Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5824)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- In The Womb Movie QuestionsDocument1 pageIn The Womb Movie Questionsapi-376200062No ratings yet
- Journal Uro 3Document5 pagesJournal Uro 3Gladys AilingNo ratings yet
- Journal Uro 1Document15 pagesJournal Uro 1Gladys AilingNo ratings yet
- JOurnal Uro 2Document6 pagesJOurnal Uro 2Gladys AilingNo ratings yet
- 13 Rasha GomaaDocument14 pages13 Rasha GomaaGladys AilingNo ratings yet
- Pelvic Floor Physical Therapy in The Treatment of Pelvic Floor Dysfunction in WomenDocument9 pagesPelvic Floor Physical Therapy in The Treatment of Pelvic Floor Dysfunction in WomenGladys Ailing100% (1)
- Massage PerineumDocument13 pagesMassage PerineumGladys AilingNo ratings yet
- Discussion: ST Elevation Myocardial Infarction (Stemi)Document33 pagesDiscussion: ST Elevation Myocardial Infarction (Stemi)Gladys AilingNo ratings yet
- Stem Cell TechnologyDocument23 pagesStem Cell TechnologyGladys AilingNo ratings yet
- Definition of Cell CultureDocument36 pagesDefinition of Cell CultureGladys AilingNo ratings yet
- John Zakour - A Man's Guide To PregnancyDocument58 pagesJohn Zakour - A Man's Guide To Pregnancyatan_rizal100% (1)
- Cleft Lip PalateDocument54 pagesCleft Lip PalateGladys AilingNo ratings yet
- Obgyn Guidelines HypertensionDocument20 pagesObgyn Guidelines HypertensionGladys AilingNo ratings yet
- Activity 1: Jevelav G. Tahadlangit BSCE-1A Oct. 22, 2020Document10 pagesActivity 1: Jevelav G. Tahadlangit BSCE-1A Oct. 22, 2020RJ TacataNo ratings yet
- Confined Space Operations: Corporate Safety TrainingDocument124 pagesConfined Space Operations: Corporate Safety Trainingreda mesbahNo ratings yet
- HeirarchyDocument3 pagesHeirarchyMazikeen LilimNo ratings yet
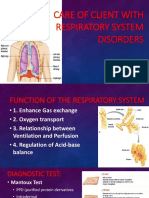
- Care of Client With Respiratory System DisordersDocument17 pagesCare of Client With Respiratory System DisordersAYTONA, JAMAICA F.No ratings yet
- Psychosocial Narrative ReportDocument2 pagesPsychosocial Narrative ReportChonnie TiaNo ratings yet
- 2017 02 - SHRM-SIOP Employee Well-BeingDocument21 pages2017 02 - SHRM-SIOP Employee Well-BeingibaumyNo ratings yet
- Divine River ChurchDocument5 pagesDivine River ChurchBrian MatovuNo ratings yet
- Risk For Falls NCPDocument1 pageRisk For Falls NCPandayaannedhesireeNo ratings yet
- EnglishDocument10 pagesEnglishDaniel RoyNo ratings yet
- Sodio OralDocument6 pagesSodio OralBoris QuelcaNo ratings yet
- Service Stream EDP Permit Training Participant WorkbookDocument19 pagesService Stream EDP Permit Training Participant Workbookshana.mxNo ratings yet
- Week 7 Guide Questions AnswersDocument7 pagesWeek 7 Guide Questions AnswersKathleenMarieAlforteNo ratings yet
- Nilai NormalDocument5 pagesNilai NormalAgya Ghilman FazaNo ratings yet
- Domestic ViolenceDocument28 pagesDomestic ViolencesyedhasnainrazanustNo ratings yet
- Nursing Care Plan 5 Altered Nutrition: Less Than Body RequirementsDocument9 pagesNursing Care Plan 5 Altered Nutrition: Less Than Body Requirementsdbryant010183% (24)
- OBSTETRIC NURSING Hand Out UPANG INHOUSE 2022Document7 pagesOBSTETRIC NURSING Hand Out UPANG INHOUSE 2022Mary Ann G. CorsanesNo ratings yet
- NIDA Clinical Trials Network Drug Abuse Screening Test (DAST-10)Document2 pagesNIDA Clinical Trials Network Drug Abuse Screening Test (DAST-10)deniNo ratings yet
- REVIEWERDocument52 pagesREVIEWERSai TrishiaNo ratings yet
- Environmental Controls in Operating Theatres: S. Dharan and D. PittetDocument6 pagesEnvironmental Controls in Operating Theatres: S. Dharan and D. PittetDinda FSNo ratings yet
- Degree of Axis Correction in Valgus High Tibial OsteotomyDocument9 pagesDegree of Axis Correction in Valgus High Tibial Osteotomy洪侊增No ratings yet
- International Economics 7th Edition Gerber Test BankDocument36 pagesInternational Economics 7th Edition Gerber Test Bankphillipsantosdod5is100% (26)
- The Versatility of Flowable Composites. Part 2 - Clinical UsesDocument4 pagesThe Versatility of Flowable Composites. Part 2 - Clinical UsesMohammad Abdulmon’emNo ratings yet
- Quarter: Week: Melc: (S10Mt-Icc-D-22) - Day Objectives Topics Classroom-Based ActivitiesDocument5 pagesQuarter: Week: Melc: (S10Mt-Icc-D-22) - Day Objectives Topics Classroom-Based ActivitiesCamille ManaloNo ratings yet
- نسخة Assignment of PsychologyDocument3 pagesنسخة Assignment of Psychologyموم الحربيNo ratings yet
- 7.artikel JKM Vol. 14 No. 2 Desember 2021 Case Report JKM Edwin Anto Pakpahan 55 63Document9 pages7.artikel JKM Vol. 14 No. 2 Desember 2021 Case Report JKM Edwin Anto Pakpahan 55 63waode apriyaniNo ratings yet
- Medical Scenarios Updated 2023Document87 pagesMedical Scenarios Updated 2023tato sernaNo ratings yet
- 2023 GKS-U Application FormsDocument11 pages2023 GKS-U Application FormsNaomi FernándezNo ratings yet
- Intro To Social WorkDocument35 pagesIntro To Social WorkJane April CalanaoNo ratings yet
- Curs 11.3 ADKDocument33 pagesCurs 11.3 ADKBrînzǎ Maria-CristinaNo ratings yet