Download as pdf or txt
You might also like
- Midpoints - Unleashing The POwer of The PlanetsDocument394 pagesMidpoints - Unleashing The POwer of The PlanetsAngela Gibson98% (104)
- Taste of Paradise Chapter 2Document16 pagesTaste of Paradise Chapter 2Gisele Ferreira33% (6)
- LS Magazine Ls Models Ls Land Issue Video LSM lsm09 08 02 Mega PDFDocument4 pagesLS Magazine Ls Models Ls Land Issue Video LSM lsm09 08 02 Mega PDFPaul25% (4)
- Chemrite Grout NSDocument2 pagesChemrite Grout NSghazanfar0% (1)
- Guided Wave System ComparisonDocument3 pagesGuided Wave System ComparisonsenthilndtNo ratings yet
- BS 8110Document9 pagesBS 8110Priyadarshini Sahoo100% (1)
- Quantitative Exam Sample For NMATDocument2 pagesQuantitative Exam Sample For NMATJenica YambsNo ratings yet
- Chrysotile Key Facts - 180419 Final - 0Document6 pagesChrysotile Key Facts - 180419 Final - 0Guillermo VillamizarNo ratings yet
- Ijerph 18 02053 v2Document16 pagesIjerph 18 02053 v2Firman Kusuma AtmajaNo ratings yet
- S 016 AsbeDocument8 pagesS 016 Asberendra boyke2023No ratings yet
- Asbestosis StatPearls NCBIBookshelfDocument11 pagesAsbestosis StatPearls NCBIBookshelfAjeng RahmawatiNo ratings yet
- Elimination Asbestos-Related Diseases ENDocument4 pagesElimination Asbestos-Related Diseases ENtimky8No ratings yet
- Cancer Incidence in Asbestos Exposed Workers An Updat 2017 Safety and HealtDocument6 pagesCancer Incidence in Asbestos Exposed Workers An Updat 2017 Safety and HealtFelicia Enriqueta López AscarzaNo ratings yet
- Environmental Exposure To Airborne Asbestos FibresDocument9 pagesEnvironmental Exposure To Airborne Asbestos FibresAziza AzizaNo ratings yet
- Environmental Asbestos Exposure and Risk of MesotheliomaDocument11 pagesEnvironmental Asbestos Exposure and Risk of MesotheliomaStavya DubeyNo ratings yet
- Asbestos On Ships: How To Manage It SafelyDocument48 pagesAsbestos On Ships: How To Manage It SafelyHashem GamNo ratings yet
- Asbestos Information: Sources and Types of AsbestosDocument5 pagesAsbestos Information: Sources and Types of AsbestosAli AltafNo ratings yet
- Notes: - Subpart Number: Z - Subpart Title: Toxic and Hazardous SubstancesDocument12 pagesNotes: - Subpart Number: Z - Subpart Title: Toxic and Hazardous Substancesmalik jahanNo ratings yet
- Imaging of Asbestos-Related Lung and Pleural Diseases As An Endemic Exposure in EgyptDocument7 pagesImaging of Asbestos-Related Lung and Pleural Diseases As An Endemic Exposure in Egyptoralposter PIPKRA2023No ratings yet
- Asbestos AwarenessDocument14 pagesAsbestos AwarenessSAQIBNo ratings yet
- AsbestosDocument27 pagesAsbestosMao ConstantinoNo ratings yet
- 2004 The Epidemiology of Asbestos-Related DiseasesDocument9 pages2004 The Epidemiology of Asbestos-Related Diseasesxiongmao2389No ratings yet
- Asbestos Download Able GatewayDocument8 pagesAsbestos Download Able Gatewaychan49No ratings yet
- Alumina Nanofiber Filters FS Feb 2011Document2 pagesAlumina Nanofiber Filters FS Feb 2011Sya'roni ImamNo ratings yet
- AsbestosDocument2 pagesAsbestosNurNo ratings yet
- PERFORMANCE TASK 1 Gen ChemDocument4 pagesPERFORMANCE TASK 1 Gen ChemHannah Marie GatpolintanNo ratings yet
- Toxicity AsDocument14 pagesToxicity AsHiệu Nguyễn QuangNo ratings yet
- New Zealand Asbestos RisksDocument16 pagesNew Zealand Asbestos RisksNgumi Wa GithaigaNo ratings yet
- Abbasi 2019Document12 pagesAbbasi 2019stefanpopovic1211No ratings yet
- Role of MicroRNAs in Lung Carcinogenesis Induced by AsbestosDocument23 pagesRole of MicroRNAs in Lung Carcinogenesis Induced by AsbestosRao UmerNo ratings yet
- Asbestos and Cancer RiskDocument9 pagesAsbestos and Cancer Riskmuadz hilmyNo ratings yet
- Asbestos-: Other Health Effects of AsbestosDocument12 pagesAsbestos-: Other Health Effects of AsbestosRegie NojaldaNo ratings yet
- Global Asbestos Disaster: Environmental Research and Public HealthDocument11 pagesGlobal Asbestos Disaster: Environmental Research and Public HealthThiago Campos MeiraNo ratings yet
