Download as pdf or txt
You might also like
- Pelvic MassesDocument15 pagesPelvic MassesJulia kwapeNo ratings yet
- Appendicectomy Step by Step PDFDocument9 pagesAppendicectomy Step by Step PDFOlugbenga A Adetunji100% (1)
- Double-V-Weld Consumption Formula in Excel SheetDocument6 pagesDouble-V-Weld Consumption Formula in Excel SheetvinothNo ratings yet
- Lesson 2 - Determining The Progress Towards The Attainment of Learning OutcomesDocument89 pagesLesson 2 - Determining The Progress Towards The Attainment of Learning OutcomesDiana HernandezNo ratings yet
- Aetiology, Pathology and Management of Enterocutaneous FistulaDocument34 pagesAetiology, Pathology and Management of Enterocutaneous Fistularoselinekhadija100% (2)
- Anorectal MalformationDocument40 pagesAnorectal Malformationblessy83% (18)
- 1 CervixDocument12 pages1 Cervixzianab aliNo ratings yet
- Surana & Surana National Trial Advocacy Moot & Judgment Writing Competition 2016 - NorthDocument20 pagesSurana & Surana National Trial Advocacy Moot & Judgment Writing Competition 2016 - Northakshi100% (1)
- General Safety Orientation Guidelines (Replaced Irp 16)Document29 pagesGeneral Safety Orientation Guidelines (Replaced Irp 16)dinuveraNo ratings yet
- Handbook Combined PDFDocument60 pagesHandbook Combined PDFHana Hill100% (2)
- Chua vs. CSCDocument4 pagesChua vs. CSCRaya Alvarez Teston100% (1)
- LaprosDocument23 pagesLaproshacker ammerNo ratings yet
- Surgical Treatment: Shany Schwarzwald s1711 DR Cojocaru CristinaDocument12 pagesSurgical Treatment: Shany Schwarzwald s1711 DR Cojocaru CristinaShany SchwarzwaldNo ratings yet
- Appendix Part 2Document7 pagesAppendix Part 2Abdullah EssaNo ratings yet
- ParacentesisDocument18 pagesParacentesistsnim saadNo ratings yet
- Surgical Treatment ShanyDocument13 pagesSurgical Treatment ShanyShany SchwarzwaldNo ratings yet
- Symptomatology of GUT DisordersDocument75 pagesSymptomatology of GUT DisordersMaraJoRNNo ratings yet
- K-25 Acute AppendicitisDocument23 pagesK-25 Acute AppendicitiscarinasheliapNo ratings yet
- AppendicitisDocument25 pagesAppendicitisshahadelkanzi56No ratings yet
- Complications of Laparoscopic SurgeriesDocument40 pagesComplications of Laparoscopic Surgeriesrajan kumar100% (10)
- Instrumentations: Presented byDocument27 pagesInstrumentations: Presented byOmar AhmedNo ratings yet
- Pancreatic PseudocystDocument16 pagesPancreatic PseudocystSpandan KadamNo ratings yet
- Iatrogenic Rectal InjuryDocument45 pagesIatrogenic Rectal InjuryThananthron PhakharatkunNo ratings yet
- Suprapubic CatheterizationDocument34 pagesSuprapubic CatheterizationalfiNo ratings yet
- 2 Semester 1 Major Patho AnatoDocument49 pages2 Semester 1 Major Patho AnatoManushi HenadeeraNo ratings yet
- Surgical Management of Benign Causes of Obstructive JaundiceDocument29 pagesSurgical Management of Benign Causes of Obstructive JaundiceNaviNo ratings yet
- SURGERY MedicalDocument15 pagesSURGERY MedicalSNo ratings yet
- Gynecological LaparosDocument32 pagesGynecological LaparosYosef Dwi Cahyadi Salan100% (1)
- Background - Docx PrintDocument8 pagesBackground - Docx PrintMarjorie Joy DanzilNo ratings yet
- Vaginal FistulaDocument14 pagesVaginal FistulaNainesh RavaliyaNo ratings yet
- Laparoscopy: Shenillee Burgess Reyad HoseinDocument31 pagesLaparoscopy: Shenillee Burgess Reyad HoseinShenillee BurgessNo ratings yet
- Indications: PeritonitisDocument8 pagesIndications: PeritonitisIrene Soriano BayubayNo ratings yet
- Visayas Community Medical Center Department of Surgery: Curan, Jan Kleen Ediza, Janseen Tortugo, Andrea MarieDocument43 pagesVisayas Community Medical Center Department of Surgery: Curan, Jan Kleen Ediza, Janseen Tortugo, Andrea MarieJanseen EdizaNo ratings yet
- FluorosDocument47 pagesFluorossinculpachillanNo ratings yet
