Download as pdf or txt
You might also like
- Stretching 35 Exercises To Improve Flexibility and Reduce Pain Harvard Health 3Document41 pagesStretching 35 Exercises To Improve Flexibility and Reduce Pain Harvard Health 3Pan90% (10)
- Epistemic Beliefs InventoryDocument4 pagesEpistemic Beliefs InventoryAlberto RojasNo ratings yet
- El Khoury2018Document3 pagesEl Khoury2018peroksidaseNo ratings yet
- Treatment of Giant Prostatic Urethral Stone W 2024 International Journal ofDocument5 pagesTreatment of Giant Prostatic Urethral Stone W 2024 International Journal ofRonald QuezadaNo ratings yet
- International Archives of Urology and Complications Iauc 3 024Document9 pagesInternational Archives of Urology and Complications Iauc 3 024Anonymous 2ernTkNo ratings yet
- Crim Urology2013-932529Document3 pagesCrim Urology2013-932529TheQueensafa90No ratings yet
- Unilateral Complete Ureteral Duplication With Distal Ureteral Stone: A Rare EntityDocument2 pagesUnilateral Complete Ureteral Duplication With Distal Ureteral Stone: A Rare EntityperoksidaseNo ratings yet
- A Case of Urethrocutaneous Fistula A Forgotten Segment of A Broken UrethralDocument3 pagesA Case of Urethrocutaneous Fistula A Forgotten Segment of A Broken UrethralWardah Fauziah El SofwanNo ratings yet
- Ijrms-12417 CDocument5 pagesIjrms-12417 CSamuel MedinaNo ratings yet
- Managing Ureterocoele in A Teenage GirlDocument6 pagesManaging Ureterocoele in A Teenage GirlAnab Rehan TaseerNo ratings yet
- Tips and Tricks in Laparoscopic Ureterolithotomy For Large Ureteric Stones About 8 CasesDocument4 pagesTips and Tricks in Laparoscopic Ureterolithotomy For Large Ureteric Stones About 8 CasesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Complex Case of Ureteropelvic Junction Obstruction 2024 International JournaDocument3 pagesComplex Case of Ureteropelvic Junction Obstruction 2024 International JournaRonald QuezadaNo ratings yet
- Case Report of Ectopic Hepatic Tissue, A Rare Finding DuringDocument4 pagesCase Report of Ectopic Hepatic Tissue, A Rare Finding DuringAnila CakeNo ratings yet
- Giant SlidingDocument5 pagesGiant Slidingcarlos.alberto.palacios.serratNo ratings yet
- Pi Is 2210261215001479Document3 pagesPi Is 2210261215001479hussein_faourNo ratings yet
- TMP CD3Document4 pagesTMP CD3FrontiersNo ratings yet
- La Importancia de La Urografía Por TC en El Diagnóstico Precoz de Variaciones Anatómicas Del Tracto Urogenital Presentación de CasoDocument5 pagesLa Importancia de La Urografía Por TC en El Diagnóstico Precoz de Variaciones Anatómicas Del Tracto Urogenital Presentación de Casojose luis ramirez espinosaNo ratings yet
- Acute Onset of Renal Colic From Bilateral Ureterolithiasis: A Case ReportDocument4 pagesAcute Onset of Renal Colic From Bilateral Ureterolithiasis: A Case ReportMarcelitaTaliaDuwiriNo ratings yet
- Preprint Not Peer Reviewed: AuthorsDocument7 pagesPreprint Not Peer Reviewed: AuthorsАмина ПлотноваNo ratings yet
- Inguinal Ureter Herniation Evaluated With Magnetic Resonance Imaging: A Case ReportDocument3 pagesInguinal Ureter Herniation Evaluated With Magnetic Resonance Imaging: A Case ReportPutriNo ratings yet
- Cats With Circumcaval UretersDocument8 pagesCats With Circumcaval UretersDaniel CapuchoNo ratings yet
- Subsidence of Hypertension in A Patient With GiantDocument4 pagesSubsidence of Hypertension in A Patient With GiantSinbijeo GinNo ratings yet
- Integrated Management of Urinary Disease: StoneDocument1 pageIntegrated Management of Urinary Disease: StoneGus Indra SudewaNo ratings yet
