
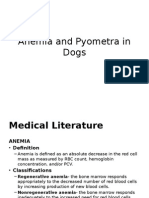
Common Rodenticide Toxicity
Common Rodenticide Toxicity
You might also like
- My Pre Fpgee QuestionsDocument17 pagesMy Pre Fpgee QuestionsAbdallahAbuodeh100% (1)
- Revised II Power Point Presentation Mark Schocken January 9 2023 2Document17 pagesRevised II Power Point Presentation Mark Schocken January 9 2023 2api-649165466No ratings yet
- Pediatric PoisoningDocument47 pagesPediatric PoisoningDr-Jagadeesh Mangamoori75% (4)
- Bloomberg ReferenceDocument112 pagesBloomberg Referencephitoeng100% (1)
- 501 Must-See MoviesDocument9 pages501 Must-See MoviesBranislavZivanovNo ratings yet
- Rodenticides: Topic Fact SheetDocument7 pagesRodenticides: Topic Fact Sheet152338No ratings yet
- Question 2Document4 pagesQuestion 2painx7No ratings yet
- Small Animal Transfusion Medicine - 2020 - VSPDocument12 pagesSmall Animal Transfusion Medicine - 2020 - VSPTactvisNo ratings yet
- Therapeutic Contraindications in Exotic PetsDocument14 pagesTherapeutic Contraindications in Exotic Pets黃皓No ratings yet
- Antibiotic Residue in FoodsDocument33 pagesAntibiotic Residue in FoodsAbhishek PandeyNo ratings yet
- Anemia and Pyometra in DogsDocument20 pagesAnemia and Pyometra in DogsVer FajaNo ratings yet
- ToxicDocument13 pagesToxicنوف الحربي.No ratings yet
- Cross SpeciesDocument475 pagesCross SpeciesSadam HussainNo ratings yet
- Insulin: Siemens Medical Solutions DiagnosticsDocument43 pagesInsulin: Siemens Medical Solutions DiagnosticsDaniel SolanoNo ratings yet
- Abram Study NotesDocument6 pagesAbram Study Notesteeman2No ratings yet
- Research ArticleDocument13 pagesResearch ArticleJames Cojab SacalNo ratings yet
- Dsis 198Document18 pagesDsis 198bvladimirov85No ratings yet
- Antineoplastic DrugsDocument38 pagesAntineoplastic DrugsTrixia CamporedondoNo ratings yet
- 10 1016@j Jpainsymman 2010 07 001Document5 pages10 1016@j Jpainsymman 2010 07 001Hugo Robles GómezNo ratings yet
- EVMS Critical Care COVID-19 Protocol PDFDocument18 pagesEVMS Critical Care COVID-19 Protocol PDFGreyWolf1776No ratings yet
- Hrana Otrovna Za PseDocument3 pagesHrana Otrovna Za PseJulijana SobotaNo ratings yet
- Blood Therapy, TPN Blood Banking: MedicationsDocument11 pagesBlood Therapy, TPN Blood Banking: Medicationsン ホアNo ratings yet
- Anticoagulants: Dr. Hassan Mohamed EnowDocument37 pagesAnticoagulants: Dr. Hassan Mohamed EnowFatimaNo ratings yet
- Khloroform: 1. 1. Product Identification Identifikasi ProdukDocument21 pagesKhloroform: 1. 1. Product Identification Identifikasi ProdukAntonio_Ipang_8256No ratings yet
- Paclitaxel: Orders Support WebDocument2 pagesPaclitaxel: Orders Support WebineedsomebooksNo ratings yet
- JULAUG 2014 - Selected PagesDocument5 pagesJULAUG 2014 - Selected PagesStephen PopeNo ratings yet
- Nclex Notes 1Document17 pagesNclex Notes 1itokumo100% (2)
- Diseases of Dairy: GoatsDocument13 pagesDiseases of Dairy: GoatsalarochaNo ratings yet
- Practice: Investigating Hyperkalaemia in AdultsDocument6 pagesPractice: Investigating Hyperkalaemia in AdultsJbarrianNo ratings yet
- T CholesterolDocument5 pagesT CholesterolDuc Nguyen ManhNo ratings yet
- Licence VPA10454-025-001 25052018155256Document5 pagesLicence VPA10454-025-001 25052018155256Khalida MuddasserNo ratings yet
- Session 9ABC - English For Pharmacy and Engineering Students - Vocabulary & ThesaurusDocument33 pagesSession 9ABC - English For Pharmacy and Engineering Students - Vocabulary & Thesauruslyra ayuNo ratings yet
