Download as pdf or txt
You might also like
- Nursing Care Plan For HypoglycemiaDocument3 pagesNursing Care Plan For HypoglycemiaCyrus De Asis83% (53)
- Nursing Care PlanDocument9 pagesNursing Care PlanLura Xstilice B. Galinato100% (1)
- Fibrogen, AstraZeneca, Astellas, and The Missing Pyrenees Data.Document15 pagesFibrogen, AstraZeneca, Astellas, and The Missing Pyrenees Data.buyersstrikewpNo ratings yet
- Phosphate Homeostasis, Assessment & Disorders: Royal Liverpool & Broadgreen University Hospital TrustDocument30 pagesPhosphate Homeostasis, Assessment & Disorders: Royal Liverpool & Broadgreen University Hospital Trustmonday125100% (1)
- Aaaq2 2015 Ir PresentationDocument45 pagesAaaq2 2015 Ir PresentationguerrezNo ratings yet
- 2012 Illinois Rules of The Road Review Course WorkbookDocument36 pages2012 Illinois Rules of The Road Review Course WorkbookmudkipzzzNo ratings yet
- Epp5 Fall 2020 The Practice of Pharmacy in Florida - Laws Rules - Alvarez Student Version 3 SlidesDocument25 pagesEpp5 Fall 2020 The Practice of Pharmacy in Florida - Laws Rules - Alvarez Student Version 3 Slidesapi-552486649No ratings yet
- OnQ Broadcast Intercom System ManualDocument2 pagesOnQ Broadcast Intercom System ManualJohn PallissardNo ratings yet
- The Duke Heart Failure ProgramDocument10 pagesThe Duke Heart Failure ProgramAnonymous PbAQxgw0No ratings yet
- Review: Marcel H A Muskiet, David C Wheeler, Hiddo J L HeerspinkDocument16 pagesReview: Marcel H A Muskiet, David C Wheeler, Hiddo J L Heerspinkellya theresia100% (1)
- World Preview 2016 Outlook To 2022Document49 pagesWorld Preview 2016 Outlook To 2022Willy Pérez-Barreto MaturanaNo ratings yet
- Kathrine O Neal PP PDFDocument92 pagesKathrine O Neal PP PDFrezqNo ratings yet
- Cardiovascular Outcomes Trials in Type 2 DiabetesDocument51 pagesCardiovascular Outcomes Trials in Type 2 Diabetes와라송이100% (1)
- 2002 GAO PDMP StudyDocument27 pages2002 GAO PDMP StudyKOMU NewsNo ratings yet
- Beyond Use DateDocument56 pagesBeyond Use DateDa Chan100% (1)
- 1183 - The Global Burden of Heart Failure. - Martin COWIE (London, United Kingdom)Document21 pages1183 - The Global Burden of Heart Failure. - Martin COWIE (London, United Kingdom)Mulyani EdwarNo ratings yet
- Pharmacy PresentationDocument93 pagesPharmacy PresentationAira Abella100% (1)
- InvokanaDocument14 pagesInvokanaalvaroNo ratings yet
- Canagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy CREDENCE TrialDocument29 pagesCanagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy CREDENCE Trialgokulam0075028No ratings yet
- 1117 FullDocument29 pages1117 FullElizabeth IB100% (1)
- AIIMS June 2020 DR Siraj Ahmad PDFDocument4 pagesAIIMS June 2020 DR Siraj Ahmad PDFadiNo ratings yet
- A Randomized, Double-Blind, Controlled Trial Comparing Rifaximin Plus Lactulose With Lactulose Alone in Treatment of Overt Hepatic EncephalopathyDocument3 pagesA Randomized, Double-Blind, Controlled Trial Comparing Rifaximin Plus Lactulose With Lactulose Alone in Treatment of Overt Hepatic EncephalopathyYunita DNo ratings yet
- SGLT 2 InhibitorDocument5 pagesSGLT 2 InhibitorAlimWijayaNo ratings yet
- THURSDAY Salisbury AfsharDocument39 pagesTHURSDAY Salisbury AfsharNational Press Foundation100% (1)
- Slides Outcomes of Sglt2i in Diabetic Kidney Disease Is It All DiabetesDocument29 pagesSlides Outcomes of Sglt2i in Diabetic Kidney Disease Is It All DiabetesVaibhav DafaleNo ratings yet
