Download as pdf or txt
You might also like
- 8 - Maxillary Expansion in Nongrowing Patients. Conventional, SurgicalDocument11 pages8 - Maxillary Expansion in Nongrowing Patients. Conventional, SurgicalMariana SantosNo ratings yet
- SD-V9N1 Bosshart CompleteDocument7 pagesSD-V9N1 Bosshart CompleteAnonymous gjrAZMXB3No ratings yet
- Metis Cookbook and Guide To Healthy Living - Second EditionDocument112 pagesMetis Cookbook and Guide To Healthy Living - Second EditionRecipeRain100% (4)
- 2.plough and Power The Economic and Social Significance of Cultivation With Ox Drawn 1Document7 pages2.plough and Power The Economic and Social Significance of Cultivation With Ox Drawn 1formatcsdNo ratings yet
- Scion - The Wiccan PantheonDocument5 pagesScion - The Wiccan Pantheonbrothersale100% (2)
- Preprosthetic SurgeryDocument4 pagesPreprosthetic SurgeryVero AngelNo ratings yet
- Increasing Vertical DimensionDocument6 pagesIncreasing Vertical DimensionAriel AcevedoNo ratings yet
- Kokich CaninosDocument6 pagesKokich CaninosMercedes RojasNo ratings yet
- Kokich Missing Laterals PDFDocument6 pagesKokich Missing Laterals PDFShatabdi A ChakravartyNo ratings yet
- The Timing of Orthodontic TreatmentDocument8 pagesThe Timing of Orthodontic TreatmentcareNo ratings yet
- How To Become A WerewolfDocument4 pagesHow To Become A WerewolfOscar WildNo ratings yet
- Knitting - 153 - April 2016Document100 pagesKnitting - 153 - April 2016Minh Anh100% (10)
- East of The Sus and West of The Moon by Tina HoweDocument29 pagesEast of The Sus and West of The Moon by Tina HoweMark MirandoNo ratings yet
- E1 MJAFImaxexpansionusingquadhelixinclp2009Document5 pagesE1 MJAFImaxexpansionusingquadhelixinclp2009ريام الموسويNo ratings yet
- Considerations For Establishing and Maintaining Proper Occlusion in The Aesthetic Zone - Dentistry TodayDocument12 pagesConsiderations For Establishing and Maintaining Proper Occlusion in The Aesthetic Zone - Dentistry Todayaziz2007No ratings yet
- Orthodontic AnchorageDocument8 pagesOrthodontic Anchoragetderiaty100% (1)
- Orthodontic Expansion: Orthodontic Expansion, Produced by Conventional Fixed Appliances As Well As by Various RemovableDocument7 pagesOrthodontic Expansion: Orthodontic Expansion, Produced by Conventional Fixed Appliances As Well As by Various RemovableNiTa DöéMy HarDianaNo ratings yet
- Management of Missing Teeth KokichDocument6 pagesManagement of Missing Teeth KokichTaufiqurrahman Abdul DjabbarNo ratings yet
- Management of Anterior Dental Crossbite With Removable AppliancesDocument4 pagesManagement of Anterior Dental Crossbite With Removable AppliancesSurya WijayaNo ratings yet
- International Dental and Medical Journal of Advanced ResearchDocument5 pagesInternational Dental and Medical Journal of Advanced ResearchShirmayne TangNo ratings yet
- Management of Impacted Maxillary Canines Using Mandibular AnchorageDocument4 pagesManagement of Impacted Maxillary Canines Using Mandibular Anchoragedrsankhya100% (1)
- Content ServerDocument4 pagesContent ServerJose Antonio Figuroa AbadoNo ratings yet
- Space ManagementDocument28 pagesSpace ManagementReena Chacko100% (1)
- Pre Prosthetic SurgeryDocument29 pagesPre Prosthetic SurgeryDentist HereNo ratings yet
- Applsci 11 00607Document10 pagesApplsci 11 00607Yerly RamirezNo ratings yet
- HSRF TopouhDocument2 pagesHSRF TopouhJordan KiddNo ratings yet
- Canine Impaction Different MethodsDocument11 pagesCanine Impaction Different MethodsMSHNo ratings yet
