Download as doc, pdf, or txt
You might also like
- Ig2 Report Muhammad ArslanDocument18 pagesIg2 Report Muhammad ArslanShaheen Himalyn salt88% (8)
- JSA FOR HT LT Panel - Transformer InstallationDocument2 pagesJSA FOR HT LT Panel - Transformer Installationwahyu nugroho86% (7)
- Arts and Design - Q1 - Mod2 - ArtistryRelatedInjuries - Version1 by Romel SabidorDocument26 pagesArts and Design - Q1 - Mod2 - ArtistryRelatedInjuries - Version1 by Romel SabidorJayson Paul Dalisay Datinguinoo100% (2)
- Accident Report PDFDocument2 pagesAccident Report PDFAdriana LimaNo ratings yet
- NHCA Health Club Incident RPT FormDocument2 pagesNHCA Health Club Incident RPT Formcrossfitvelocity982No ratings yet
- Accident Investigation Form SampleDocument2 pagesAccident Investigation Form Sample811 - 813100% (2)
- 6) SWP-06 First AidDocument6 pages6) SWP-06 First AidRachel NoraNo ratings yet
- Incident Report FromDocument3 pagesIncident Report Fromannerie.krugerNo ratings yet
- Accident Report1Document5 pagesAccident Report1gopsareknoNo ratings yet
- Incident Investigation ReportDocument4 pagesIncident Investigation ReportZohaib TahirNo ratings yet
- Injury Incident Near Miss Report FormDocument3 pagesInjury Incident Near Miss Report FormB.A.R.SNo ratings yet
- Incident Investigation ReportDocument4 pagesIncident Investigation ReportZohaib TahirNo ratings yet
- Form Incident Investigation Report Form Tiybi9Document5 pagesForm Incident Investigation Report Form Tiybi9Godfrey TamaneNo ratings yet
- Appendix C (C) - Accident-or-Incident-RecordDocument2 pagesAppendix C (C) - Accident-or-Incident-Recordanoopanil16No ratings yet
- Injury Incident Report FormDocument3 pagesInjury Incident Report FormDave Joseph Conde100% (1)
- TEMPLATE - Incident Report FormDocument3 pagesTEMPLATE - Incident Report FormZia MalikNo ratings yet
- Incident Reporting Form Pages 1&2Document2 pagesIncident Reporting Form Pages 1&2Abraham MathewNo ratings yet
- TEMPLATE - Incident Report FormDocument3 pagesTEMPLATE - Incident Report FormbesongNo ratings yet
- Accident Report Form: Name of Employee AGE SEX Designation/TradeDocument2 pagesAccident Report Form: Name of Employee AGE SEX Designation/TradeArcon AlvarNo ratings yet
- Accident Incident Report Form - 0Document2 pagesAccident Incident Report Form - 0Francis Hans B. GauranoNo ratings yet
- Incident ReportDocument4 pagesIncident ReportSachi AnandNo ratings yet
- Notification of Occupational Accident and Dangerous OccurrenceDocument3 pagesNotification of Occupational Accident and Dangerous OccurrenceThevanath Gunasekaran100% (1)
- HSE-FR-02 Incident Investigation ReportDocument4 pagesHSE-FR-02 Incident Investigation ReportAdil AbdulkhaderNo ratings yet
- PCD-QSC-FMT-13 Accident-Incident Investigation ReportDocument2 pagesPCD-QSC-FMT-13 Accident-Incident Investigation ReportRami KhedroNo ratings yet
- Wehu-A1a2jkkp 6Document3 pagesWehu-A1a2jkkp 6Nursyafiq Ali ShibramulisiNo ratings yet
- Accident / Incident Report Form: Universal ConsultancyDocument2 pagesAccident / Incident Report Form: Universal ConsultancyPrakash PatelNo ratings yet
- Accident / Incident Report Form: Use Additional Pages And/or Photos If NecessaryDocument2 pagesAccident / Incident Report Form: Use Additional Pages And/or Photos If NecessaryAkshay JadhavNo ratings yet
- Worksheet in WEHUDocument22 pagesWorksheet in WEHUKeirel EdrinNo ratings yet