- Dapa Brief Data (14271)Document24 pagesDapa Brief Data (14271)Adel SALLAM100% (1)
- Controlled Substances LawsDocument8 pagesControlled Substances LawsJames Lindon100% (1)
- Aon Profile 2020Document16 pagesAon Profile 2020phanapa100% (1)
- Ultimate Reference DocumentDocument29 pagesUltimate Reference DocumentShellyza Moledina SajwaniNo ratings yet
- SGLT 2 Inhibitors: Newer Paradigms in The Treatment of Heart Failure With Reduced Ejection FractionDocument4 pagesSGLT 2 Inhibitors: Newer Paradigms in The Treatment of Heart Failure With Reduced Ejection FractionIJAR JOURNALNo ratings yet
- 11-24 First Draft 1 5Document3 pages11-24 First Draft 1 5api-242283963No ratings yet
- Euler MathematicsDocument36 pagesEuler MathematicsJohn HamiltonNo ratings yet
- Vanco & Ag PK 2018Document35 pagesVanco & Ag PK 2018Nguyen GeenNo ratings yet
- Johnson & Johnson: "Caring For You From The Beginning, To The Very End!"Document18 pagesJohnson & Johnson: "Caring For You From The Beginning, To The Very End!"Kaushik BalachandarNo ratings yet
- AnxolamDocument38 pagesAnxolammanjitdeshmukh2No ratings yet
- ACC Handbook Ascvd Type 2 Diabetes: On andDocument10 pagesACC Handbook Ascvd Type 2 Diabetes: On andZH. omg sarNo ratings yet
- Atherosclerosis, Dyslipidaemia and Diabetes SlidesDocument83 pagesAtherosclerosis, Dyslipidaemia and Diabetes SlidesWee DaliNo ratings yet
- Blue Bio V DoH and HFMADocument21 pagesBlue Bio V DoH and HFMAShane StarlingNo ratings yet
- Hypertension Treatment Steps For HypertensionDocument15 pagesHypertension Treatment Steps For Hypertensionfreelancer08100% (1)
- Hypertension MedicationsDocument7 pagesHypertension Medicationspinkels2u49No ratings yet
- Code of MarketingDocument160 pagesCode of MarketingShimul HalderNo ratings yet
- Challenges in Hypertension ManagementDocument86 pagesChallenges in Hypertension ManagementAdel SALLAMNo ratings yet
- Pharmacy 101Document48 pagesPharmacy 101api-381827675No ratings yet
- A Speech On PunctualityDocument2 pagesA Speech On PunctualityRrhayshelle Ahnne0% (1)
- CPG - Pneumonia (2010 Update)Document55 pagesCPG - Pneumonia (2010 Update)Jade Kenneth Gonzales LomansocNo ratings yet
- 15-Aspects of Pharma Business ModelDocument11 pages15-Aspects of Pharma Business Modelits4krishna3776No ratings yet
- SGLT2i Beyond Glycemic ControlDocument55 pagesSGLT2i Beyond Glycemic ControlSwapnaNo ratings yet
- PhaaaaDocument101 pagesPhaaaaWesam MazenNo ratings yet
- Diamicron MR Factsheet - FINALDocument5 pagesDiamicron MR Factsheet - FINALRoxana Potur100% (1)
- Pharmacy: Undergraduate Study 2016Document18 pagesPharmacy: Undergraduate Study 2016kgiyerNo ratings yet
- Introduction To Evidence-Based MedicineDocument28 pagesIntroduction To Evidence-Based Medicinedila2706No ratings yet
- Illinois Pilot Program Act RoadmapDocument19 pagesIllinois Pilot Program Act RoadmapMPPNo ratings yet
- RoxadustatDocument25 pagesRoxadustatjohnlau90No ratings yet
- Dha Pharmacist Examination Questions 9 JULY 2021Document6 pagesDha Pharmacist Examination Questions 9 JULY 2021Naveen KarankaraNo ratings yet
- New Concept of Pharmacy PracticeDocument21 pagesNew Concept of Pharmacy PracticeSaddamix AL OmariNo ratings yet
- Phosphorus Handout Word SearchDocument2 pagesPhosphorus Handout Word Searchapi-239733253No ratings yet
- Pharmacotherapy of DMDocument23 pagesPharmacotherapy of DMsalinaNo ratings yet
- Overview of ForxigaDocument37 pagesOverview of ForxigaoctatransferNo ratings yet
