Download as pdf or txt
You might also like
- Fever Nursing Care PlanDocument3 pagesFever Nursing Care PlanMarie Anne T85% (40)
- Example Hospital Development PlanDocument6 pagesExample Hospital Development PlanMary Jean Gelito50% (2)
- Ibogaine Treatment Manual - by Howard Lotsof and Boaz WachtelDocument35 pagesIbogaine Treatment Manual - by Howard Lotsof and Boaz Wachtelboaz_wachtel100% (3)
- Nicotine Potentiates The Antidepressant Effects of Imipramine and Sertraline Sahar M. KamalDocument5 pagesNicotine Potentiates The Antidepressant Effects of Imipramine and Sertraline Sahar M. KamalAlexNo ratings yet
- Text-Ftgurem: Phy8iolDocument15 pagesText-Ftgurem: Phy8iolWAI SAM LIMNo ratings yet
- British Journal of Pharmacology and Chemotherapy - February 1965 - ASATOOR - The EXCRETION of DEXAMPHETAMINE and ITSDocument8 pagesBritish Journal of Pharmacology and Chemotherapy - February 1965 - ASATOOR - The EXCRETION of DEXAMPHETAMINE and ITSjumpyhumpyNo ratings yet
- J. Biol. Chem.-1954-Fukushima-863-74Document15 pagesJ. Biol. Chem.-1954-Fukushima-863-74Desak MothyNo ratings yet
- A Thiazolylami WDocument9 pagesA Thiazolylami Wwiam wiamNo ratings yet
- Toxicological Effects of Extracts of The Leaves of Scoparia Dulcis On The Brain ofDocument5 pagesToxicological Effects of Extracts of The Leaves of Scoparia Dulcis On The Brain ofFrancis AbuludeNo ratings yet
- The Excretion of Dexamphetamine and Its Derivatives j.1476-5381.1965.Tb02105.xDocument8 pagesThe Excretion of Dexamphetamine and Its Derivatives j.1476-5381.1965.Tb02105.xMichael PearsonNo ratings yet
- 1 s2.0 S0022227520390441 MainDocument4 pages1 s2.0 S0022227520390441 MainVanessa StepaniaNo ratings yet
- Vitaya Vira Suk 1999Document7 pagesVitaya Vira Suk 1999groot marvelNo ratings yet
- Bripharmchem00058 0003Document9 pagesBripharmchem00058 0003abdalah.han55No ratings yet
- Mechanism of Lithium Carbonate Induced HyperdipsiaDocument8 pagesMechanism of Lithium Carbonate Induced HyperdipsiaRafael CalpenaNo ratings yet
- Tyramine OxidaseDocument12 pagesTyramine OxidaseMilainy VianaNo ratings yet
- Anti-Hepatotoxic Activity of Clerodendrum Phlomidis: Phone No.-9415389171Document4 pagesAnti-Hepatotoxic Activity of Clerodendrum Phlomidis: Phone No.-9415389171Mirja AdiyaksaNo ratings yet
- CASE STUDY PEDIA - SaavedraDocument15 pagesCASE STUDY PEDIA - SaavedraChryst Louise SaavedraNo ratings yet
- Group (3) - Lab Report Fisvet 1 - P6 - Week 9Document20 pagesGroup (3) - Lab Report Fisvet 1 - P6 - Week 9NatAsyaNo ratings yet
- Effect of Prolonged Sedation With Propofol OnDocument4 pagesEffect of Prolonged Sedation With Propofol Onpetrus daveNo ratings yet
- InsulinDocument5 pagesInsulinEnni Mutiati Al-MaduryNo ratings yet
- Hotz 1971Document5 pagesHotz 1971CoNo ratings yet
- Activity 4 - Cell RespirationDocument6 pagesActivity 4 - Cell RespirationJaneNo ratings yet
- Polyvinyl AlcoholDocument18 pagesPolyvinyl AlcoholantiquekNo ratings yet
- 4 8 / 8 0 in TheDocument8 pages4 8 / 8 0 in ThelovehopeNo ratings yet
- Discussion.: All ProteinDocument7 pagesDiscussion.: All ProteinQadiir AlamNo ratings yet
- Anti-Fatigue Effects of Polyphenols Extracted From Pomegranate PeelDocument4 pagesAnti-Fatigue Effects of Polyphenols Extracted From Pomegranate PeelErlyta ViviNo ratings yet
- Intravenous Lipid Emulsion and Dexmedetomidine For Treatment of Feline Permethrin Intoxication: A Report From 4 CasesDocument9 pagesIntravenous Lipid Emulsion and Dexmedetomidine For Treatment of Feline Permethrin Intoxication: A Report From 4 CasescarlosNo ratings yet