- Mclean 2018Document16 pagesMclean 2018sdiqrxkzwkepyexpboNo ratings yet
- Laboratory ExamsDocument8 pagesLaboratory ExamsARIANE DOLINONo ratings yet
- Clinical Veterinary Advisor, 3rd Edition BabesiosisDocument5 pagesClinical Veterinary Advisor, 3rd Edition Babesiosisbio_trip160% (1)
- Australian Public Assessment Report For Human Prothrombin ComplexDocument51 pagesAustralian Public Assessment Report For Human Prothrombin ComplexTriponiaNo ratings yet
- AntiarrhythmiaDocument29 pagesAntiarrhythmiaDRx Raju ChandranNo ratings yet
- Thesis On Beta CaroteneDocument5 pagesThesis On Beta Carotenehmnxivief100% (2)
- American Family Physician PDFDocument8 pagesAmerican Family Physician PDFlionaNo ratings yet
- April 2019-0Document25 pagesApril 2019-0SEIYADU IBRAHIM KNo ratings yet
- 1.4 DEXTRAN-A Valuable Plasma Volume Expander. Dr.a.J.leonsins.Document6 pages1.4 DEXTRAN-A Valuable Plasma Volume Expander. Dr.a.J.leonsins.rajeevtyagi41No ratings yet
- Canine Hypoadrenocorticism Overvew Diagnosis and Treatment LolattiDocument6 pagesCanine Hypoadrenocorticism Overvew Diagnosis and Treatment LolattiAna Clara SevasteNo ratings yet
- MIRA KESUMA - Tugas Resume Jurnal - TEBDocument9 pagesMIRA KESUMA - Tugas Resume Jurnal - TEBksm vlogNo ratings yet
- Acute Respiratory Distress SyndromeDocument4 pagesAcute Respiratory Distress SyndromeBianca WelchNo ratings yet
- General Pricnciples in Apheresis SOPDocument2 pagesGeneral Pricnciples in Apheresis SOPvadivel aruNo ratings yet
- Evms Critical Care Covid-19 Management Protocol: Paul Marik, MDDocument9 pagesEvms Critical Care Covid-19 Management Protocol: Paul Marik, MDJohn GaltNo ratings yet
- Talc Chemical PleurodesisDocument4 pagesTalc Chemical Pleurodesismastan shaikNo ratings yet
- Ricinus Communis: Toxic PlantsDocument21 pagesRicinus Communis: Toxic PlantsRoman MamunNo ratings yet
- د. ﺣﻴ ﺪ ر اﳌﻴ ﺎ ﱄ Pediatric PoisoningDocument9 pagesد. ﺣﻴ ﺪ ر اﳌﻴ ﺎ ﱄ Pediatric Poisoningمسلم هاشم منافNo ratings yet
- Antihyperlipidemic Activity of Chloroxylon Swietenia in Triton WR1339 Induced HyperlipidemiaDocument7 pagesAntihyperlipidemic Activity of Chloroxylon Swietenia in Triton WR1339 Induced HyperlipidemiaDharmendra SawNo ratings yet
- HematologyDocument198 pagesHematologyLouann100% (1)
- Creative Commons Attribution LicenseDocument10 pagesCreative Commons Attribution LicenseSitty Salma Hadji AbbasNo ratings yet
- Definition:: Ii.D. Laboratory and Diagnostic TestsDocument3 pagesDefinition:: Ii.D. Laboratory and Diagnostic TestsKimberly Ann Azores AlcazarenNo ratings yet
- The Efficacy of Antioxidant (Vitamin C) in The Treatment and Management of MalariaDocument7 pagesThe Efficacy of Antioxidant (Vitamin C) in The Treatment and Management of MalariaManswi MoreNo ratings yet
- CxuchingDocument4 pagesCxuchingMussme DelgadoNo ratings yet
- A Case of Accidental Ricin Poisoning: Edward Despott, Mario J CachiaDocument3 pagesA Case of Accidental Ricin Poisoning: Edward Despott, Mario J CachiaAlexander MirandaNo ratings yet
- Summary Review Orig1s000SumRDocument26 pagesSummary Review Orig1s000SumRAlvaro MuñozNo ratings yet
- C1-Pediatrics 5th-Lec 1Document10 pagesC1-Pediatrics 5th-Lec 1عمر احمد شاكرNo ratings yet
- Clopidogrel and Aspirin For The Treatment of Polycythemia VeraDocument7 pagesClopidogrel and Aspirin For The Treatment of Polycythemia VeraYagz Hachiko ClarosNo ratings yet