- Ehs-18-Incident Investigation ReportDocument2 pagesEhs-18-Incident Investigation ReportMark RusianaNo ratings yet
- GRA - Civil Work - WWT HousekeepingDocument17 pagesGRA - Civil Work - WWT HousekeepingMohamad Nazmi Mohamad RafianNo ratings yet
- Appendix 2 - Aldar Incident Investigation Report FormDocument7 pagesAppendix 2 - Aldar Incident Investigation Report FormXtreme-DesignsNo ratings yet
- Health, Safety and Environment Incident and Accident Investigation ReportDocument6 pagesHealth, Safety and Environment Incident and Accident Investigation ReportMuhammad FirdhausNo ratings yet
- Construction Accident Report FormDocument2 pagesConstruction Accident Report FormGirma AssefaNo ratings yet
- TraumaDocument4 pagesTraumaDra. Carol Angélica Artigas GómezNo ratings yet
- Incident Report Muhammad Zahid Steel FixerDocument4 pagesIncident Report Muhammad Zahid Steel Fixerarfa vainceNo ratings yet
- REG002 Workplace Hazard IdentificationDocument2 pagesREG002 Workplace Hazard IdentificationaceNo ratings yet
- HSE-F-NEOM-008 - Final Incident-Accident ReportDocument4 pagesHSE-F-NEOM-008 - Final Incident-Accident ReportAhmed MohamedNo ratings yet
- Accident Investigation ReportDocument6 pagesAccident Investigation ReportWaseem HussainNo ratings yet
- REG002 Workplace Hazard IdentificationDocument2 pagesREG002 Workplace Hazard IdentificationAceNo ratings yet
- Incident Report Muhammad SohailDocument4 pagesIncident Report Muhammad Sohailarfa vainceNo ratings yet
- NP-NEOM-OSH-Form 05 Incident Notification FormDocument2 pagesNP-NEOM-OSH-Form 05 Incident Notification FormyasirNo ratings yet
- F-OHS-15 Incident Accident Investigation ReportDocument7 pagesF-OHS-15 Incident Accident Investigation ReportvalveworkshseNo ratings yet
- Form G: Part A - Incident NotificationDocument7 pagesForm G: Part A - Incident NotificationFNo ratings yet
- Accident / Incident ReportDocument4 pagesAccident / Incident ReportDth InfraNo ratings yet
- Incident Reporting Form (Ir 01) : Fatality Lti I RWC Accident NEAR MissDocument1 pageIncident Reporting Form (Ir 01) : Fatality Lti I RWC Accident NEAR Missmuhammadumar412296No ratings yet
- Attach A - OHS StatisticsDocument13 pagesAttach A - OHS StatisticsWilfredo MinaNo ratings yet
- Employee's Report of Injury FormDocument4 pagesEmployee's Report of Injury FormAlifudin HanifNo ratings yet
- Accident Report Form: Safety, Health & EnvironmentDocument3 pagesAccident Report Form: Safety, Health & EnvironmentPio RodolfoNo ratings yet
- Medical Device Complaint FormDocument2 pagesMedical Device Complaint FormJEYA KUMARANNo ratings yet
- Accident Report FormDocument2 pagesAccident Report Formglenn umali100% (2)
- Incident Report: (Company Name, Phone / Fax)Document2 pagesIncident Report: (Company Name, Phone / Fax)Ali SalihNo ratings yet
- Forensic Interpretation of Injuries/wounds Found On The Human BodyDocument6 pagesForensic Interpretation of Injuries/wounds Found On The Human BodydosiNo ratings yet
- Toolbox TalkDocument3 pagesToolbox Talkshane.ramirez1980No ratings yet
- Appendix 7 - Contractor Incident Report Form 100910 YwDocument3 pagesAppendix 7 - Contractor Incident Report Form 100910 Ywjennifer tigtigNo ratings yet
- AFC-HSE-F04 - Detailed Accident Investigation ReportDocument3 pagesAFC-HSE-F04 - Detailed Accident Investigation ReportIbrahim MohamedNo ratings yet
- Hse - 02 Accident Incident ReportDocument3 pagesHse - 02 Accident Incident Reportgulshan.hse22No ratings yet
