Download as pdf or txt
You might also like
- AP Medical Council Renewal ApplicationDocument2 pagesAP Medical Council Renewal Applicationdrvaas73% (11)
- Acute Respiratory Distress SyndromeDocument43 pagesAcute Respiratory Distress SyndromeAgnes Pritama Fahmi100% (1)
- Non-Invasive Positive Pressure Ventilation in Acute Respiratory Failure: Providing Competent CareDocument9 pagesNon-Invasive Positive Pressure Ventilation in Acute Respiratory Failure: Providing Competent CareAndana TrisaviNo ratings yet
- Average Volume-Assured Pressure Support - StatPearls - NCBI BookshelfDocument8 pagesAverage Volume-Assured Pressure Support - StatPearls - NCBI BookshelfmohammedNo ratings yet
- Accuracy of The Ventilator Automated Displayed Respiratory Mechanics in Passive and Active Breathing Conditions: A Bench StudyDocument7 pagesAccuracy of The Ventilator Automated Displayed Respiratory Mechanics in Passive and Active Breathing Conditions: A Bench StudyLejlaNo ratings yet
- Ventilación Del Pulmón Sano CC Current 20Document5 pagesVentilación Del Pulmón Sano CC Current 20Silvia Lorena Mireles GonzálezNo ratings yet
- Nippv CCDocument13 pagesNippv CCcnvNo ratings yet
- Acuterespiratorydistress Syndrome: Ventilator Management and Rescue TherapiesDocument16 pagesAcuterespiratorydistress Syndrome: Ventilator Management and Rescue TherapiessamuelNo ratings yet
- Windisch 2002Document8 pagesWindisch 2002guidepNo ratings yet
- Noninvasive Positive Pressure Ventilation - Successful Outcome in Patients With Acute Lung Injury ARDSDocument6 pagesNoninvasive Positive Pressure Ventilation - Successful Outcome in Patients With Acute Lung Injury ARDSpaulina mancilla ramirezNo ratings yet
- Airway Pressure Release Ventilation and PediatricsDocument12 pagesAirway Pressure Release Ventilation and PediatricsAndres Felipe BarreraNo ratings yet
- Noninvasive Ventilator Devices and ModesDocument11 pagesNoninvasive Ventilator Devices and ModesISABEL SOFIA CABARCAS COGOLLONo ratings yet
- Cpap Use in OSA 2005Document12 pagesCpap Use in OSA 2005Davi LopesNo ratings yet
- Effects of Lung Expansion Therapy On Lung Function in Patients With Prolonged Mechanical VentilationDocument7 pagesEffects of Lung Expansion Therapy On Lung Function in Patients With Prolonged Mechanical Ventilationcard breatheNo ratings yet
- Advances in Positive Airway Pressure Treatment Modalities For Hypoventilation SyndromesDocument11 pagesAdvances in Positive Airway Pressure Treatment Modalities For Hypoventilation Syndromessavvy_as_98-1No ratings yet
- WWW Minervamedica It@r02y2016n01a0058Document11 pagesWWW Minervamedica It@r02y2016n01a0058Gonzalo Venegas RojasNo ratings yet
- EXPRESS Trial 2008Document10 pagesEXPRESS Trial 2008Dr. Sergio Oscar AlunniNo ratings yet
- 2014 Keenan - Distres y ReclutamientoDocument6 pages2014 Keenan - Distres y Reclutamientolewita.valeriaNo ratings yet
- What Is APRVDocument3 pagesWhat Is APRVMario AlexanderNo ratings yet
- Novel Forms of Ventilation in Neonates Neurally Adjusted VentilatoryDocument16 pagesNovel Forms of Ventilation in Neonates Neurally Adjusted VentilatorydocsaravananNo ratings yet
- Revolutionise Your: WorkflowDocument6 pagesRevolutionise Your: WorkflowAly Arquillano JrNo ratings yet
- Ventilation During Lung Resection and Critical Care ComparativeDocument11 pagesVentilation During Lung Resection and Critical Care Comparativeema moralesNo ratings yet
- VNI en EmergencyDocument12 pagesVNI en Emergencyandres ruizNo ratings yet
- ARDS ParalisisDocument7 pagesARDS ParalisisMarvin M. Vargas AlayoNo ratings yet