- Evms Critical Care Covid-19 Management Protocol: Paul Marik, MDDocument11 pagesEvms Critical Care Covid-19 Management Protocol: Paul Marik, MDPrashanta Barman Palas100% (1)
- Customer Perception Towards Digital Payments in IndiaDocument61 pagesCustomer Perception Towards Digital Payments in IndiaPunita Kumari100% (1)
- Zara Case StudyDocument4 pagesZara Case StudyKishanth RajaramNo ratings yet
- Inspiring Leaders April 2023Document54 pagesInspiring Leaders April 2023Jay MenonNo ratings yet
- Themes From Stage BeautyDocument3 pagesThemes From Stage BeautycattykernNo ratings yet
- Hurst CyclesDocument5 pagesHurst CyclesTheodoros Maragakis100% (2)
- Transcript Consolidated Commission of Inquiry in To Post Violence 1 August 2018 Final PDFDocument1,290 pagesTranscript Consolidated Commission of Inquiry in To Post Violence 1 August 2018 Final PDFKudakwashe Mpambi100% (1)
- Curriculum VitaeDocument4 pagesCurriculum VitaeAmit KumarNo ratings yet
- Sex, Gender, Sexuality and Reproductive HealthDocument26 pagesSex, Gender, Sexuality and Reproductive HealthKaycee Daya-Magos100% (1)
- End Compulsory SchoolingDocument18 pagesEnd Compulsory SchoolingIndependence Institute100% (1)
- Reci Za PssDocument113 pagesReci Za PssMilos HajdukovicNo ratings yet
- 2022 Communicable Disease Reference Guide For SchoolsDocument118 pages2022 Communicable Disease Reference Guide For Schoolsmohan s vNo ratings yet
- Inventory of Drug Taking SituationsDocument2 pagesInventory of Drug Taking SituationsMacarena Segovia ReygadasNo ratings yet
- OGL 481 Pro-Seminar I: PCA-Symbolic Frame WorksheetDocument4 pagesOGL 481 Pro-Seminar I: PCA-Symbolic Frame Worksheetapi-538926640No ratings yet
- G9 - FA - Task 2 - U2Document3 pagesG9 - FA - Task 2 - U2Lizzy AnthonyNo ratings yet
- Music History Exam 2 Study GuideDocument4 pagesMusic History Exam 2 Study GuideHaley CoxNo ratings yet
- A Manual of KHSHNOOM The Zoroastrian Occult KnowledgeDocument491 pagesA Manual of KHSHNOOM The Zoroastrian Occult KnowledgeBryan Bethke III100% (3)
- Legal Maxim AssignmentDocument15 pagesLegal Maxim AssignmentrethiramNo ratings yet
- Goa University Entrepreneurship Development Sem V SyllabusDocument3 pagesGoa University Entrepreneurship Development Sem V SyllabusMyron VazNo ratings yet
- Introduction To Logic and Critical Thinking: Lansing Community CollegeDocument17 pagesIntroduction To Logic and Critical Thinking: Lansing Community CollegeMiyNo ratings yet
- Discrete-Time Processing of Speech Signals (IEEE Press Classic Reissue) PDFDocument919 pagesDiscrete-Time Processing of Speech Signals (IEEE Press Classic Reissue) PDFAnonymous bZtJlFvPtpNo ratings yet
- Very Low Drop Voltage Regulator: DescriptionDocument8 pagesVery Low Drop Voltage Regulator: DescriptionJhonatan CervantesNo ratings yet
- Lesson Plan FormatDocument5 pagesLesson Plan FormatAlex TutorNo ratings yet
- Disha Workshop ReportDocument4 pagesDisha Workshop ReportkolkarevinayNo ratings yet
- Buddhism Lamp PDFDocument193 pagesBuddhism Lamp PDFrajeshteeNo ratings yet
- BBM203 - Kierrtana - 071190094Document11 pagesBBM203 - Kierrtana - 071190094kierrtanaNo ratings yet
- HOMEof The AshfallDocument4 pagesHOMEof The AshfallJohn John EstiponaNo ratings yet
- Chapter 2c - EEDocument32 pagesChapter 2c - EEHarithZakariaNo ratings yet
- Manuel S. Enverga University Foundation Granted Autonomous StatusDocument9 pagesManuel S. Enverga University Foundation Granted Autonomous StatusJanine MadriagaNo ratings yet
























































































