Download as pdf or txt
You might also like
- Bipolar Disorder Concept MapDocument1 pageBipolar Disorder Concept Mapnursing concept maps100% (1)
- Fonseca Et Al - 2017Document23 pagesFonseca Et Al - 2017TAINAH DE PAULANo ratings yet
- De Paula 2017Document21 pagesDe Paula 2017TAINAH DE PAULANo ratings yet
- Acute Resistance Exercise With Blood Flow Restriction Effects On Heart Rate, Double Product, Oxygen Saturation and Perceived ExertionDocument7 pagesAcute Resistance Exercise With Blood Flow Restriction Effects On Heart Rate, Double Product, Oxygen Saturation and Perceived ExertionJuanfran Montesinos GarciaNo ratings yet
- Farup Et Al-2015-Scandinavian Journal of Medicine & Science in SportsDocument10 pagesFarup Et Al-2015-Scandinavian Journal of Medicine & Science in SportsR.No ratings yet
- Sardeli2017 CV Respons To Diff Resistance Exerc ProtocolDocument9 pagesSardeli2017 CV Respons To Diff Resistance Exerc ProtocolMumtaz MaulanaNo ratings yet
- Haemodynamics of Aerobic and Resistance Blood Flow Restriction Exercise in Young and Older AdultsDocument10 pagesHaemodynamics of Aerobic and Resistance Blood Flow Restriction Exercise in Young and Older AdultsJuanfran Montesinos GarciaNo ratings yet
- Blood Flow Restriction Attenuates Eccentric Exercise-Induced Muscle Damage Without Perceptual and Cardiovascular OverloadDocument9 pagesBlood Flow Restriction Attenuates Eccentric Exercise-Induced Muscle Damage Without Perceptual and Cardiovascular OverloadJuanfran Montesinos GarciaNo ratings yet
- Inter HugoDocument10 pagesInter HugorizkaNo ratings yet
- Post-Concurrent Exercise Hemodynamics and Cardiac Autonomic ModulationDocument10 pagesPost-Concurrent Exercise Hemodynamics and Cardiac Autonomic ModulationTAINAH DE PAULANo ratings yet
- Experimental Gerontology: ArticleinfoDocument7 pagesExperimental Gerontology: ArticleinfoLaily Mita AndriaNo ratings yet
- The Journal of Physiology - 2024 - Brito - Evening But Not Morning Aerobic Training Improves Sympathetic Activity andDocument15 pagesThe Journal of Physiology - 2024 - Brito - Evening But Not Morning Aerobic Training Improves Sympathetic Activity andAnnah MeeloNo ratings yet
- A Single Session of Aerobic Exercise Reduces Systolic Blood Pressure at Rest and in Response To Stress in Women With Rheumatoid Arthritis and HypertensionDocument9 pagesA Single Session of Aerobic Exercise Reduces Systolic Blood Pressure at Rest and in Response To Stress in Women With Rheumatoid Arthritis and HypertensionRobles Murillo Carlos Eduardo Augusto 1FNo ratings yet
- Intra Dial y TicDocument8 pagesIntra Dial y Ticratna220693No ratings yet
- Blood Flow Restriction Training Induced - Hormonal - RDocument9 pagesBlood Flow Restriction Training Induced - Hormonal - RMateus José ArrudaNo ratings yet
- H E R E W B F R: Ypotensive Ffects of Esistance Xercises ITH Lood LOW EstrictionDocument7 pagesH E R E W B F R: Ypotensive Ffects of Esistance Xercises ITH Lood LOW EstrictionJuanfran Montesinos GarciaNo ratings yet
- BFRDocument24 pagesBFRCristine Ramos100% (1)
- Thomas (2020) - The Acute Effect of Resistance Exercise On Limb Blood Flow - Experimental PhysiologyDocument11 pagesThomas (2020) - The Acute Effect of Resistance Exercise On Limb Blood Flow - Experimental PhysiologyYuri OliveiraNo ratings yet
- Acute Skeletal Muscle Responses To Very Low-Load Resistance Exercise With and Without The Application of Blood Flow Restriction in The Upper BodyDocument8 pagesAcute Skeletal Muscle Responses To Very Low-Load Resistance Exercise With and Without The Application of Blood Flow Restriction in The Upper BodyFabiano LacerdaNo ratings yet