- Case Report Severe Dysplasia of Kidney 20082021Document15 pagesCase Report Severe Dysplasia of Kidney 20082021Nikko Caesario Mauldy SusiloNo ratings yet
- Case 9582 Perinephric Fluid in Acute Ureterolithiasis: Clinical HistoryDocument8 pagesCase 9582 Perinephric Fluid in Acute Ureterolithiasis: Clinical Historygrahapuspa17No ratings yet
- HydronephrosisDocument3 pagesHydronephrosisCarla AlmerolNo ratings yet
- (Final Edit) Ventral Onlay Buccal Graft For Urethrorectal FistulaDocument13 pages(Final Edit) Ventral Onlay Buccal Graft For Urethrorectal FistulaNadia Rezky ElizaNo ratings yet
- International Archives of Urology and Complications Iauc 8 086Document6 pagesInternational Archives of Urology and Complications Iauc 8 086Ikhsan PrialaksanaNo ratings yet
- A Novel Technique For Treatment of Distal Ureteral Calculi: Early ResultsDocument4 pagesA Novel Technique For Treatment of Distal Ureteral Calculi: Early ResultsTheQueensafa90No ratings yet
- Todani IVDocument3 pagesTodani IVJoshua Patrick MuljadiNo ratings yet
- Cureus 0012 00000011460Document6 pagesCureus 0012 00000011460AlixNo ratings yet
- URL in A Case of AdultNeglected Case of Bladder ExstrophyDocument2 pagesURL in A Case of AdultNeglected Case of Bladder ExstrophyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Giants Bladder Stones With Acute Renal Failure in Patient With A Undiagnosed Neurological Bladder Due To A Spinal Cord Injury: Uncommon CaseDocument4 pagesGiants Bladder Stones With Acute Renal Failure in Patient With A Undiagnosed Neurological Bladder Due To A Spinal Cord Injury: Uncommon CaseIJAR JOURNALNo ratings yet
- Aloi IP, Lais A, Caione P. Bladder Injuries Following Inguinal Canal Surgery in Infants. Pediatr Surg Int 2010Document4 pagesAloi IP, Lais A, Caione P. Bladder Injuries Following Inguinal Canal Surgery in Infants. Pediatr Surg Int 2010Oscar Sanchez ParisNo ratings yet
- Borges Dias 2016Document2 pagesBorges Dias 2016Fandi AhmadNo ratings yet
- Sistem Tunggal Ureter Ektopik Dengan Ginjal Multikistik Displastik Di RSUP Sanglah, Bali, Indonesia: Laporan KasusDocument5 pagesSistem Tunggal Ureter Ektopik Dengan Ginjal Multikistik Displastik Di RSUP Sanglah, Bali, Indonesia: Laporan KasusRahma AmaliaNo ratings yet
- Urology Case Reports: S. Palthe, G.A. Dijkstra, M.G. SteffensDocument3 pagesUrology Case Reports: S. Palthe, G.A. Dijkstra, M.G. SteffensFloro Dave ArnucoNo ratings yet
- Duplication of Gallbladder: Case ReportDocument3 pagesDuplication of Gallbladder: Case ReportVenanda RianNo ratings yet
- Adam 2017Document4 pagesAdam 2017Bandac AlexandraNo ratings yet
- A Case Report On Biliary Ileus As A Rare Trigger For Intestinal ObstructionDocument7 pagesA Case Report On Biliary Ileus As A Rare Trigger For Intestinal ObstructionIJAR JOURNALNo ratings yet
- Should Ureteroscopy Be Considered As The First Choice For Proximal Ureter Stones of Children?Document6 pagesShould Ureteroscopy Be Considered As The First Choice For Proximal Ureter Stones of Children?TheQueensafa90No ratings yet
- A Brief Case Report of Duplicated Bladder Exstrophy A Congenital Malformation in PaediatricsDocument3 pagesA Brief Case Report of Duplicated Bladder Exstrophy A Congenital Malformation in PaediatricsMARIA SOL MONTALVO LALALEONo ratings yet
- 29580-Article Text-55601-1-10-20190129Document5 pages29580-Article Text-55601-1-10-20190129Octavia SohanggrainyNo ratings yet
- Measure BUN Creat Urine LeakageDocument4 pagesMeasure BUN Creat Urine Leakagerendi wibowoNo ratings yet
- Clinical Note: Ureteral Triplication Without Other Associated MalformationsDocument4 pagesClinical Note: Ureteral Triplication Without Other Associated MalformationsA DNo ratings yet