- Ped. Dent, Pub. Health (2) - 5 - Space MaintainerDocument19 pagesPed. Dent, Pub. Health (2) - 5 - Space MaintainerEslam HafezNo ratings yet
- Expansion Rapida 111111111111 PDFDocument12 pagesExpansion Rapida 111111111111 PDFjoserodrrNo ratings yet
- Orthodontics - 7th LectureDocument6 pagesOrthodontics - 7th LectureMarwan Qasim GhNo ratings yet
- Ecde 10 00327Document8 pagesEcde 10 00327Erisa BllakajNo ratings yet
- EffectofpositioningDocument7 pagesEffectofpositioningSkAliHassanNo ratings yet
- Cheek PlumperDocument6 pagesCheek PlumperDivya DahiyaNo ratings yet
- Flat Ridgel Impression TechniqueDocument4 pagesFlat Ridgel Impression TechniquerekabiNo ratings yet
- Practical Techniques For Achieving Improved Accuracy in Bracket PositioningDocument14 pagesPractical Techniques For Achieving Improved Accuracy in Bracket Positioninganon-976413No ratings yet
- Slow Maxillary Expansion A Review 209085c4Document12 pagesSlow Maxillary Expansion A Review 209085c4jabbarNo ratings yet
- 3 4 761Document3 pages3 4 761Sonia KumariNo ratings yet
- Maintenance of Gingival Form Following Implant PlacementDocument4 pagesMaintenance of Gingival Form Following Implant PlacementRomina BitaNo ratings yet
- Surgical-Orthodontic Expansion of The: MaxillaDocument12 pagesSurgical-Orthodontic Expansion of The: MaxillaAna LauraNo ratings yet
- Component of Extraction ForcepsDocument8 pagesComponent of Extraction ForcepsDr-Ahmed HamoodNo ratings yet
- 2016 Article 143Document7 pages2016 Article 143Andrea TokumotoNo ratings yet
- Distalising Molars How Do You Do It 31 03 2015Document21 pagesDistalising Molars How Do You Do It 31 03 2015Dorian GrayNo ratings yet
- RetrieveDocument7 pagesRetrievelinaNo ratings yet
- Single Complete DentureDocument12 pagesSingle Complete DentureHarsha Reddy100% (1)
- Compomer CrownDocument2 pagesCompomer CrownIndah SimamoraNo ratings yet
- Soft-Tissue Undercuts in Denture PlacementDocument4 pagesSoft-Tissue Undercuts in Denture Placementdrgayen6042No ratings yet
- Hybridhyrax 180211141507 PDFDocument42 pagesHybridhyrax 180211141507 PDFNgo Viet ThanhNo ratings yet
- Basic Principles of Obturator Design IIDocument7 pagesBasic Principles of Obturator Design IIGilberto Arturo Huapaya MarcosNo ratings yet
- Concepts of Occlusion in Prosthodontics: A Literature ReviewDocument6 pagesConcepts of Occlusion in Prosthodontics: A Literature ReviewMostafa FayadNo ratings yet
- 1 s2.0 S2212443823000371 MainDocument11 pages1 s2.0 S2212443823000371 MainMirza GlusacNo ratings yet
- Full Crown Module 2786Document16 pagesFull Crown Module 2786Mustafa S. KoperlyNo ratings yet
- Chapter 4 Space MaintenanceDocument17 pagesChapter 4 Space MaintenanceMarwan AlamriNo ratings yet
- Flangeless CDDocument6 pagesFlangeless CDDivya DahiyaNo ratings yet
- Neutral ZoneDocument4 pagesNeutral ZonedrsmritiNo ratings yet
- Arvystas 1998Document4 pagesArvystas 1998Саша АптреевNo ratings yet
- M.andibular Implants in Young PatientDocument16 pagesM.andibular Implants in Young PatientAna MaríaNo ratings yet
- Jurnal Labial Bow ModifikaisDocument10 pagesJurnal Labial Bow Modifikaisdinda wrNo ratings yet
- Interesting Eruption of 4 Teeth Associated With A Large Dentigerous Cyst in Mandible by Only MarsupializationDocument3 pagesInteresting Eruption of 4 Teeth Associated With A Large Dentigerous Cyst in Mandible by Only MarsupializationAnupama NagrajNo ratings yet