- Awake Prone Positioning in Acute Hypoxaemic Respiratory FailureDocument17 pagesAwake Prone Positioning in Acute Hypoxaemic Respiratory FailurePaulaNo ratings yet
- Jerath2020 Article InhalationalVolatile-basedSedaDocument4 pagesJerath2020 Article InhalationalVolatile-basedSedasncr.gnyNo ratings yet
- Newer Modes of Ventilation2Document9 pagesNewer Modes of Ventilation2Saradha PellatiNo ratings yet
- Chen 2015Document6 pagesChen 2015Manuel MesaNo ratings yet
- Kacmarek2020 Article NeurallyAdjustedVentilatoryAssDocument11 pagesKacmarek2020 Article NeurallyAdjustedVentilatoryAssHoracio Panzardo GonzálezNo ratings yet
- Chest: Point/Counterpoint EditorialsDocument3 pagesChest: Point/Counterpoint Editorialsgiseladelarosa2006No ratings yet
- New Insights in Mechanical Ventilation and Adjunctive Therapies in ARDSDocument11 pagesNew Insights in Mechanical Ventilation and Adjunctive Therapies in ARDSKarina Vanessa María Llanos YupanquiNo ratings yet
- Terapia Adjunta en SdraDocument23 pagesTerapia Adjunta en SdraMarcoNo ratings yet
- Early Initiation MV 2017 - DR - TrisnaDocument34 pagesEarly Initiation MV 2017 - DR - TrisnaHappy ShalalaNo ratings yet
- Thorax00324 0009Document3 pagesThorax00324 0009distributor.company.ivanovoNo ratings yet
- Allison 2016 Non Invasive Ventilation For The EM PhysicianDocument12 pagesAllison 2016 Non Invasive Ventilation For The EM PhysicianSuwandi AlghozyNo ratings yet
- Comment: Lancet Respir Med 2017Document2 pagesComment: Lancet Respir Med 2017Novy DitaNo ratings yet
- RESP Failure in The ICU 2Document12 pagesRESP Failure in The ICU 2Keith SaccoNo ratings yet
- 9mechanical Ventilation in Sepsis-Induced Acute LungDocument6 pages9mechanical Ventilation in Sepsis-Induced Acute LungTeodora ZamfirescuNo ratings yet
- New and Unconventional Treatments For Obstructive Sleep ApneaDocument8 pagesNew and Unconventional Treatments For Obstructive Sleep Apnea杨钦杰No ratings yet
- Invasive Mechanical Ventilation PDFDocument4 pagesInvasive Mechanical Ventilation PDFRaquel AguilarNo ratings yet
- Newer Modes of Ventilation5Document12 pagesNewer Modes of Ventilation5Saradha PellatiNo ratings yet
- Hospital Monitoring, Setting and Training For Home NIVDocument4 pagesHospital Monitoring, Setting and Training For Home NIVPaoly PalmaNo ratings yet
- Rclutamiento VAFO Pre Surfactante PTDocument7 pagesRclutamiento VAFO Pre Surfactante PTGustavo Carhuamaca RoblesNo ratings yet
- Airway Pressure Release Ventilation: Theory and Practice: P. Milo Frawley, RN, MS, and Nader M. Habashi, MDDocument13 pagesAirway Pressure Release Ventilation: Theory and Practice: P. Milo Frawley, RN, MS, and Nader M. Habashi, MDLiliana AusechaNo ratings yet
- The Role of NM Blockers in ARDS - Benefits and RisksDocument8 pagesThe Role of NM Blockers in ARDS - Benefits and RisksMahendran R MahiNo ratings yet
- I - PAV+ Clinical Summary - Georgopoulos Et AlDocument2 pagesI - PAV+ Clinical Summary - Georgopoulos Et AlJuan Genaro Martinez PeñaNo ratings yet
- Acute Life-Threatening Hypoxemia During Mechanical VentilationDocument8 pagesAcute Life-Threatening Hypoxemia During Mechanical VentilationCesar Rivas CamposNo ratings yet
- Grieco Et Al-2023-Intensive Care MedicineDocument4 pagesGrieco Et Al-2023-Intensive Care MedicineDr Vikas GuptaNo ratings yet
- Physiotherapy and Airway Clearance Techniques and Devices: Maggie McilwaineDocument3 pagesPhysiotherapy and Airway Clearance Techniques and Devices: Maggie Mcilwaineحسام الوجيهNo ratings yet
