Download as pdf or txt
You might also like
- Neurology High Yield Notes For Step 1Document25 pagesNeurology High Yield Notes For Step 1Lucykesh100% (8)
- 1.3 Describe Factors That May Impact Upon The Development of The Baby During: Pre-ConceptionDocument2 pages1.3 Describe Factors That May Impact Upon The Development of The Baby During: Pre-Conceptionjoel TorresNo ratings yet
- Brain DeathDocument45 pagesBrain DeathAdeNo ratings yet
- TBI ZamDocument67 pagesTBI ZamnafisyarifahNo ratings yet
- Distributive Shock 1Document41 pagesDistributive Shock 1Fuzi HannyNo ratings yet
- Nurkholis, DR., SpbsDocument72 pagesNurkholis, DR., SpbsRifa Nur MahmudahNo ratings yet
- Scleroza Sistemica Progresiva: SclerodermiaDocument87 pagesScleroza Sistemica Progresiva: SclerodermiaIulia Maria AgrigoroaieNo ratings yet
- Kul FCPPP GNMMPDocument151 pagesKul FCPPP GNMMPYehuda WibowoNo ratings yet
- Patofisiologi Stroke Iskemik IbnDocument14 pagesPatofisiologi Stroke Iskemik Ibnashwin kumarNo ratings yet
- Perinatal Asphyxia - Outline of Pathophysiology and Recent Trends in ManagementDocument31 pagesPerinatal Asphyxia - Outline of Pathophysiology and Recent Trends in Managementokwadha simionNo ratings yet
- Clinical Science StrokeDocument50 pagesClinical Science StrokeelsaputeriNo ratings yet
- SBRC General PrinciplesDocument51 pagesSBRC General Principlesdalia khamoNo ratings yet
- Kuliah Stroke Unram ArsipDocument75 pagesKuliah Stroke Unram ArsipAndina MarioNo ratings yet
- Neimy Kuliah Cedera OtakDocument45 pagesNeimy Kuliah Cedera OtakCahya RamadhanNo ratings yet
- 1 STROKE Kuliah UnizarDocument52 pages1 STROKE Kuliah UnizarBaiqLinaAnggrianNo ratings yet
- LP COB-Trimitha L.Document16 pagesLP COB-Trimitha L.Ciki ChicaNo ratings yet
- Kuliah StrokeDocument25 pagesKuliah Strokenoviaaulia15No ratings yet
- Kuliah StrokeDocument52 pagesKuliah StrokeJihan alifa RahmaNo ratings yet
- Pathophysiology of TBI 97Document51 pagesPathophysiology of TBI 97rajan kumarNo ratings yet
- Confusion MetabolicDocument43 pagesConfusion MetabolicYoumna ShaabanNo ratings yet
- Neurology: - Neuron: Nerve, Logos: Knowledge - Neurology: Deals With The Prevention, Therapy andDocument49 pagesNeurology: - Neuron: Nerve, Logos: Knowledge - Neurology: Deals With The Prevention, Therapy andis kimNo ratings yet
- Neuroimaging: Dr. Mashuri, SP - Rad (K) .,M.KesDocument61 pagesNeuroimaging: Dr. Mashuri, SP - Rad (K) .,M.KesGaluh EkaNo ratings yet
- Medical Surgical Nursing Review NotesDocument78 pagesMedical Surgical Nursing Review NotesLouie ParillaNo ratings yet
- WEBINAR Trauma Kepala PREMIER IDKI Mei 2020 FinalDocument130 pagesWEBINAR Trauma Kepala PREMIER IDKI Mei 2020 FinalAndiNo ratings yet
- Sirs and Sepsis Pasca TraumaDocument61 pagesSirs and Sepsis Pasca TraumahermanfirdausNo ratings yet
- 5A. Traumatic Brain InjuriesDocument242 pages5A. Traumatic Brain InjuriesMajed AlamiNo ratings yet
- (DONE) Peripheral LesionsDocument11 pages(DONE) Peripheral LesionsAstha Tusharbhai PatelNo ratings yet
- MBR 2019 - Pathology HandoutsDocument98 pagesMBR 2019 - Pathology HandoutsRgm UyNo ratings yet
- Leaflet Cushing SyndromeDocument2 pagesLeaflet Cushing SyndromesepthyaniNo ratings yet
- By Gilang Nispu SaputraDocument37 pagesBy Gilang Nispu SaputraMarogi Al AnsorianiNo ratings yet
- Cedera Otak BontangDocument65 pagesCedera Otak BontangAdelcawiduNo ratings yet
- Screening For Micro and Macrovascular ComplicationDocument38 pagesScreening For Micro and Macrovascular ComplicationRoby KieranNo ratings yet
