
File Book
File Book
You might also like
- Amboss NotesDocument12 pagesAmboss NotesVee Mend100% (2)
- September Recall ExportDocument1 pageSeptember Recall ExportMuhammad Abubakar100% (1)
- Differences Between Biological and Psychosocial Interventions.Document4 pagesDifferences Between Biological and Psychosocial Interventions.aval123No ratings yet
- Nighat Perveen W/O Muhammad Asghar Ali 306/A Centeral ParkDocument1 pageNighat Perveen W/O Muhammad Asghar Ali 306/A Centeral ParkusamaNo ratings yet
- Challenges in The Analysis of Adult Patients With Histories of Childhood Sexual Abuse - Glen O GabbardDocument11 pagesChallenges in The Analysis of Adult Patients With Histories of Childhood Sexual Abuse - Glen O GabbardJulián Alberto Muñoz Figueroa100% (1)
- Paediatrics MCQ PointsDocument117 pagesPaediatrics MCQ PointstharikaneelawathuraNo ratings yet
- Oleh: Pramitha Nayana L NIM 07201101032 Pembimbing: Dr. Johny Subandrio Erlan, SP - KK SMF Kulit Dan Kelamin FK Unej/RSD Dr. Soebandi JemberDocument21 pagesOleh: Pramitha Nayana L NIM 07201101032 Pembimbing: Dr. Johny Subandrio Erlan, SP - KK SMF Kulit Dan Kelamin FK Unej/RSD Dr. Soebandi JemberpramithanayaNo ratings yet
- Final Infectious Pe - 1Document49 pagesFinal Infectious Pe - 1Ahmad SobihNo ratings yet
- Neuro SGDocument29 pagesNeuro SGgew123No ratings yet
- ENT Lecture FinalDocument65 pagesENT Lecture FinalNejib M/AminNo ratings yet
- Filename: AMC PEDIATRICS 2005 To 2009 PDFDocument38 pagesFilename: AMC PEDIATRICS 2005 To 2009 PDFZahid QamarNo ratings yet
- Conradi Hünermann SyndromeDocument12 pagesConradi Hünermann Syndromejoerobinson8889323No ratings yet
- 2016 Coccidiomycosis1777978430-1Document4 pages2016 Coccidiomycosis1777978430-1nreena aslam100% (1)
- N. Meningitidis (MENINGOCOCCUS) : Meningococcemia/MeningitisDocument5 pagesN. Meningitidis (MENINGOCOCCUS) : Meningococcemia/MeningitisNestley TiongsonNo ratings yet
- OSPE Peads Medicine PDFDocument54 pagesOSPE Peads Medicine PDFKamran MallickNo ratings yet
- Peads NotesDocument18 pagesPeads Notesechofox11No ratings yet
- SyndromesDocument58 pagesSyndromesLGK maoreNo ratings yet
- Meningitis in Children 1204809002482509 3Document48 pagesMeningitis in Children 1204809002482509 3Ali FalihNo ratings yet
- ACFrOgBz6SCL6SA VJUDh46tP6NUDhw3P47 NPjiCaRlywgh9trN 5PhQeKcHqMl2xUsHtUBcc7n4mL1On5SlTP2X94BYDVb HoGkGegg5erftVOvtVci7Q4s0omLCXYn6dldjBQhk2bZ6Jpfl6cDocument24 pagesACFrOgBz6SCL6SA VJUDh46tP6NUDhw3P47 NPjiCaRlywgh9trN 5PhQeKcHqMl2xUsHtUBcc7n4mL1On5SlTP2X94BYDVb HoGkGegg5erftVOvtVci7Q4s0omLCXYn6dldjBQhk2bZ6Jpfl6cMalavika A GNo ratings yet
- 1-Ammar Notes (Med & Pedia)Document23 pages1-Ammar Notes (Med & Pedia)anmar alkhudhri100% (1)
- Final Infectious Pe - 1-EditDocument59 pagesFinal Infectious Pe - 1-EditAhmad SobihNo ratings yet
