Download as docx, pdf, or txt
You might also like
- Essentials of Abnormal Psychology 8th Edition Durand Test Bank DownloadDocument38 pagesEssentials of Abnormal Psychology 8th Edition Durand Test Bank DownloadcarrielivingstonocifrtkgnyNo ratings yet
- Fast Facts for Patients and Supporters: Cholangiocarcinoma: A cancer of the bile duct and liver Information + Taking Control = Best OutcomeFrom EverandFast Facts for Patients and Supporters: Cholangiocarcinoma: A cancer of the bile duct and liver Information + Taking Control = Best OutcomeNo ratings yet
- Epilepsy in African-RegionDocument56 pagesEpilepsy in African-RegionJaiye WeissNo ratings yet
- Weber 2015Document12 pagesWeber 2015Nikos SerifisNo ratings yet
- 10 1016@j CLD 2014 09 006Document23 pages10 1016@j CLD 2014 09 006Felix camilo GonzálezNo ratings yet
- Biliary Cystadenocarcinoma With Mesenchymal Stroma: A Case ReportDocument7 pagesBiliary Cystadenocarcinoma With Mesenchymal Stroma: A Case ReportAnalia RodriguezNo ratings yet
- Biliary Duct ImagingDocument7 pagesBiliary Duct ImagingImam FahriNo ratings yet
- Modern Imaging in Obstructive JaundiceDocument4 pagesModern Imaging in Obstructive JaundicedanaogreanuNo ratings yet
- Liver Fibrosis ProgressDocument9 pagesLiver Fibrosis ProgressTaufik Rizkian AsirNo ratings yet
- Hepato-Biliary System 26.4.2016Document59 pagesHepato-Biliary System 26.4.2016S B SayedNo ratings yet
- Case Report Klatskin TumorDocument5 pagesCase Report Klatskin TumorwadejackNo ratings yet
- Liver Disease: Schwartz Principles of Surgery2010Document50 pagesLiver Disease: Schwartz Principles of Surgery2010ralphNo ratings yet
- Aghiz 3Document12 pagesAghiz 3nandaaa aprilNo ratings yet
- L1 Radiology 2Document55 pagesL1 Radiology 2Princess FNo ratings yet
- American College of Radiology ACR Appropriateness CriteriaDocument10 pagesAmerican College of Radiology ACR Appropriateness CriteriaNovia ChrisnawatiNo ratings yet
- Autonomous VehiclesDocument11 pagesAutonomous VehiclessoortaNo ratings yet
- Diagnosticimagingof Hepaticlesionsinadults: Ramit Lamba,, Ghaneh Fananazapir,, Michael T. Corwin,, Vijay P. KhatriDocument32 pagesDiagnosticimagingof Hepaticlesionsinadults: Ramit Lamba,, Ghaneh Fananazapir,, Michael T. Corwin,, Vijay P. KhatrifranciscoreynaNo ratings yet
- Biliary Diseases: Dr. Wu Yang Dept. of Surgery The First Affiliated Hospital of Zhengzhou UniversityDocument75 pagesBiliary Diseases: Dr. Wu Yang Dept. of Surgery The First Affiliated Hospital of Zhengzhou Universityapi-19916399No ratings yet
- Hepatocellular Carcinoma - Diagnosis and TreatmentDocument46 pagesHepatocellular Carcinoma - Diagnosis and TreatmentSigh BalaNo ratings yet
- CholangiocarcinomaDocument9 pagesCholangiocarcinomaloloalpsheidiNo ratings yet
- Overview of The Evaluation of Hepatomegaly in Adults - UpToDateDocument19 pagesOverview of The Evaluation of Hepatomegaly in Adults - UpToDateAnna MoraNo ratings yet
- Biliary Diseases: Dr. Wu Yang Dept. of Surgery The First Affiliated Hospital of Zhengzhou UniversityDocument42 pagesBiliary Diseases: Dr. Wu Yang Dept. of Surgery The First Affiliated Hospital of Zhengzhou Universityapi-19916399No ratings yet
- CT Enterography ThesisDocument9 pagesCT Enterography Thesisrachelphillipsbillings100% (2)
- Multiple Hepatic Sclerosing HemangiomaDocument4 pagesMultiple Hepatic Sclerosing Hemangiomahussein_faourNo ratings yet
- Mrcs HepatobiliaryDocument40 pagesMrcs HepatobiliaryAdebisiNo ratings yet
- Mcevoy 2013Document17 pagesMcevoy 2013gcallupeNo ratings yet