- Medulla Compression AcuteDocument46 pagesMedulla Compression AcuteamiraNo ratings yet
- Manajemen Kegawatdaruratan Pada Syok Neurogenik - Medan - 2022Document41 pagesManajemen Kegawatdaruratan Pada Syok Neurogenik - Medan - 2022zubaidah pasaribuNo ratings yet
- Initial Diagnosis and Management of ComaDocument17 pagesInitial Diagnosis and Management of Comaguugle gogleNo ratings yet
- Genetic Testing Gor Mitochondrial DisordersDocument7 pagesGenetic Testing Gor Mitochondrial DisordersRora11No ratings yet
- Case MNGT On Cysto-TURPDocument86 pagesCase MNGT On Cysto-TURPAndelaliz SantiagoNo ratings yet
- Addison's Disease (Primary Adrenal Insufficiency)Document5 pagesAddison's Disease (Primary Adrenal Insufficiency)sunnnydayNo ratings yet
- Agni LP Stoke HimorogikDocument16 pagesAgni LP Stoke HimorogikagnydwiNo ratings yet
- Kul NBS 14 PDFDocument83 pagesKul NBS 14 PDFNia AishiteruNo ratings yet
- Cerebro Vascular Disease: "The Flowing of Blood" Stroke ApoplexyDocument34 pagesCerebro Vascular Disease: "The Flowing of Blood" Stroke ApoplexyLeo FernandoNo ratings yet
- Woc ModsDocument2 pagesWoc Modsika anggreitaNo ratings yet
- Acute ComaDocument16 pagesAcute ComaDean AccountNo ratings yet
- Stroke: Dr. Fidha Rahmayani, M.SC, SP.S Fakultas Kedokteran Universitas Lampung RS Abdul MulukDocument45 pagesStroke: Dr. Fidha Rahmayani, M.SC, SP.S Fakultas Kedokteran Universitas Lampung RS Abdul Mulukdhea nadhiaNo ratings yet
- Diabetic Neuropathy: Jurnal ReadingDocument23 pagesDiabetic Neuropathy: Jurnal ReadingSagu TechNo ratings yet
- Brain Death Role of Intensivist in Diagnosis and Preparation For Organ RetrievalDocument86 pagesBrain Death Role of Intensivist in Diagnosis and Preparation For Organ Retrievalharsha mummaka100% (1)
- Cva IschemicDocument53 pagesCva IschemicJuliatikaNo ratings yet
- Ischemic Heart Disease (ACS) THN LaluDocument40 pagesIschemic Heart Disease (ACS) THN LaluRangsiyo BeabeoNo ratings yet
- Compilation of MS NotesDocument81 pagesCompilation of MS Notesdis_is_meNo ratings yet
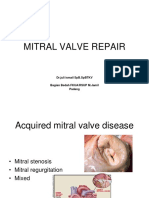
- Mitral Valve Repair: DR - Juli Ismail SPB - SPBTKV Bagian Bedah Fkua/Rsup M.Jamil PadangDocument22 pagesMitral Valve Repair: DR - Juli Ismail SPB - SPBTKV Bagian Bedah Fkua/Rsup M.Jamil PadangNova SuryatiNo ratings yet
- Spinal Cord Injury: Priza RazunipDocument71 pagesSpinal Cord Injury: Priza Razunipagus sukarnaNo ratings yet
- k20 - Stroke IskemikDocument35 pagesk20 - Stroke IskemikZikri Putra Lan LubisNo ratings yet
- By Thamrin Syamsudin, DR., SP.S (K)Document37 pagesBy Thamrin Syamsudin, DR., SP.S (K)Lidwina ChandraNo ratings yet
- Asuhan Keperawatan Klien Dengan Stroke: Thrombosis Biasanya Terjadi Pada Orang Tua Yang SedangDocument11 pagesAsuhan Keperawatan Klien Dengan Stroke: Thrombosis Biasanya Terjadi Pada Orang Tua Yang SedangVirchanisa SahraNo ratings yet
- Burn and Electrical InjuryDocument29 pagesBurn and Electrical InjuryDr_minskyNo ratings yet
- Neuropa To Log IDocument99 pagesNeuropa To Log IRidhowan SyarkawiNo ratings yet
- Stroke Igd 02 17Document77 pagesStroke Igd 02 17Yoan Caroline Saron KapressyNo ratings yet
- Pediatric StrokeDocument90 pagesPediatric StrokeJanaki SethuramanNo ratings yet
- Patogenesa Pnykt Jantung Rematik, Gagal Jantung, Cor Pulmonal, Endocarditis BakterialisDocument35 pagesPatogenesa Pnykt Jantung Rematik, Gagal Jantung, Cor Pulmonal, Endocarditis BakterialisFirdha YusraNo ratings yet