- Postexercise Hypotension in An Endurance-Trained Population of Men and Women Following High-Intensity Interval and Steady-State CyclingDocument10 pagesPostexercise Hypotension in An Endurance-Trained Population of Men and Women Following High-Intensity Interval and Steady-State Cyclingnuttela ismeNo ratings yet
- CPF 12145Document6 pagesCPF 12145Maria Yosephine WidiastutiNo ratings yet
- Artigo Completo Pei Fisio 1Document13 pagesArtigo Completo Pei Fisio 1harlley sanNo ratings yet
- Potential Safety Issues With Blood Ow Restriction Training: ReviewDocument9 pagesPotential Safety Issues With Blood Ow Restriction Training: ReviewJuanfran Montesinos GarciaNo ratings yet
- 2006 Post-Resistance Exercise Hypotension Influence of IntensityDocument8 pages2006 Post-Resistance Exercise Hypotension Influence of IntensityDavid HaluliNo ratings yet
- Acute Response Aerobic Exercise Following CabgDocument6 pagesAcute Response Aerobic Exercise Following CabgAmelia SianiparNo ratings yet
- Cardiovascular and Perceptual Responses To Blood-Flow-Restricted Resistance Exercise With Differing Restrictive CuffsDocument7 pagesCardiovascular and Perceptual Responses To Blood-Flow-Restricted Resistance Exercise With Differing Restrictive CuffsJuanfran Montesinos GarciaNo ratings yet
- Lasevicius2018 PDFDocument10 pagesLasevicius2018 PDFAgustinaNo ratings yet
- Tensión Arterial y Ejercicio de FuerzaDocument8 pagesTensión Arterial y Ejercicio de Fuerzaabraham landaetaNo ratings yet
- Peripheral Heart Action (PHA) Training As A Valid Substitute To High Intensity Interval Training To Improve Resting Cardiovascular Changes and Autonomic Adaptation Piras201Document11 pagesPeripheral Heart Action (PHA) Training As A Valid Substitute To High Intensity Interval Training To Improve Resting Cardiovascular Changes and Autonomic Adaptation Piras201jojoNo ratings yet
- Dissimilar Physiological and Perceptual Responses Between Sprint Interval Training and High-Intensity Interval TrainingDocument7 pagesDissimilar Physiological and Perceptual Responses Between Sprint Interval Training and High-Intensity Interval TrainingDouglas MarinNo ratings yet
- Comparação Entre o Treinamento Resistido de Baixa Intensidade Com Restrição de Fluxo e Alta Intensidade Na Força e Massa Muscular Do Quadríceps em IdosoDocument7 pagesComparação Entre o Treinamento Resistido de Baixa Intensidade Com Restrição de Fluxo e Alta Intensidade Na Força e Massa Muscular Do Quadríceps em IdosoEder Lemos de SantanaNo ratings yet
- The Training and Detraining Effect of High Intensity Interval Training On Post Exercise Hypotension in Young Overweight/obese WomenDocument8 pagesThe Training and Detraining Effect of High Intensity Interval Training On Post Exercise Hypotension in Young Overweight/obese WomenLeticia N. S. NevesNo ratings yet
- (Human Movement) Blood Pressure Responses After A Session of Functional Training in Young Adults and The Elderly A Pilot StudyDocument7 pages(Human Movement) Blood Pressure Responses After A Session of Functional Training in Young Adults and The Elderly A Pilot StudyEvaNo ratings yet
- Evening But Not Morning Aerobic Training Improves Sympathetic Activity and Baroreflex Sensitivity in Elderly Patients With Treated HypertensionDocument15 pagesEvening But Not Morning Aerobic Training Improves Sympathetic Activity and Baroreflex Sensitivity in Elderly Patients With Treated HypertensionCintia Matos de MeloNo ratings yet
- Moderately Heavy Exercise Produces Lower Cardiovascular, RPE, and Discomfort Compared To Lower Load Exercise With and Without Blood Flow RestrictionDocument8 pagesModerately Heavy Exercise Produces Lower Cardiovascular, RPE, and Discomfort Compared To Lower Load Exercise With and Without Blood Flow RestrictionJuanfran Montesinos GarciaNo ratings yet
- 3 - 2014 - JGABSMS - Effects of Low-Load, Elastic Band Resistance TrainingDocument10 pages3 - 2014 - JGABSMS - Effects of Low-Load, Elastic Band Resistance TrainingFelipe PereiraNo ratings yet