- Q3 Action Plan DR ZubairDocument10 pagesQ3 Action Plan DR ZubairShahid ShoaibNo ratings yet
- Antifertility DrugsDocument12 pagesAntifertility DrugsforplancessNo ratings yet
- SPIRIVA HandiHaler InstructionsDocument9 pagesSPIRIVA HandiHaler InstructionssamyvnNo ratings yet
- IKD9 - Radiological Evaluation of Renal CystsDocument26 pagesIKD9 - Radiological Evaluation of Renal CystsRenal Association MauritiusNo ratings yet
- IKD8 - HRCT Lung Findings in Pulmonary Renal SyndromesDocument46 pagesIKD8 - HRCT Lung Findings in Pulmonary Renal SyndromesRenal Association MauritiusNo ratings yet
- IDK4 - Bone Imaging in Systemic DiseaseDocument69 pagesIDK4 - Bone Imaging in Systemic DiseaseRenal Association MauritiusNo ratings yet
- The ABC of HBP - The Drug CabinetDocument16 pagesThe ABC of HBP - The Drug CabinetRenal Association MauritiusNo ratings yet
- IKD5 - Interventional Uro-Radiology - Current Practices and Aspirations in MauritiusDocument81 pagesIKD5 - Interventional Uro-Radiology - Current Practices and Aspirations in MauritiusRenal Association MauritiusNo ratings yet
- IKD6 - Contrast Associated AKIDocument44 pagesIKD6 - Contrast Associated AKIRenal Association MauritiusNo ratings yet
- IKD 2 - Imaging Renal InfectionDocument49 pagesIKD 2 - Imaging Renal InfectionRenal Association MauritiusNo ratings yet
- The ABC of HBP - When To Ring The AlarmDocument27 pagesThe ABC of HBP - When To Ring The AlarmRenal Association MauritiusNo ratings yet
- IKD3 - Uraemic Leontiassis OsseaDocument41 pagesIKD3 - Uraemic Leontiassis OsseaRenal Association MauritiusNo ratings yet
- Nephro Meets OncoDocument90 pagesNephro Meets OncoRenal Association MauritiusNo ratings yet
- The ABC of HBP-The Art of Blood Pressure TakingDocument44 pagesThe ABC of HBP-The Art of Blood Pressure TakingRenal Association MauritiusNo ratings yet
- The ABC of HBP - Living Well With HypertensionDocument70 pagesThe ABC of HBP - Living Well With HypertensionRenal Association MauritiusNo ratings yet
- The ABC of HBP-Evaluating HypertensionDocument56 pagesThe ABC of HBP-Evaluating HypertensionRenal Association MauritiusNo ratings yet
- CKD Talk To Medical Update GroupDocument49 pagesCKD Talk To Medical Update GroupRenal Association MauritiusNo ratings yet
- KDIGO GN GL Public Review Draft 1 June 2020 Lupus NephritisDocument40 pagesKDIGO GN GL Public Review Draft 1 June 2020 Lupus NephritisRenal Association MauritiusNo ratings yet
- Modern Management of Urinary Tract StonesDocument50 pagesModern Management of Urinary Tract StonesRenal Association MauritiusNo ratings yet
- Giving CREDENCE To The SGLT2 InhibitorsDocument117 pagesGiving CREDENCE To The SGLT2 InhibitorsRenal Association Mauritius100% (1)
- Living Donor Kidney Transplantation - Jonathon Oldsburgh - UOM 21.8.19Document106 pagesLiving Donor Kidney Transplantation - Jonathon Oldsburgh - UOM 21.8.19Renal Association MauritiusNo ratings yet
- Protocol For The Safe Use of Insulin v2 0 January 2016Document13 pagesProtocol For The Safe Use of Insulin v2 0 January 2016Dk YadavNo ratings yet
- Physioex Lab Report: Pre-Lab Quiz ResultsDocument4 pagesPhysioex Lab Report: Pre-Lab Quiz ResultsNovanza RayhanNo ratings yet
- Prof Dennis Yue Kellion LectureDocument55 pagesProf Dennis Yue Kellion LectureOhoud ElsheikhNo ratings yet
- Discharge Planning Project FinalDocument5 pagesDischarge Planning Project Finalapi-378401973No ratings yet