- Acute Medicine Surgery - 2024 - Hoshino - Future Directions of Lung Protective Ventilation Strategies in AcuteDocument8 pagesAcute Medicine Surgery - 2024 - Hoshino - Future Directions of Lung Protective Ventilation Strategies in AcuteDiego AzevedoNo ratings yet
- Noninvasive Ventilation Strategy For PatientsDocument6 pagesNoninvasive Ventilation Strategy For PatientsannysNo ratings yet
- Direcciones Futuras de Las Estrategias de Ventilación Con Protección Pulmonar en El Síndrome de Dificultad Respiratoria Aguda - Hoshino - 2024Document11 pagesDirecciones Futuras de Las Estrategias de Ventilación Con Protección Pulmonar en El Síndrome de Dificultad Respiratoria Aguda - Hoshino - 2024eavasiNo ratings yet
- Borges 2006 Plateau 60Document11 pagesBorges 2006 Plateau 60pablopg_5No ratings yet
- Nasal High-Frequency VentilationDocument22 pagesNasal High-Frequency VentilationdragajojicNo ratings yet
- Respiratory - ARDS Vent Revised - QuestionsDocument6 pagesRespiratory - ARDS Vent Revised - QuestionsRyan ReNo ratings yet
- VPP No InvasivaDocument12 pagesVPP No InvasivaItzel AgustínNo ratings yet
- 43 Adaptive Support Ventilation As VDocument5 pages43 Adaptive Support Ventilation As Vnanang criztaNo ratings yet
- Continuous Positive Airway Pressure Mitigates Opioid-Induced Worsening of Sleep-Disordered Breathing Early After Bariatric SurgeryDocument13 pagesContinuous Positive Airway Pressure Mitigates Opioid-Induced Worsening of Sleep-Disordered Breathing Early After Bariatric SurgeryAnonymous lF3962RA1cNo ratings yet
- Hakala2000 PDFDocument7 pagesHakala2000 PDFVanshika GuptaNo ratings yet
- Effects of Prone Position On The Oxygenation of Patients With Acute Respiratory Distress SyndromeDocument6 pagesEffects of Prone Position On The Oxygenation of Patients With Acute Respiratory Distress Syndromeade_liaNo ratings yet
- Accepted Manuscript: Journal of HepatologyDocument45 pagesAccepted Manuscript: Journal of HepatologyLuis Enrique Caceres AlavrezNo ratings yet
- 31200753: Sepsis Personalization V ProtocolizationDocument6 pages31200753: Sepsis Personalization V ProtocolizationLuis Enrique Caceres AlavrezNo ratings yet
- 31137010: MANAGEMENT OF ENDOCRINE DISEASE Predictive Scores in Autoimmune Thyroid Disease. Are They Useful PDFDocument13 pages31137010: MANAGEMENT OF ENDOCRINE DISEASE Predictive Scores in Autoimmune Thyroid Disease. Are They Useful PDFLuis Enrique Caceres AlavrezNo ratings yet
- 31106572: Deconstructing Hyperlactatemia in Sepsis Using ScvO 2 and Base Deficit PDFDocument9 pages31106572: Deconstructing Hyperlactatemia in Sepsis Using ScvO 2 and Base Deficit PDFLuis Enrique Caceres AlavrezNo ratings yet
- 30926722: 2019 Update of The EULAR Recommendations For The Management of Systemic Lupus ErythematosusDocument10 pages30926722: 2019 Update of The EULAR Recommendations For The Management of Systemic Lupus ErythematosusLuis Enrique Caceres AlavrezNo ratings yet
- Peer Review Process: Author: Section Editor: Deputy EditorDocument14 pagesPeer Review Process: Author: Section Editor: Deputy EditorLuis Enrique Caceres AlavrezNo ratings yet
- Peer Review Process: Author: Section Editor: Deputy EditorDocument10 pagesPeer Review Process: Author: Section Editor: Deputy EditorLuis Enrique Caceres AlavrezNo ratings yet
- Lesson Plan in Tle SubjectDocument11 pagesLesson Plan in Tle SubjectJonaiza PangandianNo ratings yet
- Jurnal Pentingnya Memelihara Kebersihan Dan Keamanan Lingkungan Secarapartisipatif Demi Meningkatkan Gotong Royong Dan Kualitas Hidup WargaDocument1 pageJurnal Pentingnya Memelihara Kebersihan Dan Keamanan Lingkungan Secarapartisipatif Demi Meningkatkan Gotong Royong Dan Kualitas Hidup Wargaeko sutarkoNo ratings yet