- Urological Science: Jiun-Hung Geng, Chun-Nung HuangDocument4 pagesUrological Science: Jiun-Hung Geng, Chun-Nung Huangyerich septaNo ratings yet
- Giant Bladder Stone: A Case Report and Review of The LiteratureDocument3 pagesGiant Bladder Stone: A Case Report and Review of The LiteratureElviera Is MayaraniNo ratings yet
- Chronic Myeloid Leukemia Presenting With Priapism: A Case ReportDocument4 pagesChronic Myeloid Leukemia Presenting With Priapism: A Case ReportJulio LeviNo ratings yet
- Surgical Management of Urolithiasis in Dog Along With Peritoneal Dialysis: 12 CasesDocument10 pagesSurgical Management of Urolithiasis in Dog Along With Peritoneal Dialysis: 12 CasesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Hanging Bladder Calculi Secondary To Misplaced Surgical SutureDocument3 pagesHanging Bladder Calculi Secondary To Misplaced Surgical SutureChato Haviz DanayomiNo ratings yet
- The Kaohsiung J of Med Scie - 2008 - Akg L - Penile Crural Injury Due To Perineal Penetrating Trauma A Case ReportDocument3 pagesThe Kaohsiung J of Med Scie - 2008 - Akg L - Penile Crural Injury Due To Perineal Penetrating Trauma A Case Reportkiran rayan euNo ratings yet
- Sciencedirect: Radiology Case Reports 11 (2016) 328 E331Document7 pagesSciencedirect: Radiology Case Reports 11 (2016) 328 E331Novia FaizatiwahidaNo ratings yet
- Ureterostomia CutanataDocument5 pagesUreterostomia Cutanatadiana.miron.mNo ratings yet
- 1 s2.0 S0022480423002895 MainDocument7 pages1 s2.0 S0022480423002895 Mainlucabarbato23No ratings yet
- Minimal Renal Pelvis DilationDocument8 pagesMinimal Renal Pelvis DilationdpcamposhNo ratings yet
- Laparoscopic Cholecystectomy After Conservative Su - 2024 - International JournaDocument4 pagesLaparoscopic Cholecystectomy After Conservative Su - 2024 - International JournaRonald QuezadaNo ratings yet
- A Case Report Clinical Manifestation of Covid19 in Pediatric and Its Management in Remote AreaDocument1 pageA Case Report Clinical Manifestation of Covid19 in Pediatric and Its Management in Remote AreaLitha LakeNo ratings yet
- Jurnal Cysto 2Document4 pagesJurnal Cysto 2Jihan MochiNo ratings yet
- Subhepatic Appendix: An Ectopic Topography Not To Be Disregarded: A Case ReportDocument4 pagesSubhepatic Appendix: An Ectopic Topography Not To Be Disregarded: A Case ReportPawan MishraNo ratings yet
- Case Report: Saudi Journal of Kidney Diseases and TransplantationDocument0 pagesCase Report: Saudi Journal of Kidney Diseases and TransplantationIrma Suriani DarwisNo ratings yet
- Case Report: Giant Preputial Calculus: The First Reported Case in MalaysiaDocument4 pagesCase Report: Giant Preputial Calculus: The First Reported Case in MalaysiadmpmppNo ratings yet
- Post-cholecystectomy Bile Duct InjuryFrom EverandPost-cholecystectomy Bile Duct InjuryVinay K. KapoorNo ratings yet
- Transurethral Incision of Ureterocele: Does The Time of Presentation Affect The Need For Further Surgical Interventions?Document6 pagesTransurethral Incision of Ureterocele: Does The Time of Presentation Affect The Need For Further Surgical Interventions?ErikNo ratings yet
- Active Surveillance For Antenatally Detected Ureteroceles: Predictors of SuccessDocument6 pagesActive Surveillance For Antenatally Detected Ureteroceles: Predictors of SuccessErikNo ratings yet
- Criterios Bradford-Hill PDFDocument3 pagesCriterios Bradford-Hill PDFErikNo ratings yet
- Criterios Bradford-HillDocument3 pagesCriterios Bradford-HillErikNo ratings yet