- Research Report On Asbestos in The AirDocument12 pagesResearch Report On Asbestos in The Airdenis edembaNo ratings yet
- Rainwater Harvesting and Asbestos RoofingDocument4 pagesRainwater Harvesting and Asbestos RoofingGreen Action Sustainable Technology GroupNo ratings yet
- Asbestos: An Overview For CliniciansDocument4 pagesAsbestos: An Overview For CliniciansginaNo ratings yet
- Respiratory Diseases Among Dust Exposed WorkersDocument19 pagesRespiratory Diseases Among Dust Exposed WorkersAR MalikNo ratings yet
- 1 s2.0 S2093791118300933 MainDocument5 pages1 s2.0 S2093791118300933 Maincartoon lovely storyNo ratings yet
- CadmiumDocument18 pagesCadmiumMy Brain FartsNo ratings yet
- AsbestosDocument1 pageAsbestosVALENZUELA DELIESA E.No ratings yet
- Translatean AsbestosDocument1 pageTranslatean AsbestosAlya HafidzaNo ratings yet
- 10 - Ramazzini Asbestos Is Still With Us Repeat Call For A Universal BanDocument7 pages10 - Ramazzini Asbestos Is Still With Us Repeat Call For A Universal BanHedda Michelle Guevara NietoNo ratings yet
- The Effect of CuSO 4 For Establishing in Vitro Culture, and The Role Nitrogen and Iron Sources in in Vitro Multiplication of Corylus Avellana L. Cv. Tonda Gentile RomanaDocument9 pagesThe Effect of CuSO 4 For Establishing in Vitro Culture, and The Role Nitrogen and Iron Sources in in Vitro Multiplication of Corylus Avellana L. Cv. Tonda Gentile RomanaCarlos RomeroNo ratings yet
- Pulmonary Mineral Fibers After Occupational and Environmental Exposure To Asbestos in The Russian Chrysotile IndustryDocument7 pagesPulmonary Mineral Fibers After Occupational and Environmental Exposure To Asbestos in The Russian Chrysotile IndustrycthjgfytvfnoNo ratings yet
- 04 - Bartrip History of Asbestos Related DiseaseDocument5 pages04 - Bartrip History of Asbestos Related DiseaseHedda Michelle Guevara NietoNo ratings yet
- Safety and Health at Work: Types and Health Hazards of Fibrous Materials Used As Asbestos SubstitutesDocument6 pagesSafety and Health at Work: Types and Health Hazards of Fibrous Materials Used As Asbestos SubstitutescumikkNo ratings yet
- 2 - The Burden of Asbestos-Related DiseasesDocument45 pages2 - The Burden of Asbestos-Related DiseasesMuhammad HasbiNo ratings yet
- Review ArticleDocument12 pagesReview ArticlemikhaelyosiaNo ratings yet
- Sir Shahid Review PaperDocument12 pagesSir Shahid Review PaperSaweeraNo ratings yet
- Science of The Total Environment: Daniel López-Muñoz, M . Amparo Ochoa-Zapater, Amparo Torreblanca, M . Dolores GarceráDocument7 pagesScience of The Total Environment: Daniel López-Muñoz, M . Amparo Ochoa-Zapater, Amparo Torreblanca, M . Dolores GarceráGemmaNo ratings yet
- Manifiesto de AsbestoDocument11 pagesManifiesto de AsbestoFrancisco SanchezNo ratings yet
- Aluminum ToxicityDocument13 pagesAluminum ToxicityFeyi AsgillNo ratings yet
- GCMS Batch Equilibrium Study and Adsorption Isotherms of Atrazine Sorption by Activated H3PO4 - TreaDocument12 pagesGCMS Batch Equilibrium Study and Adsorption Isotherms of Atrazine Sorption by Activated H3PO4 - TreaZackkNo ratings yet
- Present Status of Asbestos Mining and Related Health Problems in India - A SurveyDocument7 pagesPresent Status of Asbestos Mining and Related Health Problems in India - A Surveyesclusivos1No ratings yet
- Occupational Exposure To Asbestos During Renovation of Oil Shale Fuelled Power Plants in EstoniaDocument7 pagesOccupational Exposure To Asbestos During Renovation of Oil Shale Fuelled Power Plants in EstoniaBruno ThiemeNo ratings yet
- 10 1002@jat 3910Document27 pages10 1002@jat 3910Zahra Nur AzizaNo ratings yet
- Association Between Iron Deficiency and Hearing Loss: Biochemical and Cellular Archives June 2019Document7 pagesAssociation Between Iron Deficiency and Hearing Loss: Biochemical and Cellular Archives June 2019JuanNo ratings yet
- Articulo de RevistaDocument15 pagesArticulo de RevistasergioNo ratings yet
- Use of Ozone in The Food IndustryDocument8 pagesUse of Ozone in The Food IndustrysrLeoSalazarNo ratings yet