- Cholangiocarcinoma: R.KarthikeyanDocument49 pagesCholangiocarcinoma: R.KarthikeyanKarthikeyan R100% (2)
- Imaging in Chronic PancreatitisDocument7 pagesImaging in Chronic Pancreatitisdesy 102017135No ratings yet
- Cholangiocarcinoma Differential DiagnosisDocument2 pagesCholangiocarcinoma Differential DiagnosisPremaKurniaNo ratings yet
- Wilm's Tumor RadiographyDocument8 pagesWilm's Tumor RadiographyWowo Masthuro MahfudNo ratings yet
- Cirrhosis Is A Late Stage of ScarringDocument2 pagesCirrhosis Is A Late Stage of ScarringLander EslaoNo ratings yet
- 2.4.1 Hepatobiliary and Pancreatic DisordersDocument17 pages2.4.1 Hepatobiliary and Pancreatic DisordersZayan SyedNo ratings yet
- Astrocytoma SDocument6 pagesAstrocytoma SMohammadAwitNo ratings yet
- Cholangiocarcinoma 2 Juni 2018Document40 pagesCholangiocarcinoma 2 Juni 2018Anonymous 1UgsHkUNo ratings yet
- Liver TumorsDocument52 pagesLiver TumorsRajendra DesaiNo ratings yet
- Benign Liver LesionsDocument30 pagesBenign Liver LesionstheintrovNo ratings yet
- PathophysiologyDocument3 pagesPathophysiologyHendro SNo ratings yet
- Obstructive Jaundice Aetiological SpectrDocument8 pagesObstructive Jaundice Aetiological Spectrvvwaghmare30No ratings yet
- Bendelow 2008Document8 pagesBendelow 2008Alexandra CastellanosNo ratings yet
- Choledocholithiasis: Evolving Standards For Diagnosis and ManagementDocument6 pagesCholedocholithiasis: Evolving Standards For Diagnosis and ManagementAngel Princëzza LovërzNo ratings yet
- Liver CancerDocument44 pagesLiver CancerJoyce Ann CumlatNo ratings yet
- An Updated Review of Cystic Hepatic LesionsDocument8 pagesAn Updated Review of Cystic Hepatic LesionsMayerlin CalvacheNo ratings yet
- Liver CancerDocument44 pagesLiver CancerEjay Jacob Ricamara50% (2)
- The Liver: Xu Bing, M.D. Associate ProfessorDocument71 pagesThe Liver: Xu Bing, M.D. Associate Professorapi-19916399No ratings yet
- 012011SCNA3Document14 pages012011SCNA3mariafmhNo ratings yet
- Secundary Deposits On LiverDocument7 pagesSecundary Deposits On LiverDarko DimitrievskiNo ratings yet
- Bile Duct DilatedDocument4 pagesBile Duct DilatedAmit GauravNo ratings yet
- Otto Van Delden and Robin SmithuisDocument11 pagesOtto Van Delden and Robin SmithuisSheila AnisaNo ratings yet
- Small Bowel Bleeding Aug2015Document23 pagesSmall Bowel Bleeding Aug2015dranita@yahoo.comNo ratings yet
- Exploración Del ColédocoDocument14 pagesExploración Del ColédocoJavier VegaNo ratings yet
- Liver 2024 LectureDocument5 pagesLiver 2024 LectureTaha MuhammedNo ratings yet
- Yu 2017Document3 pagesYu 2017Ish PanditNo ratings yet
- Isolated Hepatic SarcoidosisDocument6 pagesIsolated Hepatic Sarcoidosiskabal321No ratings yet
- Studiu Comparativ Al Factorilor Asociați Trombozei Venoase Portale La Pacienții Cirotici Cu Sau Fără HepatocarcinomDocument7 pagesStudiu Comparativ Al Factorilor Asociați Trombozei Venoase Portale La Pacienții Cirotici Cu Sau Fără HepatocarcinomAna BocaNo ratings yet
- General Guidelines For CT ProtocolsDocument4 pagesGeneral Guidelines For CT ProtocolsBilal Maqsood SukheraNo ratings yet
- Jasmin O. Dingle BSN-4y1-3CDocument6 pagesJasmin O. Dingle BSN-4y1-3CJasmn DingleNo ratings yet
- Hepatocellular Carcinoma 2009Document58 pagesHepatocellular Carcinoma 2009ctsakalakisNo ratings yet
- 17-09-2019 Lower GI FINALDocument32 pages17-09-2019 Lower GI FINALNaima HabibNo ratings yet
- Dynamic CT Findings of A Polypoid Gastric - ChrisnaDocument4 pagesDynamic CT Findings of A Polypoid Gastric - ChrisnaferonicaNo ratings yet