- Low-Load Resistance Training With Blood - Flow Restriction in Relation To Muscle Function, Mass, and Functionality in Women With Rheumatoid ArthritisDocument11 pagesLow-Load Resistance Training With Blood - Flow Restriction in Relation To Muscle Function, Mass, and Functionality in Women With Rheumatoid ArthritissanaullahNo ratings yet
- Acute Hypotensive Response To Continuous and Accumulated Isocaloric Aerobic BoutsDocument8 pagesAcute Hypotensive Response To Continuous and Accumulated Isocaloric Aerobic BoutsLeticia N. S. NevesNo ratings yet
- Letter To The Editor Hydrotherapy in Heart Failure: A Case: BackgroundDocument4 pagesLetter To The Editor Hydrotherapy in Heart Failure: A Case: BackgroundElizabete MonteiroNo ratings yet
- Potential Adverse Cardiovascular Effects From Excessive Endurance ExerciseDocument9 pagesPotential Adverse Cardiovascular Effects From Excessive Endurance Exercisewfaachannel8No ratings yet
- Aerobic Versus Isometric Handgrip Exercise in Hypertension: A Randomized Controlled TrialDocument8 pagesAerobic Versus Isometric Handgrip Exercise in Hypertension: A Randomized Controlled TrialROSANo ratings yet
- Blood Ow Restriction Augments The Skeletal Muscle Response During Very Low-Load Resistance Exercise To Volitional FailureDocument14 pagesBlood Ow Restriction Augments The Skeletal Muscle Response During Very Low-Load Resistance Exercise To Volitional FailureFabiano LacerdaNo ratings yet
- Szivak 2013 - HISRDocument13 pagesSzivak 2013 - HISRjk trainerNo ratings yet
- Associations Between Borgs' Rating of Perceived Exertion and Physiological Measures of Exercise Intensity # ControlDocument9 pagesAssociations Between Borgs' Rating of Perceived Exertion and Physiological Measures of Exercise Intensity # ControlVinicius Fallux QueirozNo ratings yet
- Muscle Failure Promotes Greater Muscle Hypertrophy in Low-Load But Not in High-Load Resistance TrainingDocument7 pagesMuscle Failure Promotes Greater Muscle Hypertrophy in Low-Load But Not in High-Load Resistance TrainingCaio MarquesNo ratings yet
- McCarthyetal 2023-SimilarPEHfollowingMICTHIITSITDocument9 pagesMcCarthyetal 2023-SimilarPEHfollowingMICTHIITSITCintia Matos de MeloNo ratings yet
- Physical Activity and Fitness For The Prevention of HypertensionDocument8 pagesPhysical Activity and Fitness For The Prevention of HypertensionFerdy LainsamputtyNo ratings yet
- Protocolo Fuerza HandgripDocument5 pagesProtocolo Fuerza HandgripValeria Tabares SanchezNo ratings yet
- Muscle Size and Arterial Stiffness After Blood Flow-Restricted Low-Intensity Resistance Training in Older AdultsDocument8 pagesMuscle Size and Arterial Stiffness After Blood Flow-Restricted Low-Intensity Resistance Training in Older AdultsEvanio SousaNo ratings yet
- Effects of Ace Inhibitors and Angiotensin Type 1.1266Document1 pageEffects of Ace Inhibitors and Angiotensin Type 1.1266Anett Pappné LeppNo ratings yet
- Effects of Exercise Intensity and Occlusion Pressure After 12 Weeks of Resistance Training With Blood - Ow RestrictionDocument11 pagesEffects of Exercise Intensity and Occlusion Pressure After 12 Weeks of Resistance Training With Blood - Ow RestrictionRoberto Bernárdez VázquezNo ratings yet
- JEPonlineJUNE2018 SachaClael PDFDocument8 pagesJEPonlineJUNE2018 SachaClael PDFFabiano LacerdaNo ratings yet
- 2022 Strength Training For Arterial Hypertension Treatment A Systematic Review and Meta-Analysis of Randomize Clinical TrialsDocument15 pages2022 Strength Training For Arterial Hypertension Treatment A Systematic Review and Meta-Analysis of Randomize Clinical TrialsAntofa V EndeNo ratings yet