- Health Insurance Premium CalculatorDocument15 pagesHealth Insurance Premium CalculatorqwertyNo ratings yet
- Class 11 - EDocument7 pagesClass 11 - EAnitha SathiaseelanNo ratings yet
- Powering Past Pain With Sustainable Profitability Initiating at Buy and 12 Price TargetDocument22 pagesPowering Past Pain With Sustainable Profitability Initiating at Buy and 12 Price TargetHans NokeNo ratings yet
- 1983 - Lawton - Environment and Other Determinants of Well-Being in Older PeopleDocument9 pages1983 - Lawton - Environment and Other Determinants of Well-Being in Older PeoplezigfriNo ratings yet
- GNHCPDocument210 pagesGNHCPSuryavenkat RaghavanNo ratings yet
- Safety Data Sheet: Starchem LLCDocument8 pagesSafety Data Sheet: Starchem LLCnailuj9614No ratings yet
- Long-Term Outcome Characteristics in Mesial Temporal Lobe Epilepsy With and Without Associated Cortical DysplasiaDocument10 pagesLong-Term Outcome Characteristics in Mesial Temporal Lobe Epilepsy With and Without Associated Cortical DysplasiaGesael Passos Ferreira JuniorNo ratings yet
- Tooth Numbering System: Whydoweneed?Document3 pagesTooth Numbering System: Whydoweneed?najwan domaNo ratings yet
- CHC33015-AC-HACC-Subject 4-AWB-F-v2.5Document45 pagesCHC33015-AC-HACC-Subject 4-AWB-F-v2.5Ashesh Basnet100% (6)
- Parole AgreementDocument6 pagesParole AgreementKUTV 2News100% (1)
- The Tyranny of Neuronormativity QuestionDocument16 pagesThe Tyranny of Neuronormativity QuestionSandra SandersNo ratings yet
- Transfer Via Bangkok Is Not Yet PossibleDocument4 pagesTransfer Via Bangkok Is Not Yet PossibleIan CeladaNo ratings yet
- (Cambridge Studies in Social and Emotional Development) Ofra Mayseless - Parenting Representations - Theory, Research, and Clinical Implications-Cambridge University Press (2006)Document487 pages(Cambridge Studies in Social and Emotional Development) Ofra Mayseless - Parenting Representations - Theory, Research, and Clinical Implications-Cambridge University Press (2006)Claudia HoreanuNo ratings yet
- Laboratory Activity 4.2Document5 pagesLaboratory Activity 4.2Paolo CampanoNo ratings yet
- Sarah Stone - 22personal Legend Project 22Document6 pagesSarah Stone - 22personal Legend Project 22api-552019617No ratings yet
- Policy DocumentDocument5 pagesPolicy DocumentmanojsalinNo ratings yet
- Flexor Tendon InjuriesDocument12 pagesFlexor Tendon InjuriesFrancis CarterNo ratings yet
- Stolen Generations PDFDocument4 pagesStolen Generations PDFIndiana JonesNo ratings yet
- Incidence of Recurrent Laryngeal Nerve Palsy Following Thyroid SurgeryDocument25 pagesIncidence of Recurrent Laryngeal Nerve Palsy Following Thyroid SurgeryAshokNo ratings yet
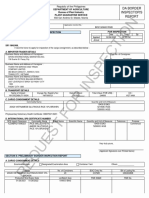
- Da Border Inspector'S: Republic of The PhilippinesDocument3 pagesDa Border Inspector'S: Republic of The PhilippinesPaul TanNo ratings yet
- ANCADocument1 pageANCAMuvenn KannanNo ratings yet
- Advertisement For MHADA Recruitment 2021 DTD 17-9-2021Document18 pagesAdvertisement For MHADA Recruitment 2021 DTD 17-9-2021SureshSawantNo ratings yet
- Dabsa SDSDocument13 pagesDabsa SDSKC Lakshmi NarayananNo ratings yet
- Las Week 7 Peh12Document6 pagesLas Week 7 Peh12Rheena-Ann Dupale PadillaNo ratings yet
- Cover, Part I & IIDocument45 pagesCover, Part I & IIMA. CRISTINA SERVANDONo ratings yet
- Riverside Medical College College of Nursing Professor: Jessie Daclis Topic: Communicable Diseases Day 1Document2 pagesRiverside Medical College College of Nursing Professor: Jessie Daclis Topic: Communicable Diseases Day 1Trixie Adaley Xen HeirenciaNo ratings yet