- Sag-Cookery NC Ii PDFDocument6 pagesSag-Cookery NC Ii PDFArayaskillsdevt InstitutecorpNo ratings yet
- Air Cooler Cleaner (Acc) Is A Liquid Blend of Highly Active CleaningDocument5 pagesAir Cooler Cleaner (Acc) Is A Liquid Blend of Highly Active CleaningAbdul AnisNo ratings yet
- Enum - Singleton Pattern - InstanceOfDocument18 pagesEnum - Singleton Pattern - InstanceOfadarsh rajNo ratings yet
- TSPSC Vro Vra Exam Pattern 2017Document7 pagesTSPSC Vro Vra Exam Pattern 2017Sk HarrshadNo ratings yet
- RapidprototypingDocument27 pagesRapidprototypingThirumalaimuthukumaranMohanNo ratings yet
- Nfhs-5 India ReportDocument713 pagesNfhs-5 India ReportROHIT DASNo ratings yet
- Advanced Data Research PaperDocument6 pagesAdvanced Data Research Papersaurabh20apr100% (1)
- English NotesDocument16 pagesEnglish NotesNerin MichaelNo ratings yet
- Updated UHVPE Unit II Notes PDFDocument28 pagesUpdated UHVPE Unit II Notes PDFAditya SrivastavaNo ratings yet
- 11 - John Laurents - Pavemetrics - 3D Transverse Road ProfilingDocument74 pages11 - John Laurents - Pavemetrics - 3D Transverse Road ProfilingOrlando Rojas100% (1)
- Understanding Supply Chain ManagementDocument58 pagesUnderstanding Supply Chain Managementrl magsinoNo ratings yet
- The Abcs of Technical WritingDocument30 pagesThe Abcs of Technical WritingMayeng's VlogNo ratings yet
- Medsurg Careplan 3Document10 pagesMedsurg Careplan 3api-520874306No ratings yet
- Tubos de CalorDocument7 pagesTubos de CalorChristo AcostaNo ratings yet
- How To Restore Market Confidence in The NCM 150412Document7 pagesHow To Restore Market Confidence in The NCM 150412ProshareNo ratings yet
- 2 Ethico-legal-POWERPOINT-BASIC As of January 12, 2009 (1) .Document81 pages2 Ethico-legal-POWERPOINT-BASIC As of January 12, 2009 (1) .Crystal Mae Castrodes Daquipil100% (1)
- Causes and Prevention of Common Diseases Abd Epidemics in Human Epidemics, Pandemics, and OutbreaksDocument4 pagesCauses and Prevention of Common Diseases Abd Epidemics in Human Epidemics, Pandemics, and OutbreaksFaisal AwanNo ratings yet
- Test Bank For Management 10th Edition Ricky W GriffinDocument34 pagesTest Bank For Management 10th Edition Ricky W Griffinreordervarianceygdn100% (53)
- Seven Refractories Aluminio PDFDocument15 pagesSeven Refractories Aluminio PDFjose.figueroa@foseco.comNo ratings yet
- Julia Dault: Born 1977, Toronto Lives and Works in New YorkDocument4 pagesJulia Dault: Born 1977, Toronto Lives and Works in New YorkUn BigoteNo ratings yet
- mddn413 Project 3 KDC Logotype BriefDocument2 pagesmddn413 Project 3 KDC Logotype Briefapi-269292118No ratings yet
- Jared Diamond How Societies Can Grow Older BetterDocument5 pagesJared Diamond How Societies Can Grow Older BetterMariana Casals100% (1)
- Hubungan Indeks Massa Tubuh Dengan Siklus Menstruasi Pada Siswi SMP Wahid Hasyim Kota MalangDocument13 pagesHubungan Indeks Massa Tubuh Dengan Siklus Menstruasi Pada Siswi SMP Wahid Hasyim Kota MalangRoslince Umbu patiNo ratings yet
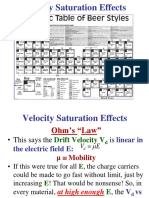
- Transport4 - High Electric Fields - Velocity SaturationDocument16 pagesTransport4 - High Electric Fields - Velocity SaturationMạnh Huy BùiNo ratings yet
- Learning EvidenceDocument5 pagesLearning EvidenceArtperture Fotografía100% (3)
- Control Units System - Ul Product Iq 4100esDocument13 pagesControl Units System - Ul Product Iq 4100escnreyes3No ratings yet
- Fundamentals of Computer NetworkDocument320 pagesFundamentals of Computer NetworkHARSH JHANo ratings yet
- Theory of Indicator BehaviourDocument12 pagesTheory of Indicator BehaviourPavoNo ratings yet