Download as docx, pdf, or txt
You might also like
- Cardiac Diagnostic TestsDocument14 pagesCardiac Diagnostic TestsSimran Josan100% (6)
- Endocarditis, Pericarditic, Myocarditis: TopicDocument104 pagesEndocarditis, Pericarditic, Myocarditis: TopicOM VERMANo ratings yet
- Medical EmergenciesDocument32 pagesMedical EmergenciesDharani Chowdary Kilari100% (1)
- Orlando's TheoryDocument52 pagesOrlando's TheorySimran Josan100% (1)
- Benign Prostatic Hyperplasia - BPH - Pathophysiology - Schematic DiagramDocument2 pagesBenign Prostatic Hyperplasia - BPH - Pathophysiology - Schematic DiagramSimran JosanNo ratings yet
- Dictionary of The Later New Testament & Its Developments (The IVP Bible Dictionary Series) 1997aDocument660 pagesDictionary of The Later New Testament & Its Developments (The IVP Bible Dictionary Series) 1997aHerbert Adam Storck85% (13)
- Right Heart Catheterization, NicvdDocument17 pagesRight Heart Catheterization, NicvdNavojit ChowdhuryNo ratings yet
- Cardiac TamponadeDocument29 pagesCardiac Tamponadeanimesh pandaNo ratings yet
- Joy B. Johnson Department of PharmacologyDocument55 pagesJoy B. Johnson Department of Pharmacologymatchees-gone rogueNo ratings yet
- Hypertensive Heart DiseaseDocument33 pagesHypertensive Heart Diseaserini_adriani6817No ratings yet
- Renal Transplant: 1) Steps Involved in Kidney TransplantationDocument4 pagesRenal Transplant: 1) Steps Involved in Kidney TransplantationNadia SalwaniNo ratings yet
- Mitral StenosisDocument50 pagesMitral Stenosissruthimeena6891No ratings yet
- Acute Isolated MyocarditisDocument20 pagesAcute Isolated Myocarditismerin sunilNo ratings yet
- Restrictive Lung DiseaseDocument32 pagesRestrictive Lung DiseaseSalman Khan100% (1)
- Left Ventricular Non-CompactionDocument20 pagesLeft Ventricular Non-CompactionlawlietNo ratings yet
- Appendix A: Doppler Ultrasound and Ankle-Brachial Pressure IndexDocument26 pagesAppendix A: Doppler Ultrasound and Ankle-Brachial Pressure IndexabigailNo ratings yet
- Ivc FilterDocument15 pagesIvc FilterashishNo ratings yet
- Rhythm Control Versus Rate Control in Atrial Fibrillation - UpToDocument39 pagesRhythm Control Versus Rate Control in Atrial Fibrillation - UpTohatsune100% (1)
- Primary Pulmonary TuberculosisDocument4 pagesPrimary Pulmonary TuberculosisdocdorkmeNo ratings yet
- Diabetes MellitusDocument79 pagesDiabetes Mellituskhalid saifur rahman khanNo ratings yet
- LESSON 9 Organ Donation ActDocument56 pagesLESSON 9 Organ Donation ActnullNo ratings yet
- 2019 - MCardiology - Clinical Features of Val HT 2019 2Document72 pages2019 - MCardiology - Clinical Features of Val HT 2019 2Vaenusha MuruganNo ratings yet
- Pulmonary HypertensionDocument58 pagesPulmonary HypertensionnadiasalimaNo ratings yet
- Blood Gas Analysis For Bedside DiagnosisDocument6 pagesBlood Gas Analysis For Bedside DiagnosisMuhamad Wirawan AdityoNo ratings yet
- Aortic Regurgitation CaseDocument38 pagesAortic Regurgitation CaseIka MagfirahNo ratings yet
- Infective EndocarditisDocument66 pagesInfective EndocarditisDias SeptariiaNo ratings yet
- Booklet Bcu Revisi 5Document8 pagesBooklet Bcu Revisi 5irza nasutionNo ratings yet
- Ozid Iv (Omeprazole) : Cedocard Iv (Isosorbid Dinitrat)Document15 pagesOzid Iv (Omeprazole) : Cedocard Iv (Isosorbid Dinitrat)Galih Aryo UtomoNo ratings yet
- Atrial Fibrillation: Discussed by - DR Kunwar Sidharth SaurabhDocument45 pagesAtrial Fibrillation: Discussed by - DR Kunwar Sidharth SaurabhKunwar Sidharth SaurabhNo ratings yet
- Arterial Stiffness-1Document21 pagesArterial Stiffness-1yoeldp100% (2)
