarditis: Blok KardiovaskularDocument31 pagesEndokarditis, Miokarditis Perikarditis: Blok KardiovaskularTiara RamliNo ratings yet
- Tarif RS Yarsi RevisiDocument20 pagesTarif RS Yarsi RevisiWhen Ren DhyNo ratings yet
- Name of Drug Classification Action Indication Side Effects Intervention and EvaluationDocument3 pagesName of Drug Classification Action Indication Side Effects Intervention and EvaluationMikz JocomNo ratings yet
- What To Expect After VaccinationsDocument2 pagesWhat To Expect After Vaccinationsmunshimbwe munshimbweNo ratings yet
- TonsillitisDocument44 pagesTonsillitisBheru Lal100% (1)
- Atsp Re:: DR Gillian Jackson DR Fran Bennett DR Tom HannanDocument24 pagesAtsp Re:: DR Gillian Jackson DR Fran Bennett DR Tom HannanSagarJobanNo ratings yet
- iTIJ:: P4Yicai. Etfal - Uati OnDocument4 pagesiTIJ:: P4Yicai. Etfal - Uati OnBartolome MercadoNo ratings yet
- Ada-Montefiore Dka Protcol Version 3.0 5 22 20Document3 pagesAda-Montefiore Dka Protcol Version 3.0 5 22 20ibnuNo ratings yet