Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- JHA - Unloading of Sheet PileDocument3 pagesJHA - Unloading of Sheet PileJensen Sunga100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- TDSB GR 9-12 Student Census, 2022Document31 pagesTDSB GR 9-12 Student Census, 2022True NorthNo ratings yet
- Caregiver Resume Sample For ElderlyDocument6 pagesCaregiver Resume Sample For Elderlye76yzn9p100% (1)
- Stock GDL-CDMX 26-09-22Document3 pagesStock GDL-CDMX 26-09-22Ivan Domínguez LopezNo ratings yet
- Ipcr Final Mon July To December 2023Document2 pagesIpcr Final Mon July To December 2023Jhosie Melchor de GuzmanNo ratings yet
- Nutrition & Dietetics - A Healthy Career ChoiceDocument11 pagesNutrition & Dietetics - A Healthy Career ChoiceVivek Pai KNo ratings yet
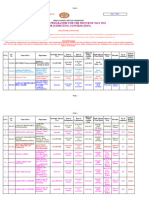
- Exam Programme May 2024 For ConfirmationDocument16 pagesExam Programme May 2024 For ConfirmationJim LevigsonNo ratings yet
- Dehp in PVC Medical FDADocument119 pagesDehp in PVC Medical FDAkalebasveggieNo ratings yet
- Intoksikasi - 15Document29 pagesIntoksikasi - 15Athifah Azalia AzarineNo ratings yet
- Group 5 - Module 10 - Processes and Methods Involved in CounselingDocument10 pagesGroup 5 - Module 10 - Processes and Methods Involved in CounselingLUCERO, ALEIAH KATE O.No ratings yet
- 2021-04-15 St. Mary's County TimesDocument40 pages2021-04-15 St. Mary's County TimesSouthern Maryland Online100% (1)
- Psychology Electives - 6th Semester PSY641A-EDocument10 pagesPsychology Electives - 6th Semester PSY641A-EALAKA RAJEEV 1930317No ratings yet
- Health 9 w7 q2 (Prevention of Substance Use and Abuse)Document31 pagesHealth 9 w7 q2 (Prevention of Substance Use and Abuse)John Paul SuelenNo ratings yet
- CHECKLIST - SwitchingDocument1 pageCHECKLIST - SwitchingAzminAgNo ratings yet
- 60-SGC-HSE-F-007 Task Risk Assesement - Rev00 (En+Az) - ApprovedDocument11 pages60-SGC-HSE-F-007 Task Risk Assesement - Rev00 (En+Az) - ApprovedРашад ИбрагимовNo ratings yet
- Getting Covid Benefit SoalDocument5 pagesGetting Covid Benefit Soalnanda nabilaNo ratings yet
- KumarDocument5 pagesKumarMeris JugadorNo ratings yet
- Stok Tanggal 25 Mei 2022Document8 pagesStok Tanggal 25 Mei 2022dewi lestariNo ratings yet
- Andhra University PHD Approved Topics in FinanceDocument6 pagesAndhra University PHD Approved Topics in FinanceNaga Sai KiranNo ratings yet
- Nigeria Gyts 2008Document39 pagesNigeria Gyts 2008aimanNo ratings yet
- Unit 3 Assignment TemplateDocument24 pagesUnit 3 Assignment TemplateMel DoodlesNo ratings yet
- Final Exam in Ed205 Advance PsychologyDocument2 pagesFinal Exam in Ed205 Advance PsychologyJeannitte Gelos OnanNo ratings yet
- Elise A Olsen Disorders of Hair GrowthDocument3 pagesElise A Olsen Disorders of Hair GrowthJames WarrenNo ratings yet
- Test Bank For Community Oral Health Practice For The Dental Hygienist 4th Edition Christine French BeattyDocument36 pagesTest Bank For Community Oral Health Practice For The Dental Hygienist 4th Edition Christine French Beattychiragramallfsk7100% (55)
- Large Databases in Anaesthesiology: ReviewDocument6 pagesLarge Databases in Anaesthesiology: ReviewSoumya DasNo ratings yet
- Impact of Lockdown Due To Coronavirus Pandemic On The Performance of Reliance Industries LTDDocument6 pagesImpact of Lockdown Due To Coronavirus Pandemic On The Performance of Reliance Industries LTDAishNo ratings yet
- Module in Physical Education 9 (First Quarter, WEEK 1) MelcDocument11 pagesModule in Physical Education 9 (First Quarter, WEEK 1) MelcElton Martin de LeonNo ratings yet
- 2nd Sem. Syllabus For P.E Grade 11Document4 pages2nd Sem. Syllabus For P.E Grade 11Bench Benito ColladoNo ratings yet
- Goshu Et Al Food Security in EthiopiaDocument12 pagesGoshu Et Al Food Security in EthiopiaibsaNo ratings yet
- Cancer Cells Can Exhibit A Sparing FLASH Effect atDocument9 pagesCancer Cells Can Exhibit A Sparing FLASH Effect atMohamed El-AgamyNo ratings yet