- SAFETY Accident - Investigation - Form (1) (AutoRecovered)Document6 pagesSAFETY Accident - Investigation - Form (1) (AutoRecovered)ramilnavarra62No ratings yet
- Lamp Sesi 8.2 Investigasi SCATDocument2 pagesLamp Sesi 8.2 Investigasi SCATaab kanayaNo ratings yet
- SHES - Prelim Inci NotificationDocument3 pagesSHES - Prelim Inci NotificationKoi ChiNo ratings yet
- 2 (Accident Incident Report)Document3 pages2 (Accident Incident Report)abb hseNo ratings yet
- Rapid Health Assessment (Mci) : Event TitleDocument2 pagesRapid Health Assessment (Mci) : Event TitleMrr ThoNo ratings yet
- Incident Report TemplateDocument3 pagesIncident Report Templateapi-412577219No ratings yet
- Leakpen Vonroll HydroDocument4 pagesLeakpen Vonroll HydroElvyn Fabellore HerreraNo ratings yet
- Log3000 Vonroll HydroDocument4 pagesLog3000 Vonroll HydroElvyn Fabellore HerreraNo ratings yet
- Premium Efficient Three Phase Baldor Farm Duty Motors 1 Thru 100 Horsepower NEMA 56 Thru 405TDocument2 pagesPremium Efficient Three Phase Baldor Farm Duty Motors 1 Thru 100 Horsepower NEMA 56 Thru 405TElvyn Fabellore HerreraNo ratings yet
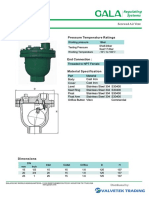
- Gala Air Vent Threaded To NPT CI Body 16 Bar Fig 9701Document1 pageGala Air Vent Threaded To NPT CI Body 16 Bar Fig 9701Elvyn Fabellore HerreraNo ratings yet
- lotoFINALDocument19 pageslotoFINALElvyn Fabellore HerreraNo ratings yet
- Woltman Type Flow MeterDocument4 pagesWoltman Type Flow MeterElvyn Fabellore HerreraNo ratings yet
- Construction Methodology Building OfficeDocument2 pagesConstruction Methodology Building OfficeElvyn Fabellore HerreraNo ratings yet
- 33 Raphael SAV BrochureDocument2 pages33 Raphael SAV BrochureElvyn Fabellore HerreraNo ratings yet
- Hazard Identification and Risk Assessment Criteria Form Hazard Identification and Risk Assessment Criteria FormDocument21 pagesHazard Identification and Risk Assessment Criteria Form Hazard Identification and Risk Assessment Criteria FormElvyn Fabellore HerreraNo ratings yet
- Boracay Island Water Company, IncDocument1 pageBoracay Island Water Company, IncElvyn Fabellore HerreraNo ratings yet
- Yapak CPRDocument1 pageYapak CPRElvyn Fabellore HerreraNo ratings yet
- Liloan Pumping Station Electro-Mech UpgradeDocument1 pageLiloan Pumping Station Electro-Mech UpgradeElvyn Fabellore HerreraNo ratings yet
- L I S T O F EquipementDocument1 pageL I S T O F EquipementElvyn Fabellore HerreraNo ratings yet
- Request To Release Check Policy Documents To Representative or Agent - 01132015 - 3rd Added PDFDocument1 pageRequest To Release Check Policy Documents To Representative or Agent - 01132015 - 3rd Added PDFElvyn Fabellore HerreraNo ratings yet
- A Method For Creating A Septic Tank Comprising: Erecting A Secondary Frame, Erecting ADocument2 pagesA Method For Creating A Septic Tank Comprising: Erecting A Secondary Frame, Erecting AElvyn Fabellore HerreraNo ratings yet
- Samuel L. Lozada Engr. Lawrence ConopioDocument1 pageSamuel L. Lozada Engr. Lawrence ConopioElvyn Fabellore HerreraNo ratings yet
- Scaffold Inspection Report1Document1 pageScaffold Inspection Report1Elvyn Fabellore HerreraNo ratings yet
- Smoking and Its EffectsDocument65 pagesSmoking and Its EffectsElvyn Fabellore HerreraNo ratings yet
- Manila Water Company, Inc. MWSS Compound, 489 Katipunan Road Old Balara, Quezon CityDocument2 pagesManila Water Company, Inc. MWSS Compound, 489 Katipunan Road Old Balara, Quezon CityElvyn Fabellore HerreraNo ratings yet