- 62 KoneruDocument7 pages62 KonerubhutaniseNo ratings yet
- CO Inhalation at Dose Corresponding To Tobacco Smoke Worsens Cardiac Remodeling After Experimental Myocardial Infarction in RatsDocument7 pagesCO Inhalation at Dose Corresponding To Tobacco Smoke Worsens Cardiac Remodeling After Experimental Myocardial Infarction in RatsGael ROCHEFORTNo ratings yet
- Amitraz MetabolismDocument28 pagesAmitraz MetabolismDr. Attalla F. El-kottNo ratings yet
- Polyalkylcyanoacrylate Nanocapsules Increase The IntestinalDocument5 pagesPolyalkylcyanoacrylate Nanocapsules Increase The IntestinalLeonardo C.No ratings yet
- Galati2000 Effects of Teucrium Di6aricatum Heldr. Ssp. Di6aricatumDocument6 pagesGalati2000 Effects of Teucrium Di6aricatum Heldr. Ssp. Di6aricatumDjamila HEZILNo ratings yet
- Synthesis, Characterization and Evaluation For Antidepressant Activities of Some Novel 4-Thiazolidinone Derivatives B. Vamshi Dhar, Asish Bhaumik, P. Yadagiri ReddyDocument4 pagesSynthesis, Characterization and Evaluation For Antidepressant Activities of Some Novel 4-Thiazolidinone Derivatives B. Vamshi Dhar, Asish Bhaumik, P. Yadagiri ReddyHabibur RahmanNo ratings yet
- Intravenous Rocuronium 0,3 MG - KG Improves The Conditions For Tracheal Intubation in CatsDocument6 pagesIntravenous Rocuronium 0,3 MG - KG Improves The Conditions For Tracheal Intubation in CatsbrasilvilermandoNo ratings yet
- Ijgmp - Format-Studies On Effect of Control Drugs On Histology of Thyroid GlandDocument6 pagesIjgmp - Format-Studies On Effect of Control Drugs On Histology of Thyroid Glandiaset123No ratings yet
- Anti-Inflammatory and Analgesic Activity of Peperomia PellucidaDocument4 pagesAnti-Inflammatory and Analgesic Activity of Peperomia PellucidaJheaz Lhey RiemerNo ratings yet
- Destructive Effects of Prolonged Epilepticus: StatusDocument5 pagesDestructive Effects of Prolonged Epilepticus: StatusJaen VelazcoNo ratings yet
- 21 2011-JBAS Ketoprofen 2011Document6 pages21 2011-JBAS Ketoprofen 2011Dr. Taha NazirNo ratings yet
- Ketamine Promotes Alzheimers-Like NeurodegeneratiDocument6 pagesKetamine Promotes Alzheimers-Like Neurodegeneratiserama15692uacNo ratings yet
- Analgesic and Anti-Inflammatory Activities of (6) - Gingerol.Document5 pagesAnalgesic and Anti-Inflammatory Activities of (6) - Gingerol.TyaNo ratings yet
- Farmacocinesis de La KetaDocument10 pagesFarmacocinesis de La KetaEdwin GutiérrezNo ratings yet
- LORD-1989-Australian Veterinary JournalDocument2 pagesLORD-1989-Australian Veterinary JournalKelas C FKH UB 2018/2019No ratings yet
- Exercise 11-12Document5 pagesExercise 11-12Kenny TuanNo ratings yet
- Chronic Toxicity of Chenopodium Ambrosioides in Rats: Biomedical Research 2005 16 (2) : 111-113Document3 pagesChronic Toxicity of Chenopodium Ambrosioides in Rats: Biomedical Research 2005 16 (2) : 111-113Entang The'FirsterNo ratings yet
- The Effects of SKF 525-A On The Analgesic and Barbiturate-Potentiating Activity of A9-Tetrahydrocannabinol in M Ice and RatsDocument14 pagesThe Effects of SKF 525-A On The Analgesic and Barbiturate-Potentiating Activity of A9-Tetrahydrocannabinol in M Ice and RatsChristine AlayonNo ratings yet
- By Worth Hale: (From The Pharmacological Laboratory, University of Michigan)Document9 pagesBy Worth Hale: (From The Pharmacological Laboratory, University of Michigan)AlexNo ratings yet
- Acute and Subacute Toxicity of The Hydroalcoholic Extract From Wedelia Paludosa (Acmela Brasiliensis) (Asteraceae) in MiceDocument4 pagesAcute and Subacute Toxicity of The Hydroalcoholic Extract From Wedelia Paludosa (Acmela Brasiliensis) (Asteraceae) in MiceAsad SaleemNo ratings yet