- Adrenaline (Child, Adult, IM, IV... ) Ya Corticosteroids Too Asthma Ya Croup o ..Document17 pagesAdrenaline (Child, Adult, IM, IV... ) Ya Corticosteroids Too Asthma Ya Croup o ..raji selvakumaranNo ratings yet
- Notes in Pediatrics. 2 Ed. 2001/02 Senior & Junior Peds RotationsDocument18 pagesNotes in Pediatrics. 2 Ed. 2001/02 Senior & Junior Peds Rotationsopis08100% (1)
- Aipg11 AnswersDocument175 pagesAipg11 AnswersVivek ChoukseNo ratings yet
- Edward Syndrome: Continuing Education ActivityDocument14 pagesEdward Syndrome: Continuing Education ActivitylalaaNo ratings yet
- Stevens-Johnson SyndromeDocument4 pagesStevens-Johnson SyndromeBelleNo ratings yet
- Dandy Walker MalformationDocument27 pagesDandy Walker MalformationNurul AtiqahNo ratings yet
- LymphomaDocument40 pagesLymphomaMans Fans100% (1)
- Pediatric MCQDocument17 pagesPediatric MCQAhmed Kassem100% (1)
- Meningococcal Infection (Lec4)Document8 pagesMeningococcal Infection (Lec4)Ali Al.JuffairiNo ratings yet
- Outcome Analysis of Shunt Surgery in Hydrocephalus: Riginal RticleDocument4 pagesOutcome Analysis of Shunt Surgery in Hydrocephalus: Riginal RticleiqbalNo ratings yet
- Moh RevisionDocument113 pagesMoh RevisionNeelamBadruddin67% (3)
- Management of Gradenigo Syndrome in A ChildDocument4 pagesManagement of Gradenigo Syndrome in A ChildmitaNo ratings yet
- Nclex Notes 1Document17 pagesNclex Notes 1itokumo100% (2)
- Chapter VI.17. Kawasaki Disease Kara S. Yamamoto, MD Marian E. Melish, MDDocument12 pagesChapter VI.17. Kawasaki Disease Kara S. Yamamoto, MD Marian E. Melish, MDgretch_carreonNo ratings yet
- Toacs 6Document159 pagesToacs 6Mobin Ur Rehman Khan100% (2)
- Referensi ToxoDocument37 pagesReferensi ToxoAndi IshaqNo ratings yet
- PediatricDocument32 pagesPediatricsallyNo ratings yet
- Facial Nerve PalsyDocument3 pagesFacial Nerve PalsyGayle VillarizaNo ratings yet
- Amc Pediatrics 2005 To 2009Document37 pagesAmc Pediatrics 2005 To 2009florettyNo ratings yet
- 2010 Childhood LeukaemiaDocument64 pages2010 Childhood LeukaemiaAnastasiafynnNo ratings yet
- eMRCS Pathology 326 MCQsDocument101 pageseMRCS Pathology 326 MCQsSaad KhanNo ratings yet
- Birthinjuries Dr.M.maniDocument65 pagesBirthinjuries Dr.M.manimaniNo ratings yet
- Herpes Zoster Oticus in A 12 Year Old Child and Review of Literature - A CaseDocument5 pagesHerpes Zoster Oticus in A 12 Year Old Child and Review of Literature - A CaseClodeyaRizolaNo ratings yet
- PediaDocument20 pagesPediaMedha ReddyNo ratings yet
- PediatricsDocument38 pagesPediatricskhanNo ratings yet
- Pediatric SmleDocument59 pagesPediatric SmleMoayad Zeyad M100% (1)
- Brain Abscess PDFDocument28 pagesBrain Abscess PDFdoctordilafrozaNo ratings yet
- Lymphoma: 2011-2012 Prof - Dr.Rejin Kebudi, M.DDocument57 pagesLymphoma: 2011-2012 Prof - Dr.Rejin Kebudi, M.Dmia rachmiNo ratings yet
- Clinical Diseases With Chromosomal AbnormalitiesDocument52 pagesClinical Diseases With Chromosomal AbnormalitiesAzifah ZakariaNo ratings yet