- By Thamrin Syamsudin, DR., SP.S (K)Document37 pagesBy Thamrin Syamsudin, DR., SP.S (K)Kevin KarimNo ratings yet
- Konsulta Key ProcessDocument9 pagesKonsulta Key ProcessArlo Winston De GuzmanNo ratings yet
- Pharmacy 101Document48 pagesPharmacy 101api-381827675No ratings yet
- Pedia Reporting 2ND Yr 2ND SemDocument109 pagesPedia Reporting 2ND Yr 2ND SemWenalyn Grace Abella LlavanNo ratings yet
- Types of Wounds 101Document17 pagesTypes of Wounds 101Grey Tapes100% (1)
- NCP FinalDocument3 pagesNCP FinalCheska Mae PalicNo ratings yet
- Pengelolaan Asma Dengan Menerapkan Pelangi Asma APE: Manfaat Mandiri DANDocument10 pagesPengelolaan Asma Dengan Menerapkan Pelangi Asma APE: Manfaat Mandiri DANDrBamz WahyuNo ratings yet
- A Case of Molluscum ContagiosumDocument5 pagesA Case of Molluscum ContagiosumHomoeopathic PulseNo ratings yet
- Crash Cart ManagementDocument20 pagesCrash Cart ManagementRohannah D. MalawadNo ratings yet
- WHO 2019 NCoV Therapeutics 2022.2 EngDocument109 pagesWHO 2019 NCoV Therapeutics 2022.2 EngArina Papita SimanungkalitNo ratings yet
- Republic of The Philippines University Town, Northern SamarDocument14 pagesRepublic of The Philippines University Town, Northern SamarMark Johnson San JuanNo ratings yet
- TinglingDocument7 pagesTinglingMutia AnggraeniNo ratings yet
- Ginkgo Biloba Extract 40 MG Tablet - Taj Pharma Leaflet Patient Medication InformationDocument2 pagesGinkgo Biloba Extract 40 MG Tablet - Taj Pharma Leaflet Patient Medication InformationTAJ PHARMA — A Health Care ProviderNo ratings yet
- PulpotecDocument2 pagesPulpotecFeras Al-ZbounNo ratings yet
- Resume RDH PDFDocument2 pagesResume RDH PDFapi-668181352No ratings yet
- Restorative Quick Guide: All-On-4® Treatment ConceptDocument17 pagesRestorative Quick Guide: All-On-4® Treatment ConceptStanislav StrîșcaNo ratings yet
- Gastrointestinal Diseases: Psycho-Social Aspects: BackgroundDocument7 pagesGastrointestinal Diseases: Psycho-Social Aspects: BackgroundPedro LosadaNo ratings yet
- Chiba 2018Document9 pagesChiba 2018Fred MeyerNo ratings yet
- Answ1 PDFDocument184 pagesAnsw1 PDFAbdirahiim Ahmed100% (1)
- Painful Penile Induration and HomoeopathyDocument12 pagesPainful Penile Induration and HomoeopathyDr. Rajneesh Kumar Sharma MD HomNo ratings yet
- Breastfeeding and The Fascial System.Document3 pagesBreastfeeding and The Fascial System.jenniferspak100% (2)
- Clinical Problem Solving in Periodontology and ImplantologyDocument195 pagesClinical Problem Solving in Periodontology and ImplantologyEshan Verma100% (19)
- Phage TherapyDocument6 pagesPhage Therapyapi-535086280No ratings yet
- CH-2 Components of Food PPT-3Document27 pagesCH-2 Components of Food PPT-3SUHANEERIYANo ratings yet
- Planned Parenthood Advocates of OhioDocument2 pagesPlanned Parenthood Advocates of OhioAlanna JeanNo ratings yet
- Artikel Penelitian Kelengkapan Kuantitatif DRM RI Demam Thypoid 2022 - SUYANTIDocument10 pagesArtikel Penelitian Kelengkapan Kuantitatif DRM RI Demam Thypoid 2022 - SUYANTIgveuytNo ratings yet
- Felix Bronner Nutritional and Clinical Management of Chronic Conditions and Diseases PDFDocument299 pagesFelix Bronner Nutritional and Clinical Management of Chronic Conditions and Diseases PDFTux GilNo ratings yet
- Discussion Report Form 2 - Group C - PBL 1Document3 pagesDiscussion Report Form 2 - Group C - PBL 1Irma NareswariNo ratings yet
- MTP Act, FinalDocument29 pagesMTP Act, FinalDivya Sridharan100% (8)
- Speak Up For Patient Safety.1Document1 pageSpeak Up For Patient Safety.1Quality PmnhNo ratings yet