- Ventral Hernia CaseDocument63 pagesVentral Hernia CaseROUNAK MEHROTRANo ratings yet
- Exp LapDocument9 pagesExp LapShreeja SajitNo ratings yet
- Screenshot 2023-11-26 at 5.15.31 PMDocument39 pagesScreenshot 2023-11-26 at 5.15.31 PMgauravsingh708284No ratings yet
- Injury To The Colon and RectumDocument40 pagesInjury To The Colon and RectumLilibeth Tenorio De LeonNo ratings yet
- 55 Endoscopy in Obstetric and GynaecologyDocument65 pages55 Endoscopy in Obstetric and GynaecologycollinsmagNo ratings yet
- Scrotal Swelling FadhlyDocument52 pagesScrotal Swelling FadhlyfadhlyNo ratings yet
- Vesico Vaginal FistulaDocument6 pagesVesico Vaginal Fistulaapi-3705046No ratings yet
- VVF Clinical Presentation 1Document24 pagesVVF Clinical Presentation 1georgeloto12No ratings yet
- Dilatation & Curettage: DR Ayswarya NarayanDocument19 pagesDilatation & Curettage: DR Ayswarya NarayanPrajwal Kp0% (1)
- Scrotal SwellingDocument40 pagesScrotal Swellingeirene simbolonNo ratings yet
- Imperforate AnusDocument52 pagesImperforate Anushayssam rashwan100% (6)
- Diseses of Large IntestineDocument24 pagesDiseses of Large Intestineaastharawat1234No ratings yet
- Management of Urological FistulaeDocument31 pagesManagement of Urological FistulaeBrendan DiasNo ratings yet
- Female ReproductiveDocument13 pagesFemale Reproductiveta CNo ratings yet
- LaparotomyDocument36 pagesLaparotomydenekeNo ratings yet
- Paediatric Surgery Exit Test 2022Document11 pagesPaediatric Surgery Exit Test 2022ferdosjm74No ratings yet
- 2 2017 03 26!08 03 00 PMDocument10 pages2 2017 03 26!08 03 00 PManakayamNo ratings yet
- Small Intestine and ColonDocument9 pagesSmall Intestine and Colonlentini@maltanet.netNo ratings yet
- Diverticular Disease: Maj Mohit Goyal Maj Rahul Goel Dept of SurgeryDocument67 pagesDiverticular Disease: Maj Mohit Goyal Maj Rahul Goel Dept of Surgeryunknownsince1986No ratings yet
- Hirschprung DiseaseDocument61 pagesHirschprung DiseaseAdditi Satyal100% (1)
- Explor LaparotomyDocument14 pagesExplor LaparotomyGracia NievesNo ratings yet
- LaparosDocument31 pagesLaparosAnuradha RoopchandNo ratings yet
- Anatomy and Blood Supply of AppendixDocument30 pagesAnatomy and Blood Supply of AppendixForam PatelNo ratings yet
- VVF Clinical Presentation 1Document24 pagesVVF Clinical Presentation 1api-370504686% (7)
- Paediatric Surgery 2Document38 pagesPaediatric Surgery 2عمار عارفNo ratings yet
- Diseases of Rectum and Anal CanalDocument68 pagesDiseases of Rectum and Anal CanalKoridor Falua Sakti Halawa 21000063No ratings yet
- Common Gynecologic ProceduresDocument55 pagesCommon Gynecologic ProceduresQurrataini IbanezNo ratings yet
- Analrectal Conditions and Managements: Presenter Dr. Gilbert SangaDocument63 pagesAnalrectal Conditions and Managements: Presenter Dr. Gilbert SangaSamar AhmadNo ratings yet
- Genital FistulaeDocument27 pagesGenital Fistulaeapi-3705046100% (1)
- Sigmoid Volvulus (Autosaved)Document34 pagesSigmoid Volvulus (Autosaved)msichiliinnocent7No ratings yet
- Female SterilisationDocument29 pagesFemale SterilisationWilliams Emmanuel AdeyeyeNo ratings yet
- Contraception Part1Document38 pagesContraception Part1zianab aliNo ratings yet
- Polycystic Ovarian SyndromeDocument11 pagesPolycystic Ovarian Syndromezianab aliNo ratings yet
- Operative ProcedureDocument22 pagesOperative Procedurezianab aliNo ratings yet
- Female Genital Tract Anatomy 5th YearDocument12 pagesFemale Genital Tract Anatomy 5th Yearzianab aliNo ratings yet
- Contraception: Heidery - Class DR. Hanaa Al 5 GynaecologyDocument11 pagesContraception: Heidery - Class DR. Hanaa Al 5 Gynaecologyzianab aliNo ratings yet
- Primary and Secondary Anenorrhea 2016-2017Document24 pagesPrimary and Secondary Anenorrhea 2016-2017zianab ali100% (1)
- Physiology of The Menstrual CycleDocument17 pagesPhysiology of The Menstrual Cyclezianab aliNo ratings yet