- Cerebral PalsyDocument25 pagesCerebral PalsyDr.P.NatarajanNo ratings yet
- Massa Kat 2019Document17 pagesMassa Kat 2019nayyarNo ratings yet
- Reti No Blast OmaDocument55 pagesReti No Blast OmaIndranil GhoshNo ratings yet
- Spotters AnswersDocument53 pagesSpotters AnswersParthiban RajNo ratings yet
- Eye Docs PediatricsDocument133 pagesEye Docs PediatricsMuneeb ShahzadNo ratings yet
- NocardiaDocument6 pagesNocardiadocalsultanNo ratings yet
- 2008 Article 20Document3 pages2008 Article 20tria dianaNo ratings yet
- Enarm Train Quiz AnswDocument284 pagesEnarm Train Quiz AnswanndreaoliveraNo ratings yet
- Dermatology Notes for Medical StudentsFrom EverandDermatology Notes for Medical StudentsRating: 4 out of 5 stars4/5 (5)
- Fast Facts: Blastic Plasmacytoid Dendritic Cell Neoplasm: Shedding light on a rare diseaseFrom EverandFast Facts: Blastic Plasmacytoid Dendritic Cell Neoplasm: Shedding light on a rare diseaseNo ratings yet
- Med Nov 19 NightdocxDocument21 pagesMed Nov 19 NightdocxusamaNo ratings yet
- Morning 20nov SurgeryDocument23 pagesMorning 20nov SurgeryusamaNo ratings yet
- Open Access Textbook of General SurgeryDocument7 pagesOpen Access Textbook of General SurgeryusamaNo ratings yet
- Night 20nov SurgeryDocument21 pagesNight 20nov SurgeryusamaNo ratings yet
- University of Health Sciences, Lahore: Admission Form ForDocument2 pagesUniversity of Health Sciences, Lahore: Admission Form ForusamaNo ratings yet
- Open Access Textbook of General Surgery: Shock P NavsariaDocument4 pagesOpen Access Textbook of General Surgery: Shock P NavsariausamaNo ratings yet
- Bromides Is What We NeedDocument3 pagesBromides Is What We Needusama100% (1)
- Surgery NotesDocument24 pagesSurgery NotesusamaNo ratings yet
- Open Access Textbook of General Surgery: Wound Healing G ChinneryDocument6 pagesOpen Access Textbook of General Surgery: Wound Healing G ChinneryusamaNo ratings yet
- Past PaperssssDocument231 pagesPast PaperssssusamaNo ratings yet
- 1.7 Fluids PDFDocument6 pages1.7 Fluids PDFusamaNo ratings yet
- Infectious Diseases Notes PDFDocument1 pageInfectious Diseases Notes PDFusamaNo ratings yet
- Application Form For The Post ofDocument2 pagesApplication Form For The Post ofusamaNo ratings yet
- 240519ds4043 PDFDocument1 page240519ds4043 PDFusamaNo ratings yet
- Bromides Is What We NeedDocument3 pagesBromides Is What We Needusama100% (1)
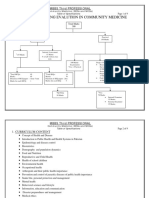
- Flow Chart Showng Evalution in Community Medicine: Mbbs Third ProfessionalDocument9 pagesFlow Chart Showng Evalution in Community Medicine: Mbbs Third ProfessionalusamaNo ratings yet
- General Pearls .TXT Version 1Document9 pagesGeneral Pearls .TXT Version 1usamaNo ratings yet
- Final English Notes B SC PDFDocument31 pagesFinal English Notes B SC PDFusamaNo ratings yet
- Visual Mnemonics For Pathology: Marbas, Laurie LDocument3 pagesVisual Mnemonics For Pathology: Marbas, Laurie LusamaNo ratings yet