- Management Flabby RidgeDocument4 pagesManagement Flabby RidgeNidya Patricia Sembiring100% (1)
- Publication 4 8339 1696Document9 pagesPublication 4 8339 1696habeebNo ratings yet
- Serial ExtractionDocument9 pagesSerial ExtractionFarheen MahmoodaNo ratings yet
- Write Up of Removable AppliancesDocument17 pagesWrite Up of Removable AppliancesSaurabh SinghNo ratings yet
- Klasifikasi AramanyDocument7 pagesKlasifikasi AramanyErwin SutonoNo ratings yet
- Board of Trustees of The Leland Stanford Junior University v. Roche Molecular Systems, Inc. Et Al - Document No. 172Document8 pagesBoard of Trustees of The Leland Stanford Junior University v. Roche Molecular Systems, Inc. Et Al - Document No. 172Justia.comNo ratings yet
- Major Connectors IN RPDDocument47 pagesMajor Connectors IN RPDaakankshakanwarNo ratings yet
- Ielts Reading 4Document16 pagesIelts Reading 4nguyenhoaind2No ratings yet
- Area of Activities of VPHDocument16 pagesArea of Activities of VPHAlpesh Suthar100% (1)
- Puzzle 1Document12 pagesPuzzle 1Brundaban MohapatraNo ratings yet
- Respon Sinkronisasi Berahi Pada Induk Sapi Potong Dengan Skor Kondisi Tubuh Berbeda Pada Peternakan RakyatDocument7 pagesRespon Sinkronisasi Berahi Pada Induk Sapi Potong Dengan Skor Kondisi Tubuh Berbeda Pada Peternakan RakyatMaksar Muhuruna LaodeNo ratings yet
- Tazkia Grade 8 Degree of ComparisonDocument6 pagesTazkia Grade 8 Degree of ComparisonMiftahul AzizahNo ratings yet
- Guitar Songs For Spring 2021Document19 pagesGuitar Songs For Spring 2021Lauren NielsonNo ratings yet
- Earthworm BehaviorsDocument6 pagesEarthworm BehaviorskellymcnameeNo ratings yet
- Guyton and Hall Textbook of Medical Physiology 12th Ed p0775Document2 pagesGuyton and Hall Textbook of Medical Physiology 12th Ed p0775Maryama AflahaNo ratings yet
- Artificial Insemination-Swine CG PDFDocument9 pagesArtificial Insemination-Swine CG PDFLloyl MonteroNo ratings yet
- SYLLABUS GRADE 9 ScienceDocument3 pagesSYLLABUS GRADE 9 ScienceCienna Dayao del RosarioNo ratings yet
- Tailieunhanh Dieutrinhikhoadongy 2 352Document130 pagesTailieunhanh Dieutrinhikhoadongy 2 35211010706No ratings yet
- Sindrom Nefritik DebDocument2 pagesSindrom Nefritik DebrchristevenNo ratings yet
- Occlusal Equilibration PDFDocument1 pageOcclusal Equilibration PDFindah anggarainiNo ratings yet
- Malaria ReviewerDocument6 pagesMalaria ReviewerManis SantiagoNo ratings yet
- Reflection Title: Story "Mr. Bunny's Carrot Soup"Document3 pagesReflection Title: Story "Mr. Bunny's Carrot Soup"api-296835930No ratings yet
- Claire Bolalin - Quiz (Neurulation)Document1 pageClaire Bolalin - Quiz (Neurulation)Claire BolalinNo ratings yet
- ПрезентаціяDocument38 pagesПрезентаціяЕлена СклярNo ratings yet
- External Disease and CorneaDocument105 pagesExternal Disease and CorneaNova CiNg CiNgNo ratings yet
- Breathing and The Valsalva Meneuver. Part 1Document5 pagesBreathing and The Valsalva Meneuver. Part 1alextrbnNo ratings yet
- Adayatthezoo: All Resources ©2020 Literacy ShedDocument4 pagesAdayatthezoo: All Resources ©2020 Literacy ShedPaola del Moral100% (1)
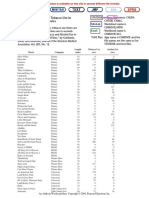
- Data Set 7: Alcohol and Tobacco Use in Animated Children's MoviesDocument1 pageData Set 7: Alcohol and Tobacco Use in Animated Children's MoviesBishop PantaNo ratings yet
- MGT538 - Reflection Report - Group 1Document21 pagesMGT538 - Reflection Report - Group 1aniskhadijahsayutiNo ratings yet