- MiscarriageDocument38 pagesMiscarriagezianab aliNo ratings yet
- Recurrent Miscarriage - Pregnancy LossDocument34 pagesRecurrent Miscarriage - Pregnancy Losszianab aliNo ratings yet
- Corporeal Fantasy - The Algebra of Life (Gurdjieff Influenced)Document5 pagesCorporeal Fantasy - The Algebra of Life (Gurdjieff Influenced)Kenneth AndersonNo ratings yet
- Notes On How To Fill in The Medical Certificate of Cause of DeathDocument10 pagesNotes On How To Fill in The Medical Certificate of Cause of DeathSayantan BanerjeeNo ratings yet
- Nordac SK 750E: Manual For Frequency InvertersDocument157 pagesNordac SK 750E: Manual For Frequency InvertersjorgeNo ratings yet
- Instant Download Psychological Science Modeling Scientific Literacy 1st Edition Krause Test Bank PDF Full ChapterDocument32 pagesInstant Download Psychological Science Modeling Scientific Literacy 1st Edition Krause Test Bank PDF Full ChapterAdrianSmitheqim100% (9)
- Syllabus - MCH Course 2019 FINAL 1 1Document8 pagesSyllabus - MCH Course 2019 FINAL 1 1Nur Fatima SanaaniNo ratings yet
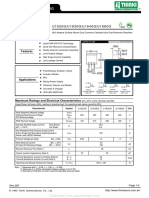
- U1620G Thru U1660G: U1620G/U1630G/U1640G/U1660GDocument2 pagesU1620G Thru U1660G: U1620G/U1630G/U1640G/U1660GTeles SilvaNo ratings yet
- DC 1 5dDocument18 pagesDC 1 5dSymon Miranda SiosonNo ratings yet
- 014EBM Degracia DB EtallDocument17 pages014EBM Degracia DB EtallMarinel Piol MarasiganNo ratings yet
- 09-22-2021 Original Complaint by Austin ISD Against District Over Covid-19 PoliciesDocument278 pages09-22-2021 Original Complaint by Austin ISD Against District Over Covid-19 PoliciesCBS Austin WebteamNo ratings yet
- Human Resource Management 13Th Global Edition by R Wayne Mondy Full ChapterDocument41 pagesHuman Resource Management 13Th Global Edition by R Wayne Mondy Full Chapterhelen.bolden534100% (25)
- Kansal Diebetes and BiochemicsDocument144 pagesKansal Diebetes and BiochemicsAhmad KhanNo ratings yet
- Basf Ucrete Ud200 TdsDocument2 pagesBasf Ucrete Ud200 TdsBagus Deddy AndriNo ratings yet
- Section-1: Drilling Fluids CriteriaDocument8 pagesSection-1: Drilling Fluids CriteriaMohamed AbozeimaNo ratings yet
- TN 09.30 02 2001 Clearance of DU Hazards V.10 Amd 1 01 PDFDocument18 pagesTN 09.30 02 2001 Clearance of DU Hazards V.10 Amd 1 01 PDFKhaledMadridiNo ratings yet
- Augmentin DdsDocument12 pagesAugmentin DdsQureshi imtiyazNo ratings yet
- Respicio Group2 MarketingPlan ABM12-3PDocument34 pagesRespicio Group2 MarketingPlan ABM12-3PChristine RespicioNo ratings yet
- Transformer Overexcitation Protection-RALK: ABB India Utilities - Automation Juliana/K Tickoo 1Document17 pagesTransformer Overexcitation Protection-RALK: ABB India Utilities - Automation Juliana/K Tickoo 1santoshkumarNo ratings yet
- Satisfaction With Job Security As A Predictor of Organizational Commitment and Job Performance in A Multicultural EnvironmentDocument11 pagesSatisfaction With Job Security As A Predictor of Organizational Commitment and Job Performance in A Multicultural EnvironmentEffeNo ratings yet
- 2010 Single Phase Padmount TransformerDocument9 pages2010 Single Phase Padmount TransformerRick DownerNo ratings yet
- Estimation of Nursing Staff Requirment Active Analysis and Various Research StudiesDocument17 pagesEstimation of Nursing Staff Requirment Active Analysis and Various Research StudiesmOHAN.S100% (3)
- Sh300 Owner's ManualDocument142 pagesSh300 Owner's ManualMakalukiNo ratings yet
- Regla de Ergonomía 1Document15 pagesRegla de Ergonomía 1Valeria RincónNo ratings yet
- Specification Chart of Pipes - Stainless Steel - Seamless Pipe - Mild Steel - Hollow SteelDocument5 pagesSpecification Chart of Pipes - Stainless Steel - Seamless Pipe - Mild Steel - Hollow SteelSarita BoteNo ratings yet
- Orion 920DX UkDocument2 pagesOrion 920DX UkVinícius Leite BandeiraNo ratings yet