Download as pdf or txt
You might also like
- My Pre Fpgee QuestionsDocument17 pagesMy Pre Fpgee QuestionsAbdallahAbuodeh100% (1)
- Revised II Power Point Presentation Mark Schocken January 9 2023 2Document17 pagesRevised II Power Point Presentation Mark Schocken January 9 2023 2api-649165466No ratings yet
- Pediatric PoisoningDocument47 pagesPediatric PoisoningDr-Jagadeesh Mangamoori75% (4)
- Bloomberg ReferenceDocument112 pagesBloomberg Referencephitoeng100% (1)
- 501 Must-See MoviesDocument9 pages501 Must-See MoviesBranislavZivanovNo ratings yet
- Rodenticides: Topic Fact SheetDocument7 pagesRodenticides: Topic Fact Sheet152338No ratings yet
- Question 2Document4 pagesQuestion 2painx7No ratings yet
- Small Animal Transfusion Medicine - 2020 - VSPDocument12 pagesSmall Animal Transfusion Medicine - 2020 - VSPTactvisNo ratings yet
- Therapeutic Contraindications in Exotic PetsDocument14 pagesTherapeutic Contraindications in Exotic Pets黃皓No ratings yet
- Antibiotic Residue in FoodsDocument33 pagesAntibiotic Residue in FoodsAbhishek PandeyNo ratings yet
- Anemia and Pyometra in DogsDocument20 pagesAnemia and Pyometra in DogsVer FajaNo ratings yet
- ToxicDocument13 pagesToxicنوف الحربي.No ratings yet
- Cross SpeciesDocument475 pagesCross SpeciesSadam HussainNo ratings yet
- Insulin: Siemens Medical Solutions DiagnosticsDocument43 pagesInsulin: Siemens Medical Solutions DiagnosticsDaniel SolanoNo ratings yet
- Abram Study NotesDocument6 pagesAbram Study Notesteeman2No ratings yet
- Research ArticleDocument13 pagesResearch ArticleJames Cojab SacalNo ratings yet
- Dsis 198Document18 pagesDsis 198bvladimirov85No ratings yet
- Antineoplastic DrugsDocument38 pagesAntineoplastic DrugsTrixia CamporedondoNo ratings yet
- 10 1016@j Jpainsymman 2010 07 001Document5 pages10 1016@j Jpainsymman 2010 07 001Hugo Robles GómezNo ratings yet
- EVMS Critical Care COVID-19 Protocol PDFDocument18 pagesEVMS Critical Care COVID-19 Protocol PDFGreyWolf1776No ratings yet
- Hrana Otrovna Za PseDocument3 pagesHrana Otrovna Za PseJulijana SobotaNo ratings yet
- Blood Therapy, TPN Blood Banking: MedicationsDocument11 pagesBlood Therapy, TPN Blood Banking: Medicationsン ホアNo ratings yet
- Anticoagulants: Dr. Hassan Mohamed EnowDocument37 pagesAnticoagulants: Dr. Hassan Mohamed EnowFatimaNo ratings yet
- Khloroform: 1. 1. Product Identification Identifikasi ProdukDocument21 pagesKhloroform: 1. 1. Product Identification Identifikasi ProdukAntonio_Ipang_8256No ratings yet
- Paclitaxel: Orders Support WebDocument2 pagesPaclitaxel: Orders Support WebineedsomebooksNo ratings yet
- JULAUG 2014 - Selected PagesDocument5 pagesJULAUG 2014 - Selected PagesStephen PopeNo ratings yet
- Nclex Notes 1Document17 pagesNclex Notes 1itokumo100% (2)
- Diseases of Dairy: GoatsDocument13 pagesDiseases of Dairy: GoatsalarochaNo ratings yet
- Practice: Investigating Hyperkalaemia in AdultsDocument6 pagesPractice: Investigating Hyperkalaemia in AdultsJbarrianNo ratings yet
- T CholesterolDocument5 pagesT CholesterolDuc Nguyen ManhNo ratings yet
- Licence VPA10454-025-001 25052018155256Document5 pagesLicence VPA10454-025-001 25052018155256Khalida MuddasserNo ratings yet
- Session 9ABC - English For Pharmacy and Engineering Students - Vocabulary & ThesaurusDocument33 pagesSession 9ABC - English For Pharmacy and Engineering Students - Vocabulary & Thesauruslyra ayuNo ratings yet