- Health, Safety and Environment Incident and Accident Investigation ReportDocument6 pagesHealth, Safety and Environment Incident and Accident Investigation ReportMuhammad FirdhausNo ratings yet
- Nursing Care Plan: Angeles University Foundation College of NursingDocument3 pagesNursing Care Plan: Angeles University Foundation College of NursingPatricia Ellyne DizonNo ratings yet
- ftc2 Ducting Risk Ass 2Document11 pagesftc2 Ducting Risk Ass 2Kyle AdamsNo ratings yet
- Ig2 Example 1 v1Document16 pagesIg2 Example 1 v1asim zeeshanNo ratings yet
- Medial Epicondyle Fracture of The Humerus - WikipediaDocument6 pagesMedial Epicondyle Fracture of The Humerus - Wikipediaismail ajiNo ratings yet
- Achilles Tendon InjuryDocument6 pagesAchilles Tendon InjuryKEVIN NGUYENNo ratings yet
- Freemasonry Today ISSUE 25Document84 pagesFreemasonry Today ISSUE 25MarianoRomeroNo ratings yet
- Comprehensive Medical Assisting Administrative and Clinical Competencies 6th Edition Lindh Test BankDocument14 pagesComprehensive Medical Assisting Administrative and Clinical Competencies 6th Edition Lindh Test Bankricinussquabash.46iz9100% (28)
- PE 12 4th QuarterDocument4 pagesPE 12 4th Quarterwiljhon sunioNo ratings yet
- Q4: What Management Failures Could Have Contributed To This Accident?Document2 pagesQ4: What Management Failures Could Have Contributed To This Accident?Mohamed saidNo ratings yet
- Scholastic Scope Magazine May 2017 - Nick VenturaDocument5 pagesScholastic Scope Magazine May 2017 - Nick VenturaPatty Rice100% (2)
- Is Your Workplace SafeDocument36 pagesIs Your Workplace SafeAmor ArnaoNo ratings yet
- Safety & Health Officer: Introductory Course GLRT0060 UTM Professional Skills CertificateDocument6 pagesSafety & Health Officer: Introductory Course GLRT0060 UTM Professional Skills CertificateHaikal Hamka100% (1)
- First Aid For Soldiers FM 21Document93 pagesFirst Aid For Soldiers FM 21ChannelGNo ratings yet
- Referência Bibliográfica Trauma CraniofacialDocument2 pagesReferência Bibliográfica Trauma CraniofacialSamira FreitasNo ratings yet
- Physical Educ & Health G11aDocument42 pagesPhysical Educ & Health G11aANGELU RANE BAGARES INTOLNo ratings yet
- Tort Law Psychiatric Illness: Ms GallopDocument23 pagesTort Law Psychiatric Illness: Ms GallopABDOULIENo ratings yet
- Physical Injuries: Rey J. Millena, MD, MCHM, FPCAM Legal MedicineDocument45 pagesPhysical Injuries: Rey J. Millena, MD, MCHM, FPCAM Legal MedicineSheena TNo ratings yet
- Emergency Pre-Drill Report WAHDocument5 pagesEmergency Pre-Drill Report WAHSakendran RamodaranNo ratings yet
- Safety Practices and Sports Injury Management.Document8 pagesSafety Practices and Sports Injury Management.cejaygecainNo ratings yet
- Blue Healer: Hazardous Incidents RegisterDocument1 pageBlue Healer: Hazardous Incidents RegisterParash RijalNo ratings yet
- Safety Committee Vs Incident InvestigationDocument74 pagesSafety Committee Vs Incident InvestigationSham AranNo ratings yet
- Assignment OSH Act Legal RegisterDocument18 pagesAssignment OSH Act Legal RegisterMOHD RASHIDI BIN AWANG JAMAN (BOMBA-WPLABUAN)No ratings yet
- Gano Massage Oil - English - Malaysia - v2Document13 pagesGano Massage Oil - English - Malaysia - v2bigjebatNo ratings yet
- Safety Policy PDFDocument16 pagesSafety Policy PDFaselabollegalaNo ratings yet
- Job Hazard Analysis (JHA) TrainingDocument76 pagesJob Hazard Analysis (JHA) Trainingyoakamura100% (1)