- Review Article: Acute Effects of Exercise On Blood Pressure: A Meta-Analytic InvestigationDocument12 pagesReview Article: Acute Effects of Exercise On Blood Pressure: A Meta-Analytic InvestigationFisio KineticNo ratings yet
- P H A C, A I, S I E: Ostexercise Ypotension Fter Ontinuous Erobic Nterval AND Print Nterval XerciseDocument6 pagesP H A C, A I, S I E: Ostexercise Ypotension Fter Ontinuous Erobic Nterval AND Print Nterval Xercisenuttela ismeNo ratings yet
- Muscle Failure Promotes Greater Muscle Hypertrophy in Low-Load But Not in High-Load Resistance TrainingDocument6 pagesMuscle Failure Promotes Greater Muscle Hypertrophy in Low-Load But Not in High-Load Resistance TrainingGabrielDosAnjosNo ratings yet
- Am J Hypertens 2015 Sharman 147 58Document12 pagesAm J Hypertens 2015 Sharman 147 58yusnadiNo ratings yet
- Association of Heart Rate and Heart Rate Variability With An Anaerobic Performance Test and Recovery of Brazilian Jiu-Jitsu AthletesDocument14 pagesAssociation of Heart Rate and Heart Rate Variability With An Anaerobic Performance Test and Recovery of Brazilian Jiu-Jitsu AthletesBruno CastroNo ratings yet
- Ladlow Et Al. 2018 PDFDocument14 pagesLadlow Et Al. 2018 PDFmatheus ramosNo ratings yet
- Marchese 2019 Controlled Study of Central Hemodynamic ChangesDocument8 pagesMarchese 2019 Controlled Study of Central Hemodynamic Changestaaaatan.04No ratings yet
- Complementary and Alternative Medical Lab Testing Part 4: VascularFrom EverandComplementary and Alternative Medical Lab Testing Part 4: VascularNo ratings yet
- Moderately Heavy Exercise Produces Lower Cardiovascular, RPE, and Discomfort Compared To Lower Load Exercise With and Without Blood Flow RestrictionDocument8 pagesModerately Heavy Exercise Produces Lower Cardiovascular, RPE, and Discomfort Compared To Lower Load Exercise With and Without Blood Flow RestrictionJuanfran Montesinos GarciaNo ratings yet
- Potential Safety Issues With Blood Ow Restriction Training: ReviewDocument9 pagesPotential Safety Issues With Blood Ow Restriction Training: ReviewJuanfran Montesinos GarciaNo ratings yet
- Blood Flow Restriction Attenuates Eccentric Exercise-Induced Muscle Damage Without Perceptual and Cardiovascular OverloadDocument9 pagesBlood Flow Restriction Attenuates Eccentric Exercise-Induced Muscle Damage Without Perceptual and Cardiovascular OverloadJuanfran Montesinos GarciaNo ratings yet
- Post-Exercise Aortic Hemodynamic Responses To Low-Intensity Resistance Exercise With and Without Vascular OcclusionDocument6 pagesPost-Exercise Aortic Hemodynamic Responses To Low-Intensity Resistance Exercise With and Without Vascular OcclusionJuanfran Montesinos GarciaNo ratings yet
- T A R P O K E: HE Cute Esponse of Ractical Cclusion in THE NEE XtensorsDocument4 pagesT A R P O K E: HE Cute Esponse of Ractical Cclusion in THE NEE XtensorsJuanfran Montesinos GarciaNo ratings yet
- H E R E W B F R: Ypotensive Ffects of Esistance Xercises ITH Lood LOW EstrictionDocument7 pagesH E R E W B F R: Ypotensive Ffects of Esistance Xercises ITH Lood LOW EstrictionJuanfran Montesinos GarciaNo ratings yet
- Cardiovascular and Perceptual Responses To Blood-Flow-Restricted Resistance Exercise With Differing Restrictive CuffsDocument7 pagesCardiovascular and Perceptual Responses To Blood-Flow-Restricted Resistance Exercise With Differing Restrictive CuffsJuanfran Montesinos GarciaNo ratings yet
- Takano2005 PDFDocument9 pagesTakano2005 PDFJuanfran Montesinos GarciaNo ratings yet
- Haemodynamics of Aerobic and Resistance Blood Flow Restriction Exercise in Young and Older AdultsDocument10 pagesHaemodynamics of Aerobic and Resistance Blood Flow Restriction Exercise in Young and Older AdultsJuanfran Montesinos GarciaNo ratings yet
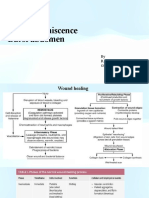
- Wound Dehiscence Burst Abdomen: by R.V.Kalyani Gen Surgery V UnitDocument25 pagesWound Dehiscence Burst Abdomen: by R.V.Kalyani Gen Surgery V Unitvinitha kattaNo ratings yet