- Case 1 Theophylline ToxicityDocument46 pagesCase 1 Theophylline ToxicityabechikNo ratings yet
- Effect of Administration Route of DDT On Acute Toxicity and On Drug Biotransformation in Various RodentsDocument16 pagesEffect of Administration Route of DDT On Acute Toxicity and On Drug Biotransformation in Various RodentsSh1vaNo ratings yet
- Hum. Reprod.-1996-Wyss-1992-7Document6 pagesHum. Reprod.-1996-Wyss-1992-7Juliana GuerraNo ratings yet
- EXERCISE XII Endocrine PhysiologyDocument4 pagesEXERCISE XII Endocrine PhysiologyKarl Sonny UganizaNo ratings yet
- Tutorial 2 - KGDocument4 pagesTutorial 2 - KGAbdurRahmanShafiNo ratings yet
- Isopropyl Alcohoi: 1) N-Octanol/Water Partition CoefficientDocument16 pagesIsopropyl Alcohoi: 1) N-Octanol/Water Partition CoefficientAdienk Abdul KNo ratings yet
- Rivea HypocrateriformisDocument3 pagesRivea HypocrateriformisugoNo ratings yet
- St. Paul University Philippines: MethodologyDocument8 pagesSt. Paul University Philippines: MethodologyAlicetair Buncad LopezNo ratings yet
- Pharmacological Studies of Cernilton Cernitin GBX and Cernitin T 60Document30 pagesPharmacological Studies of Cernilton Cernitin GBX and Cernitin T 60api-442513573No ratings yet
- 4 2009-4-JAP Dipyron 2009Document6 pages4 2009-4-JAP Dipyron 2009Dr. Taha NazirNo ratings yet
- Jurell 1981Document4 pagesJurell 1981Sam CastilloNo ratings yet
- Cardiovascular Respiratory: and Effects of Cannabis in Cat and RatDocument10 pagesCardiovascular Respiratory: and Effects of Cannabis in Cat and RatRóbson BatistaNo ratings yet
- Tumo Yoga Termodinamica 2013Document5 pagesTumo Yoga Termodinamica 2013Tarlley BarrosNo ratings yet
- Carica Papaya Linn. in Carbon Tetrachloride Induced RenalDocument9 pagesCarica Papaya Linn. in Carbon Tetrachloride Induced Renalsharadrai007No ratings yet
- O Level Biology Practice Questions And Answers HomeostasisFrom EverandO Level Biology Practice Questions And Answers HomeostasisRating: 5 out of 5 stars5/5 (1)
- The Total Synthesis of Natural ProductsFrom EverandThe Total Synthesis of Natural ProductsJohn ApSimonNo ratings yet
- A Case Study On CholelithiasisDocument51 pagesA Case Study On CholelithiasisANCHAL SHARMANo ratings yet
- OncologyDocument83 pagesOncologyANCHAL SHARMANo ratings yet
- Unit 2 PDFDocument36 pagesUnit 2 PDFANCHAL SHARMANo ratings yet
- Nursing Management: OF ArteriosclerosisDocument6 pagesNursing Management: OF ArteriosclerosisANCHAL SHARMANo ratings yet
- Section 1: General Pathology 1. Cellular Responses To Stress and Injury 3Document7 pagesSection 1: General Pathology 1. Cellular Responses To Stress and Injury 3ANCHAL SHARMANo ratings yet
- GNRH AssignmentDocument1 pageGNRH AssignmentANCHAL SHARMANo ratings yet
- Case Study of Acute GastritisDocument12 pagesCase Study of Acute GastritisANCHAL SHARMANo ratings yet
- Section 1 Pathology: Prelims - Indd 15 31-08-2015 14:44:44Document3 pagesSection 1 Pathology: Prelims - Indd 15 31-08-2015 14:44:44ANCHAL SHARMANo ratings yet
- National Doctor's DayDocument1 pageNational Doctor's DayANCHAL SHARMANo ratings yet
- Acute GastritisDocument43 pagesAcute GastritisANCHAL SHARMANo ratings yet
- SARSDocument17 pagesSARSANCHAL SHARMANo ratings yet
- Antiadrenergic System AssesmentDocument2 pagesAntiadrenergic System AssesmentANCHAL SHARMANo ratings yet
- GNRH AssignmentDocument1 pageGNRH AssignmentANCHAL SHARMANo ratings yet