- Mclean 2018Document16 pagesMclean 2018sdiqrxkzwkepyexpboNo ratings yet
- Laboratory ExamsDocument8 pagesLaboratory ExamsARIANE DOLINONo ratings yet
- Clinical Veterinary Advisor, 3rd Edition BabesiosisDocument5 pagesClinical Veterinary Advisor, 3rd Edition Babesiosisbio_trip160% (1)
- Australian Public Assessment Report For Human Prothrombin ComplexDocument51 pagesAustralian Public Assessment Report For Human Prothrombin ComplexTriponiaNo ratings yet
- AntiarrhythmiaDocument29 pagesAntiarrhythmiaDRx Raju ChandranNo ratings yet
- Thesis On Beta CaroteneDocument5 pagesThesis On Beta Carotenehmnxivief100% (2)
- American Family Physician PDFDocument8 pagesAmerican Family Physician PDFlionaNo ratings yet
- April 2019-0Document25 pagesApril 2019-0SEIYADU IBRAHIM KNo ratings yet
- 1.4 DEXTRAN-A Valuable Plasma Volume Expander. Dr.a.J.leonsins.Document6 pages1.4 DEXTRAN-A Valuable Plasma Volume Expander. Dr.a.J.leonsins.rajeevtyagi41No ratings yet
- Canine Hypoadrenocorticism Overvew Diagnosis and Treatment LolattiDocument6 pagesCanine Hypoadrenocorticism Overvew Diagnosis and Treatment LolattiAna Clara SevasteNo ratings yet
- MIRA KESUMA - Tugas Resume Jurnal - TEBDocument9 pagesMIRA KESUMA - Tugas Resume Jurnal - TEBksm vlogNo ratings yet
- Acute Respiratory Distress SyndromeDocument4 pagesAcute Respiratory Distress SyndromeBianca WelchNo ratings yet
- General Pricnciples in Apheresis SOPDocument2 pagesGeneral Pricnciples in Apheresis SOPvadivel aruNo ratings yet
- Evms Critical Care Covid-19 Management Protocol: Paul Marik, MDDocument9 pagesEvms Critical Care Covid-19 Management Protocol: Paul Marik, MDJohn GaltNo ratings yet
- Talc Chemical PleurodesisDocument4 pagesTalc Chemical Pleurodesismastan shaikNo ratings yet
- Ricinus Communis: Toxic PlantsDocument21 pagesRicinus Communis: Toxic PlantsRoman MamunNo ratings yet
- د. ﺣﻴ ﺪ ر اﳌﻴ ﺎ ﱄ Pediatric PoisoningDocument9 pagesد. ﺣﻴ ﺪ ر اﳌﻴ ﺎ ﱄ Pediatric Poisoningمسلم هاشم منافNo ratings yet
- Antihyperlipidemic Activity of Chloroxylon Swietenia in Triton WR1339 Induced HyperlipidemiaDocument7 pagesAntihyperlipidemic Activity of Chloroxylon Swietenia in Triton WR1339 Induced HyperlipidemiaDharmendra SawNo ratings yet
- HematologyDocument198 pagesHematologyLouann100% (1)
- Creative Commons Attribution LicenseDocument10 pagesCreative Commons Attribution LicenseSitty Salma Hadji AbbasNo ratings yet
- Definition:: Ii.D. Laboratory and Diagnostic TestsDocument3 pagesDefinition:: Ii.D. Laboratory and Diagnostic TestsKimberly Ann Azores AlcazarenNo ratings yet
- The Efficacy of Antioxidant (Vitamin C) in The Treatment and Management of MalariaDocument7 pagesThe Efficacy of Antioxidant (Vitamin C) in The Treatment and Management of MalariaManswi MoreNo ratings yet
- CxuchingDocument4 pagesCxuchingMussme DelgadoNo ratings yet
- A Case of Accidental Ricin Poisoning: Edward Despott, Mario J CachiaDocument3 pagesA Case of Accidental Ricin Poisoning: Edward Despott, Mario J CachiaAlexander MirandaNo ratings yet
- Summary Review Orig1s000SumRDocument26 pagesSummary Review Orig1s000SumRAlvaro MuñozNo ratings yet
- C1-Pediatrics 5th-Lec 1Document10 pagesC1-Pediatrics 5th-Lec 1عمر احمد شاكرNo ratings yet
- Clopidogrel and Aspirin For The Treatment of Polycythemia VeraDocument7 pagesClopidogrel and Aspirin For The Treatment of Polycythemia VeraYagz Hachiko ClarosNo ratings yet