- Different Physiotherapy Protocols After Coronary Artery Bypass Graft Surgery: A Randomized Controlled TrialDocument8 pagesDifferent Physiotherapy Protocols After Coronary Artery Bypass Graft Surgery: A Randomized Controlled Trialratnayanti udinNo ratings yet
- Client Package Manual (Magsaysay - WestfalLarsen Management AS)Document8 pagesClient Package Manual (Magsaysay - WestfalLarsen Management AS)Shalinur GonzalesNo ratings yet
- PHENYLEPHRINEDocument3 pagesPHENYLEPHRINERoger Jr PumarenNo ratings yet
- Kahoot (1) MergedDocument8 pagesKahoot (1) MergedNathaly MoraNo ratings yet
- Managing The Difficult Soft Tissue Envelope in Facial and Rhinoplasty SurgeryDocument15 pagesManaging The Difficult Soft Tissue Envelope in Facial and Rhinoplasty SurgeryFabian Camelo OtorrinoNo ratings yet
- Psychotherapy For BPDDocument5 pagesPsychotherapy For BPDJuanaNo ratings yet
- Mock 1 Answer Key:: AnatomyDocument34 pagesMock 1 Answer Key:: AnatomyPambala Krishna100% (1)
- Fawcett Et Al (2020) Medicalisation - An Enduring ConceptDocument14 pagesFawcett Et Al (2020) Medicalisation - An Enduring ConceptEHNo ratings yet
- Thyroid Tumors: Subtitle Headline Dr. DeaDocument34 pagesThyroid Tumors: Subtitle Headline Dr. Deanaili nsnNo ratings yet
- Homeopathy The Human Medicine Leon VannierDocument5 pagesHomeopathy The Human Medicine Leon VannierAbhiram Banerjee100% (2)
- Oral Tuberculosis: Negin Hekmatjoo (1702169) Armin Hekmatjoo (1702183)Document12 pagesOral Tuberculosis: Negin Hekmatjoo (1702169) Armin Hekmatjoo (1702183)Negin HekmatjooNo ratings yet
- Gastric Outlet ObstructionDocument59 pagesGastric Outlet Obstructionmaryam tariqNo ratings yet
- Colloidal Gold and Silver - The Use of Colloidal Gold - Then and NowDocument11 pagesColloidal Gold and Silver - The Use of Colloidal Gold - Then and NowDevon NarokNo ratings yet
- Davis-Oparil2018Document17 pagesDavis-Oparil2018neeraj glaNo ratings yet
- Transplantation and Rejection 2022Document25 pagesTransplantation and Rejection 2022malkalhmaidh03No ratings yet
- HLS19 Q12 NO - English (10116)Document1 pageHLS19 Q12 NO - English (10116)陳順玲No ratings yet
- ReflectionDocument2 pagesReflectionapi-283689862No ratings yet
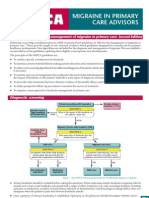
- National Guidelines - MigraineDocument4 pagesNational Guidelines - MigraineSean CardozoNo ratings yet
- EntireDrugPack - BFN FINAL 090217 PDFDocument134 pagesEntireDrugPack - BFN FINAL 090217 PDFDeny HudaNo ratings yet
- Psychological Changes of A Pregnant WomanDocument4 pagesPsychological Changes of A Pregnant WomanEuna Patricia AguilarNo ratings yet
- (Cocos Nucifera) The Tree of Life: Coconut in Modern MedicineDocument6 pages(Cocos Nucifera) The Tree of Life: Coconut in Modern MedicineAdharsh ShankaranNo ratings yet
- Acynotic DiseaseDocument55 pagesAcynotic DiseaseTesfamichael AbathunNo ratings yet
- Case Study ReportDocument23 pagesCase Study Reportapi-290866384No ratings yet
- Miliue Therapy Skill PDFDocument1 pageMiliue Therapy Skill PDFRosalinda SalvadorNo ratings yet
- Nilai Ankle Brachial Index (Abi) Dengan Neuropati Perifer Diabetik Pada Pasien Diabetes Melitus Tipe 2Document9 pagesNilai Ankle Brachial Index (Abi) Dengan Neuropati Perifer Diabetik Pada Pasien Diabetes Melitus Tipe 2Khadidjah HaniaNo ratings yet
- Chapter 16: Breastfeeding Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionDocument4 pagesChapter 16: Breastfeeding Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionHelen UgochukwuNo ratings yet
- Electrocardiograph Y (ECG / Ekg) : Rose Dyane F - Nunag, RMT, MPHDocument52 pagesElectrocardiograph Y (ECG / Ekg) : Rose Dyane F - Nunag, RMT, MPHClaire GonoNo ratings yet
- PcolDocument17 pagesPcolThea JulianaNo ratings yet