- Cardiomyopathy: Imtiyaz Ali Lecturer, UTARDocument31 pagesCardiomyopathy: Imtiyaz Ali Lecturer, UTARSalman KhanNo ratings yet
- Esophageal Varices Week 4 T2T3Document37 pagesEsophageal Varices Week 4 T2T3liewhuilianNo ratings yet
- Coronary Artery DiseaseDocument33 pagesCoronary Artery DiseaseAlma Rifa'Ana LiskaNo ratings yet
- VasculitidesDocument13 pagesVasculitidesIrene Zae MwandotoNo ratings yet
- Mitral RegurgitationDocument11 pagesMitral RegurgitationAbdur RaqibNo ratings yet
- Approach To Septic ShockDocument16 pagesApproach To Septic ShockRaja EllysyaNo ratings yet
- Best Practices in PhlebotomyDocument8 pagesBest Practices in PhlebotomyPrincess WeiyoungNo ratings yet
- Aortic StenosisDocument3 pagesAortic StenosisMaxine BaraquiaNo ratings yet
- Sepsis Power Point Slide Presentation - The Guidelines - Implementation For The FutureDocument25 pagesSepsis Power Point Slide Presentation - The Guidelines - Implementation For The Futuremontie13No ratings yet
- Catheters and Guide Wires: Presenter: Omkar Gaonkar Course: M.SC., Mit 2 SEM Moderator: Kayalvizhi R DATE:26/03/2019Document42 pagesCatheters and Guide Wires: Presenter: Omkar Gaonkar Course: M.SC., Mit 2 SEM Moderator: Kayalvizhi R DATE:26/03/2019Omkar GaonkarNo ratings yet
- ArrhythmiaDocument25 pagesArrhythmiad_94No ratings yet
- 0105 GBukhman Hypertensive Heart DiseaseDocument27 pages0105 GBukhman Hypertensive Heart DiseaseEvi MiwaNo ratings yet
- Aorta DissectionDocument98 pagesAorta DissectionDian SukaryaNo ratings yet
- Ecg Pathology 02Document95 pagesEcg Pathology 02Andi MP Manurung100% (1)
- Overview of HIV and Its Management: Caroline Mills-Davies Emmanuel FantevieDocument101 pagesOverview of HIV and Its Management: Caroline Mills-Davies Emmanuel FantevieImanuel Fantevie100% (1)
- Start CPR Shout For Help/Activate Emergency Response: Give Oxygen Attach Monitor/DefibrillatorDocument2 pagesStart CPR Shout For Help/Activate Emergency Response: Give Oxygen Attach Monitor/DefibrillatorFelicia ErikaNo ratings yet
- Care of Patient With TPM Slide PresentationDocument16 pagesCare of Patient With TPM Slide PresentationirzehronNo ratings yet
- CKD MBD GuidelineDocument65 pagesCKD MBD GuidelinehoracioNo ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument33 pagesChronic Obstructive Pulmonary DiseasealexpharmNo ratings yet
- 10.08.07 Cardiac Tamponade HaagDocument16 pages10.08.07 Cardiac Tamponade HaagfoetorNo ratings yet
- 2012 Cath Lab Consensus DocumentDocument85 pages2012 Cath Lab Consensus DocumentDorin DocNo ratings yet
- Procedure For Patent Ductus Arteriosus (PDA) Device ClosureDocument13 pagesProcedure For Patent Ductus Arteriosus (PDA) Device ClosurejaganjaggiNo ratings yet
- Diagnosis & Treament: ShockDocument52 pagesDiagnosis & Treament: ShockasepNo ratings yet
- Cough, Dyspnea and HemoptysisDocument34 pagesCough, Dyspnea and HemoptysisPooja ShashidharanNo ratings yet
- Right Ventricular Myocardial InfarctionDocument43 pagesRight Ventricular Myocardial Infarctionrudresh m g0% (2)
- Normal Sinus RhythmDocument97 pagesNormal Sinus RhythmNatasha LiberisNo ratings yet
- Cardiac BiomarkersDocument72 pagesCardiac BiomarkersAmey JatharNo ratings yet
- NHS DIABETESUNDERGOING Surgery Adults Full PDFDocument72 pagesNHS DIABETESUNDERGOING Surgery Adults Full PDFekyNo ratings yet
- Lung Metabolism: Proteolysis and Antioproteolysis Biochemical Pharmacology Handling of Bioactive SubstancesFrom EverandLung Metabolism: Proteolysis and Antioproteolysis Biochemical Pharmacology Handling of Bioactive SubstancesAlain JunodNo ratings yet