- Evms Critical Care Covid-19 Management Protocol: Paul Marik, MDDocument11 pagesEvms Critical Care Covid-19 Management Protocol: Paul Marik, MDPrashanta Barman Palas100% (1)
- Customer Perception Towards Digital Payments in IndiaDocument61 pagesCustomer Perception Towards Digital Payments in IndiaPunita Kumari100% (1)
- Zara Case StudyDocument4 pagesZara Case StudyKishanth RajaramNo ratings yet
- Inspiring Leaders April 2023Document54 pagesInspiring Leaders April 2023Jay MenonNo ratings yet
- Themes From Stage BeautyDocument3 pagesThemes From Stage BeautycattykernNo ratings yet
- Hurst CyclesDocument5 pagesHurst CyclesTheodoros Maragakis100% (2)
- Transcript Consolidated Commission of Inquiry in To Post Violence 1 August 2018 Final PDFDocument1,290 pagesTranscript Consolidated Commission of Inquiry in To Post Violence 1 August 2018 Final PDFKudakwashe Mpambi100% (1)
- Curriculum VitaeDocument4 pagesCurriculum VitaeAmit KumarNo ratings yet
- Sex, Gender, Sexuality and Reproductive HealthDocument26 pagesSex, Gender, Sexuality and Reproductive HealthKaycee Daya-Magos100% (1)
- End Compulsory SchoolingDocument18 pagesEnd Compulsory SchoolingIndependence Institute100% (1)
- Reci Za PssDocument113 pagesReci Za PssMilos HajdukovicNo ratings yet
- 2022 Communicable Disease Reference Guide For SchoolsDocument118 pages2022 Communicable Disease Reference Guide For Schoolsmohan s vNo ratings yet
- Inventory of Drug Taking SituationsDocument2 pagesInventory of Drug Taking SituationsMacarena Segovia ReygadasNo ratings yet
- OGL 481 Pro-Seminar I: PCA-Symbolic Frame WorksheetDocument4 pagesOGL 481 Pro-Seminar I: PCA-Symbolic Frame Worksheetapi-538926640No ratings yet
- G9 - FA - Task 2 - U2Document3 pagesG9 - FA - Task 2 - U2Lizzy AnthonyNo ratings yet
- Music History Exam 2 Study GuideDocument4 pagesMusic History Exam 2 Study GuideHaley CoxNo ratings yet
- A Manual of KHSHNOOM The Zoroastrian Occult KnowledgeDocument491 pagesA Manual of KHSHNOOM The Zoroastrian Occult KnowledgeBryan Bethke III100% (3)
- Legal Maxim AssignmentDocument15 pagesLegal Maxim AssignmentrethiramNo ratings yet
- Goa University Entrepreneurship Development Sem V SyllabusDocument3 pagesGoa University Entrepreneurship Development Sem V SyllabusMyron VazNo ratings yet
- Introduction To Logic and Critical Thinking: Lansing Community CollegeDocument17 pagesIntroduction To Logic and Critical Thinking: Lansing Community CollegeMiyNo ratings yet
- Discrete-Time Processing of Speech Signals (IEEE Press Classic Reissue) PDFDocument919 pagesDiscrete-Time Processing of Speech Signals (IEEE Press Classic Reissue) PDFAnonymous bZtJlFvPtpNo ratings yet
- Very Low Drop Voltage Regulator: DescriptionDocument8 pagesVery Low Drop Voltage Regulator: DescriptionJhonatan CervantesNo ratings yet
- Lesson Plan FormatDocument5 pagesLesson Plan FormatAlex TutorNo ratings yet
- Disha Workshop ReportDocument4 pagesDisha Workshop ReportkolkarevinayNo ratings yet
- Buddhism Lamp PDFDocument193 pagesBuddhism Lamp PDFrajeshteeNo ratings yet
- BBM203 - Kierrtana - 071190094Document11 pagesBBM203 - Kierrtana - 071190094kierrtanaNo ratings yet
- HOMEof The AshfallDocument4 pagesHOMEof The AshfallJohn John EstiponaNo ratings yet
- Chapter 2c - EEDocument32 pagesChapter 2c - EEHarithZakariaNo ratings yet
- Manuel S. Enverga University Foundation Granted Autonomous StatusDocument9 pagesManuel S. Enverga University Foundation Granted Autonomous StatusJanine MadriagaNo ratings yet