- Case ReportDocument10 pagesCase ReportFika Wilda AnggraeniNo ratings yet
- Classification of Diabetes Disease Using Decision Tree Algorithm (C4.5)Document9 pagesClassification of Diabetes Disease Using Decision Tree Algorithm (C4.5)Hariman BahtiarNo ratings yet
- Special Course: Team-Based Learning: Today's Clinical Case 1: Type I Diabetes MellitusDocument3 pagesSpecial Course: Team-Based Learning: Today's Clinical Case 1: Type I Diabetes MellitusAnanda DitaNo ratings yet
- JBDS 02 Nursing Management For DKA v1 20122022Document10 pagesJBDS 02 Nursing Management For DKA v1 20122022olazbt2000No ratings yet
- Diabetic Kidney DiseaseDocument69 pagesDiabetic Kidney DiseaseLavina JainNo ratings yet
- Prevalence of Refractive Errors in Type 2 Diabetic Patients in Northern IndiaDocument8 pagesPrevalence of Refractive Errors in Type 2 Diabetic Patients in Northern IndiaRagni MishraNo ratings yet
- ICD 10 CM Coding - DiabetesDocument68 pagesICD 10 CM Coding - Diabeteschaitanya varmaNo ratings yet
- Blood Glucose RegulationDocument10 pagesBlood Glucose RegulationJuma SammyNo ratings yet
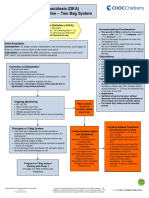
- Diabetic Ketoacidosis Care GuidelineDocument5 pagesDiabetic Ketoacidosis Care GuidelineRahma DhNo ratings yet
- Sick Day Advice For Adults With Type 1 DiabetesDocument3 pagesSick Day Advice For Adults With Type 1 DiabetesRegina PunNo ratings yet
- English Yt Sem 1 FinalDocument8 pagesEnglish Yt Sem 1 FinalGaming with DevilNo ratings yet
- Disclosure: Complex Case: Complications After Cardiac Surgery - Glucose, Sedation and ThrombocytopeniaDocument27 pagesDisclosure: Complex Case: Complications After Cardiac Surgery - Glucose, Sedation and ThrombocytopeniaEnrique SánchezNo ratings yet
- KDIGO 2022 Clinical Practice Guideline For Diabetes Management in CKDDocument128 pagesKDIGO 2022 Clinical Practice Guideline For Diabetes Management in CKDChelsy VitugNo ratings yet
- Fitness and Health - Body Mass Index and Waist ManagementDocument17 pagesFitness and Health - Body Mass Index and Waist ManagementEinej JenieNo ratings yet
- Jardiance Epar Product Information - enDocument47 pagesJardiance Epar Product Information - enSaad MasoodNo ratings yet
- Scenario Based QuestionsDocument7 pagesScenario Based QuestionsPraty SawadenNo ratings yet
- 2 MergedDocument11 pages2 MergedMudasir ElahiNo ratings yet
- Issue BriefDocument14 pagesIssue Briefapi-668173055No ratings yet
- Pharmacotherapyofdm-64854783c05c6 2Document105 pagesPharmacotherapyofdm-64854783c05c6 2zahra.sheardoostNo ratings yet
- Blue Index The Diabetes Health ScoreDocument33 pagesBlue Index The Diabetes Health ScoreDr DiabeatNo ratings yet
- A Comparative Study of Serum Ascorbate Between Newly Diagnosed Type 2 Diabetics and Long Standing Type 2 Diabetics On TreatmentDocument4 pagesA Comparative Study of Serum Ascorbate Between Newly Diagnosed Type 2 Diabetics and Long Standing Type 2 Diabetics On TreatmentIJAR JOURNALNo ratings yet
- NURS FPX 6011 Assessment 1 Evidence-Based Patient-Centered Concept MapDocument5 pagesNURS FPX 6011 Assessment 1 Evidence-Based Patient-Centered Concept Mapzadem5266No ratings yet
- NHS FPX 6004 Assessment 1 Dashboard Metrics EvaluationDocument6 pagesNHS FPX 6004 Assessment 1 Dashboard Metrics Evaluationfarwaamjad771No ratings yet
- CVD in Diabetes - EADSG 2016Document57 pagesCVD in Diabetes - EADSG 2016OmarNo ratings yet