- Ha SsDocument7 pagesHa SsSowmya ChitraNo ratings yet
- Labs & Imaging for Primary Eye Care: Optometry In Full ScopeFrom EverandLabs & Imaging for Primary Eye Care: Optometry In Full ScopeNo ratings yet
- Malignant Liver Tumors: Current and Emerging TherapiesFrom EverandMalignant Liver Tumors: Current and Emerging TherapiesNo ratings yet
- Molluscum Contagiosum: Report of One Case With OverviewDocument3 pagesMolluscum Contagiosum: Report of One Case With Overviewevitri pasaribuNo ratings yet
- Nuts Are Not Good For HumansDocument88 pagesNuts Are Not Good For HumansNatalia67% (3)
- CBD DR Saugi IrfanDocument88 pagesCBD DR Saugi IrfanFebri BimayanaNo ratings yet
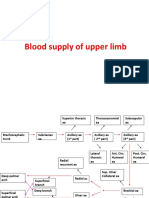
- Blood Supply of Upper LimbDocument36 pagesBlood Supply of Upper Limbteklay100% (2)
- 2 Vol. 8 Issue 5 May 2017 IJPSR RE 2098Document13 pages2 Vol. 8 Issue 5 May 2017 IJPSR RE 2098KhokonNo ratings yet
- PNLE Community Health Nursing Exam 4Document9 pagesPNLE Community Health Nursing Exam 4Denisse PalayNo ratings yet
- Family Nursing Care PlanDocument7 pagesFamily Nursing Care PlanMarilou Jumalon MontefalconNo ratings yet
- Lecture 1 - General Properties and Classification of FungiDocument4 pagesLecture 1 - General Properties and Classification of FungiRemelou Garchitorena AlfelorNo ratings yet
- NICE GuidelineDocument143 pagesNICE GuidelinewindyayudhiaNo ratings yet
- ACMG Classification of Sequence VariantsDocument4 pagesACMG Classification of Sequence VariantsDienatha Sekar BuanaNo ratings yet
- Eclampsia Guidelines FINAL Ratified MCYP SG Sept20 15Document20 pagesEclampsia Guidelines FINAL Ratified MCYP SG Sept20 15Grigore PopaNo ratings yet
- What Are The New Strains of Coronavirus?: We're Here For You With Information and Support Around CoronavirusDocument5 pagesWhat Are The New Strains of Coronavirus?: We're Here For You With Information and Support Around CoronavirusColeen gaboyNo ratings yet
- Dengue FeverDocument5 pagesDengue FeverMae AzoresNo ratings yet
- Unit 3 Genetics: Gene1:-Has Two Alleles P and PDocument38 pagesUnit 3 Genetics: Gene1:-Has Two Alleles P and Pkoket negashNo ratings yet
- Transport in AnimalsDocument43 pagesTransport in AnimalsEdwins MaranduNo ratings yet
- CV Prof. DR., Zairin Noor (English) - March 2019Document19 pagesCV Prof. DR., Zairin Noor (English) - March 2019Nina EvelynaNo ratings yet
- Claret College of Isabela: Senior High SchoolDocument5 pagesClaret College of Isabela: Senior High SchoolLatifah Emam0% (1)
- BloodlettingDocument5 pagesBloodlettingMaria Lana Grace DiazNo ratings yet
- M PostpartumDocument23 pagesM PostpartumDonaJeanNo ratings yet
- Daftar Puastaka BaruuuDocument2 pagesDaftar Puastaka BaruuuEvan AninditoNo ratings yet
- GASTRITISDocument11 pagesGASTRITISHemant SharmaNo ratings yet
- Lecture 5 Birth DefectsDocument13 pagesLecture 5 Birth DefectsDenis KaguiNo ratings yet
- Latihan Soal Literasi Bahasa Inggris 1Document9 pagesLatihan Soal Literasi Bahasa Inggris 1Daffa AryaputraNo ratings yet
- DHS CFS 600 Certificate of Child Examination Form IL444-4737Document2 pagesDHS CFS 600 Certificate of Child Examination Form IL444-4737ArtueroNo ratings yet
- Patient ZeroDocument109 pagesPatient ZeroDiego Emanuel Osechas LucartNo ratings yet
- Who HCV 2018Document108 pagesWho HCV 2018hendrawanNo ratings yet
- Gene Transfer MethodsDocument41 pagesGene Transfer MethodsMayuriGulhane100% (1)
- Tarun MeenaDocument59 pagesTarun Meenapiyushjakhar05No ratings yet