- Oligodynamic Effect of Precious Metal On Skin BacteriaDocument8 pagesOligodynamic Effect of Precious Metal On Skin BacteriaEmmanuel BawaNo ratings yet
- Asbestos: From Wikipedia, The Free Encyclopedia Jump To:, For Other Uses, SeeDocument26 pagesAsbestos: From Wikipedia, The Free Encyclopedia Jump To:, For Other Uses, SeeSonorizari BrasovNo ratings yet
- Chemical Hazards MT......Document32 pagesChemical Hazards MT......mayuri zanwarNo ratings yet
- 10 Hematopoietic Toxicity in Wistar Rats Experimental-3Document20 pages10 Hematopoietic Toxicity in Wistar Rats Experimental-3Owonikoko MathewNo ratings yet
- Ijerph 13 01223 v2Document24 pagesIjerph 13 01223 v2Rajesh TripathyNo ratings yet
- tmpF545 TMPDocument6 pagestmpF545 TMPFrontiersNo ratings yet
- 23-Tseng - Correlation of An Immune-Related 8-Gene Panel With Pathologic Response To NAC in BCDocument9 pages23-Tseng - Correlation of An Immune-Related 8-Gene Panel With Pathologic Response To NAC in BCMichelle Guevara-NietoNo ratings yet
- MedicinaDocument25 pagesMedicinaMichelle Guevara-NietoNo ratings yet
- 19 - Mandel Potential-Problem Determining-Elongate-Mineral-ParticleDocument2 pages19 - Mandel Potential-Problem Determining-Elongate-Mineral-ParticleMichelle Guevara-NietoNo ratings yet
- Cohen 2016Document17 pagesCohen 2016Michelle Guevara-NietoNo ratings yet
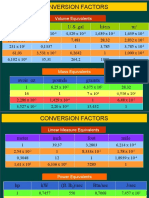
- Conversion Factors: in FT U.S. Gal Liters MDocument8 pagesConversion Factors: in FT U.S. Gal Liters MSamuel MahendraNo ratings yet
- TM25RDocument2 pagesTM25Rphong nguyễn bá0% (1)
- Cat C32 ACERT Spec Sheet - Pleasure CraftDocument8 pagesCat C32 ACERT Spec Sheet - Pleasure CraftSteven Wong100% (1)
- Streamlines Shape Hull PDFDocument15 pagesStreamlines Shape Hull PDFdleanteNo ratings yet
- Piano Tuning GuidelinesDocument6 pagesPiano Tuning GuidelinesAleksandraMladenovićNo ratings yet
- REPORTDocument6 pagesREPORTrachana singhNo ratings yet
- LECTURE 1. PUMPS and FANS.Document21 pagesLECTURE 1. PUMPS and FANS.RocsNo ratings yet
- Makgantai - Journal of Xi'an University of Architecture & Technology - 2021Document18 pagesMakgantai - Journal of Xi'an University of Architecture & Technology - 2021Adi SetiyawanNo ratings yet
- Test Certificate For Vista Superplast Hs 400 Consignee: Dhariwal Buildtech Ltd. Quantity: 22.022 MT Date: 14-12-2022 Batch No.: VK/2022-23/228Document1 pageTest Certificate For Vista Superplast Hs 400 Consignee: Dhariwal Buildtech Ltd. Quantity: 22.022 MT Date: 14-12-2022 Batch No.: VK/2022-23/228Deepak PachauriaNo ratings yet
- Msds Hydrogen PeroxideDocument2 pagesMsds Hydrogen PeroxideSlamet Ar100% (1)
- JBL+Boombox+ND+vV1 0Document37 pagesJBL+Boombox+ND+vV1 0Gilson Pereira100% (1)
- Si47 1971 Frenic Lift Loader Im WebDocument128 pagesSi47 1971 Frenic Lift Loader Im WebLogic EngineeringNo ratings yet
- Basic Driving Instructor CourseDocument9 pagesBasic Driving Instructor CourseRafael AbdullaNo ratings yet
- Poultry Anatomy and PhysiologyDocument40 pagesPoultry Anatomy and PhysiologyMamtaNo ratings yet
- Grade 9 TOSDocument4 pagesGrade 9 TOSManuel EsponillaNo ratings yet
- Control Panel ETV 0551Document40 pagesControl Panel ETV 0551Thillainathan So ThanabhalanNo ratings yet
- Chapter 1 - CONCEPT OF PLANT BIOTECH AGT 566Document33 pagesChapter 1 - CONCEPT OF PLANT BIOTECH AGT 566Xwag 12No ratings yet
- DSTV PDFDocument4 pagesDSTV PDFEddy TangaNo ratings yet
- TIS REV5 BRAINFARMA Brasile 1-055-12-12-22-1Document14 pagesTIS REV5 BRAINFARMA Brasile 1-055-12-12-22-1AndreaNo ratings yet
- A Study of How Lighting Can Affect A Guests Dining ExperienceDocument133 pagesA Study of How Lighting Can Affect A Guests Dining ExperiencehattyuuNo ratings yet
- Art For Animals: J. Keri CroninDocument44 pagesArt For Animals: J. Keri CroninDill an' SebastianNo ratings yet
- Fixture For Centering Connecting RodDocument2 pagesFixture For Centering Connecting Rodarie prasetyaNo ratings yet
- Ultimate Goals of LifeDocument11 pagesUltimate Goals of LifeDaniel C. DequiñaNo ratings yet