- Adrenergic System Assesment: Dr. Mousumi Das Pharmacology DeptDocument2 pagesAdrenergic System Assesment: Dr. Mousumi Das Pharmacology DeptANCHAL SHARMANo ratings yet
- MeningitisDocument29 pagesMeningitisANCHAL SHARMANo ratings yet
- 2009 Flu Pandemic Influenza A (H1N1)Document8 pages2009 Flu Pandemic Influenza A (H1N1)ANCHAL SHARMANo ratings yet
- Gene TherapyDocument21 pagesGene TherapyDeepak Raj.kNo ratings yet
- Hypertensive EmergencyDocument17 pagesHypertensive EmergencyNhã PhạmNo ratings yet
- Experimental Design by Arun Kumar Mishra IftmDocument19 pagesExperimental Design by Arun Kumar Mishra IftmarunNo ratings yet
- Pharmacology of Thyroid Hormones and Anti Thyroid Drugs For Second Year Medicine StudentsDocument48 pagesPharmacology of Thyroid Hormones and Anti Thyroid Drugs For Second Year Medicine StudentsAmanuel MaruNo ratings yet
- RamiprilDocument1 pageRamiprilGracia Dela CruzNo ratings yet
- Paramedic Student GuideDocument431 pagesParamedic Student GuideShahed Facebook0% (1)
- Age Greater Than 60 Y/o Hereditary Precipitating Factors: Hypertension Increase Protein and Fat IntakeDocument3 pagesAge Greater Than 60 Y/o Hereditary Precipitating Factors: Hypertension Increase Protein and Fat Intakenursing concept mapsNo ratings yet
- WJGPTV 4 I 4Document57 pagesWJGPTV 4 I 4Sabrine DwigintNo ratings yet
- IM - Facts From Case Files CRCDocument80 pagesIM - Facts From Case Files CRCridin007No ratings yet
- Katalog Cook Gynekologie PDFDocument70 pagesKatalog Cook Gynekologie PDFHari_Shankar_G_7847No ratings yet
- Runner's Knee (Patellofemoral Pain) : CausesDocument4 pagesRunner's Knee (Patellofemoral Pain) : CausesBarath KannanNo ratings yet
- December 2012 Coffee Corner PaperDocument6 pagesDecember 2012 Coffee Corner Paperapi-123091552No ratings yet
- Management of Dry SocketDocument4 pagesManagement of Dry SocketFakhrul ImamNo ratings yet
- Traumatic Brain Injury A Case Report: SCORE:40/50Document10 pagesTraumatic Brain Injury A Case Report: SCORE:40/50Allan CastroNo ratings yet
- Obstruction EDocument10 pagesObstruction ECorina MunteanuNo ratings yet
- CipaDocument15 pagesCipaapi-247628136No ratings yet
- PETCT in Radiation Oncology - The FROG Manual For Clinical Use 2nd Edition - MIND - 4513173 - 2Document76 pagesPETCT in Radiation Oncology - The FROG Manual For Clinical Use 2nd Edition - MIND - 4513173 - 2Analía BardónNo ratings yet
- NAC Medications Chart 2016 A2Document1 pageNAC Medications Chart 2016 A2ayuniNo ratings yet
- Drugs Acting On GitDocument35 pagesDrugs Acting On GitPridho GaziansyahNo ratings yet
- 23rd EADPH Congress Joint With SESPO Authors Abstracts ListDocument3 pages23rd EADPH Congress Joint With SESPO Authors Abstracts ListAdminNo ratings yet
- DiabetesMellitus enDocument2 pagesDiabetesMellitus enRajesh KumarNo ratings yet
- 1345571825binder2Document36 pages1345571825binder2CoolerAdsNo ratings yet
- Unit 2 Final DraftDocument2 pagesUnit 2 Final Draftapi-252269185No ratings yet
- Vallabh Prakashan Order Form: C-5, SMA Cooperative Industrial Estate, GT Karnal RD, DELHI-33Document3 pagesVallabh Prakashan Order Form: C-5, SMA Cooperative Industrial Estate, GT Karnal RD, DELHI-33Naveen LankadasariNo ratings yet
- The Cure WithinDocument327 pagesThe Cure WithinAnonymous Ka4d6opeQt100% (1)
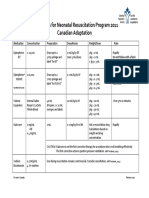
- Medications For Neonatal Resuscitation Program 2011 Canadian AdaptationDocument1 pageMedications For Neonatal Resuscitation Program 2011 Canadian AdaptationrubymayNo ratings yet
- Midterm Practice 2011Document53 pagesMidterm Practice 2011Marina ChengNo ratings yet