- Community-Acquired Pneumonia: Strategies for ManagementFrom EverandCommunity-Acquired Pneumonia: Strategies for ManagementAntoni TorresRating: 4.5 out of 5 stars4.5/5 (2)
- Nursing Theory: Betty Neuman's: By: Harpreet Kaur M.Sc. 1 YearDocument34 pagesNursing Theory: Betty Neuman's: By: Harpreet Kaur M.Sc. 1 YearSimran JosanNo ratings yet
- Orem's Theory ApplicationDocument45 pagesOrem's Theory ApplicationSimran JosanNo ratings yet
- FEVERDocument8 pagesFEVERSimran JosanNo ratings yet
- Unit Plan: Unit TIME (HRS) Objective S Content Teaching Learning Activities A.V. Aids Assessment MethodsDocument2 pagesUnit Plan: Unit TIME (HRS) Objective S Content Teaching Learning Activities A.V. Aids Assessment MethodsSimran Josan67% (9)
- Course of Instruction Third Year B.Sc. Nursing Theory Sr. No. Subject Class Lab Practical Hrs. HrsDocument3 pagesCourse of Instruction Third Year B.Sc. Nursing Theory Sr. No. Subject Class Lab Practical Hrs. HrsSimran JosanNo ratings yet
- ENDOTRACHEAL INTUBATIOn SandeepDocument17 pagesENDOTRACHEAL INTUBATIOn SandeepSimran JosanNo ratings yet
- Cardiac Tamponade, Also Known As Pericardial Tamponade, Is AnDocument7 pagesCardiac Tamponade, Also Known As Pericardial Tamponade, Is AnSimran Josan100% (1)
- Orem'S Self-Care Deficit TheoryDocument52 pagesOrem'S Self-Care Deficit TheorySimran JosanNo ratings yet
- Arterial Blood Gas Analysis PROCEDUREDocument6 pagesArterial Blood Gas Analysis PROCEDURESimran Josan100% (4)
- Cyanotic Congenital Heart DiseaseDocument6 pagesCyanotic Congenital Heart DiseaseSimran JosanNo ratings yet
- Acynotic Heart DiseasesDocument13 pagesAcynotic Heart DiseasesSimran JosanNo ratings yet
- Anatomy and Physiology of Colon of Case StudyDocument4 pagesAnatomy and Physiology of Colon of Case StudySimran JosanNo ratings yet
- Unit Plan MSC 1 FRST Year - Docx 22Document5 pagesUnit Plan MSC 1 FRST Year - Docx 22Simran JosanNo ratings yet
- SUBMITTED TO - Resp. Mr. Somorjit SinghDocument8 pagesSUBMITTED TO - Resp. Mr. Somorjit SinghSimran JosanNo ratings yet
- LESSON PLAN ON CommunicationDocument11 pagesLESSON PLAN ON CommunicationSimran Josan100% (6)
- Disease Condition... Diabetes MellitusDocument6 pagesDisease Condition... Diabetes MellitusSimran JosanNo ratings yet
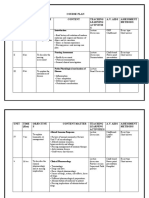
- Course Plan Unit Time (HRS) Objective S Content Teaching Learning Activitie S A.V. Aids Assessment MethodsDocument8 pagesCourse Plan Unit Time (HRS) Objective S Content Teaching Learning Activitie S A.V. Aids Assessment MethodsSimran JosanNo ratings yet
- Unit Plan UNI T Time (HRS) Objectives Content Teaching Learning Activities A.V. Aids Assessment MethodsDocument4 pagesUnit Plan UNI T Time (HRS) Objectives Content Teaching Learning Activities A.V. Aids Assessment MethodsSimran Josan100% (1)
- Complete FractureDocument10 pagesComplete FractureSimran JosanNo ratings yet
- ThesisDocument30 pagesThesisSimran JosanNo ratings yet
- Anatomy and Physiology of HeartDocument2 pagesAnatomy and Physiology of HeartSimran JosanNo ratings yet
- NCP of GlomerularnephritisDocument6 pagesNCP of GlomerularnephritisSimran JosanNo ratings yet
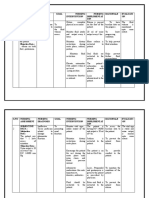
- S.N O Nursing Assessmen T Nursing Diagnosis Goal Nursing Intervention Nursing Implementati ON Rationale Evaluati ONDocument7 pagesS.N O Nursing Assessmen T Nursing Diagnosis Goal Nursing Intervention Nursing Implementati ON Rationale Evaluati ONSimran JosanNo ratings yet
- 1) Screening: Individual Achievement Test-Revised/Normative UpdateDocument5 pages1) Screening: Individual Achievement Test-Revised/Normative UpdateSimran JosanNo ratings yet
- S.N O Time Specific Objectives Content Matter Teaching Learning Activity AV Aids EvaluationDocument13 pagesS.N O Time Specific Objectives Content Matter Teaching Learning Activity AV Aids EvaluationSimran JosanNo ratings yet
- Animals in Disasters: The Four Phases of Emergency ManagementDocument20 pagesAnimals in Disasters: The Four Phases of Emergency ManagementSimran JosanNo ratings yet
- InfertilityDocument24 pagesInfertilitySimran JosanNo ratings yet
- Detailed Lesson Plan in Music 3Document7 pagesDetailed Lesson Plan in Music 3Aya NatsumeNo ratings yet
- GDNTDocument27 pagesGDNTrakshithmpNo ratings yet
- Effect of Lifestyle Modification Intervention On Health Status of Coronary Artery Disease Patients Randomized Control TrialDocument14 pagesEffect of Lifestyle Modification Intervention On Health Status of Coronary Artery Disease Patients Randomized Control TrialRobet Agung wicaksonoNo ratings yet
- TNCT Q3ExamDocument7 pagesTNCT Q3ExamREY ANN RUBIONo ratings yet
- Final Report - Foot Orthosis PDFDocument79 pagesFinal Report - Foot Orthosis PDFAdnan4466No ratings yet
- BGTOTSC1Document59 pagesBGTOTSC1hokshyNo ratings yet
- Make An Essay About The Problems of Student May e PDFDocument1 pageMake An Essay About The Problems of Student May e PDFTito villarasaNo ratings yet
- SNAP 2013 BulletinDocument85 pagesSNAP 2013 BulletinRohan SinghNo ratings yet
- 1 Intermolecular InteractionsDocument64 pages1 Intermolecular InteractionsAz Zahra Assyifa UshwahNo ratings yet
- Wa0008.Document2 pagesWa0008.innocentmakawa3No ratings yet
- Samruddhi RealtyDocument288 pagesSamruddhi Realtyjatt zaildarNo ratings yet
- Design of Steel Beams With Discrete Late PDFDocument9 pagesDesign of Steel Beams With Discrete Late PDFsathiyanNo ratings yet
- Science Syllabus Key Stage 2Document79 pagesScience Syllabus Key Stage 2Fathimath NajdhaNo ratings yet
- Analysis of MichelinDocument1 pageAnalysis of MichelinreganhinesNo ratings yet
- Understanding How To Buy A Computer RubricDocument1 pageUnderstanding How To Buy A Computer Rubricapi-370628488No ratings yet
- McLean Hospital 2013 Annual ReportDocument24 pagesMcLean Hospital 2013 Annual ReportmcleanhospitalNo ratings yet
- Brahma Satyam Jagan MithyaDocument2 pagesBrahma Satyam Jagan Mithya007RaaVaN Wu S PNo ratings yet
- A Methodology For Embedded Classificatio PDFDocument6 pagesA Methodology For Embedded Classificatio PDFHimon ThakurNo ratings yet
- GSTKDocument5 pagesGSTKCristobal Salinas PetersenNo ratings yet
- Vedantam Satyanarayana Sharma: by Subiksha S 18SDMB01Document11 pagesVedantam Satyanarayana Sharma: by Subiksha S 18SDMB01Subiksha SNo ratings yet
- January 1 - 7, 2020 Sports ReporterDocument8 pagesJanuary 1 - 7, 2020 Sports ReporterSportsReporterNo ratings yet
- 16-Political Economy of FilmDocument17 pages16-Political Economy of Filmhrishikesh arvikarNo ratings yet
- Erdogan Visits WashingtonDocument3 pagesErdogan Visits WashingtonPatrick SnellNo ratings yet
- Sec 5 Article Viii - White Light V ManilaDocument4 pagesSec 5 Article Viii - White Light V ManilaTon RiveraNo ratings yet
- Labour Law Notes GeneralDocument55 pagesLabour Law Notes GeneralPrince MwendwaNo ratings yet
- URBAN DESIGN A Deifinition, Approach and Conceptual FrameworkDocument37 pagesURBAN DESIGN A Deifinition, Approach and Conceptual FrameworkLalisa MNo ratings yet
- Cardinal Bernadin SEAMLESS GARMENTDocument5 pagesCardinal Bernadin SEAMLESS GARMENTMike LewisNo ratings yet
- Birth Day QuotesDocument2 pagesBirth Day QuotesNazmus SakibNo ratings yet
- 11 History Notes 04 Central Islamic LandsDocument9 pages11 History Notes 04 Central Islamic LandsPrisha NijhawanNo ratings yet