- Sci Digest Circ Respir Systems v1Document36 pagesSci Digest Circ Respir Systems v1draganNo ratings yet
- OB PathophysiologyDocument2 pagesOB PathophysiologyCathy SantosNo ratings yet
- Laporan Inhouse Clinic PT SIIX 2023Document135 pagesLaporan Inhouse Clinic PT SIIX 2023Tabita SilalahiNo ratings yet
- Call For ProposalsDocument5 pagesCall For ProposalsNITHYAPREMININo ratings yet
- Surgical Gastroenterologist in ChennaiDocument2 pagesSurgical Gastroenterologist in ChennaiSrivatsan GurumurthyNo ratings yet
- Urine Collection: Collecting A Clean Catch UrineDocument5 pagesUrine Collection: Collecting A Clean Catch UrineAngelene CalivaNo ratings yet
- Suicide and Undetermined Death by DrowningDocument10 pagesSuicide and Undetermined Death by DrowningJorge GomezNo ratings yet
- Mudra VigyanDocument13 pagesMudra VigyanYeathy Raj K NaiduNo ratings yet
- Give To CMC : Email DirectoryDocument11 pagesGive To CMC : Email DirectoryDanish KhanNo ratings yet
- DR ActivityDocument2 pagesDR ActivityVia Teresa AtienzaNo ratings yet
- Patofisiologi Addison DiseaseDocument4 pagesPatofisiologi Addison DiseaseDicoGunawijayaNo ratings yet
- "Article-PDF-naresh Sharma Binita Srivastava Hind P Bhatia Arch-849Document3 pages"Article-PDF-naresh Sharma Binita Srivastava Hind P Bhatia Arch-849Ruchi ShahNo ratings yet
- 1 SMDocument6 pages1 SMedi_wsNo ratings yet
- Microbiology Nca-Cls: Terms in This SetDocument18 pagesMicrobiology Nca-Cls: Terms in This SetjustinNo ratings yet
- BHP Ethical Issue in DialysisDocument3 pagesBHP Ethical Issue in DialysisIka Mutia SilvianaNo ratings yet
- Presentation On: Kgmu College of NursingDocument42 pagesPresentation On: Kgmu College of NursingSweety YadavNo ratings yet
- Notes of 2020Document90 pagesNotes of 2020eolhc rezarf100% (1)
- Yati Soenarto - RACP AucklandDocument34 pagesYati Soenarto - RACP AucklandIntan HartandyNo ratings yet
- CABG Surgical Case Study EditeDocument18 pagesCABG Surgical Case Study Editemaduwanthaharsha88No ratings yet
- The One Minute Preceptor 5 Microskills For One-On-One Teaching PDFDocument7 pagesThe One Minute Preceptor 5 Microskills For One-On-One Teaching PDFunderwood@eject.co.zaNo ratings yet
- Contents of The CHN RLE Written RequirementsDocument4 pagesContents of The CHN RLE Written RequirementsRoshie Kaye AbalorioNo ratings yet
- CSBP Post Stroke Checklist ENDocument2 pagesCSBP Post Stroke Checklist ENEduardo BessoloNo ratings yet
- Gero Study GuideDocument42 pagesGero Study GuideAbby Schmidt100% (1)
- Bronchial AsthmaDocument39 pagesBronchial AsthmaSaeed mohamed100% (1)
- Uso Correcto de CubrebocasDocument24 pagesUso Correcto de CubrebocasMarco LeónNo ratings yet
- Assisting-in-Lumbar-Puncture Procedure GuideDocument6 pagesAssisting-in-Lumbar-Puncture Procedure GuideLeigh Chanelle OngNo ratings yet
- Rule 11DDDocument3 pagesRule 11DDIonut ColcearNo ratings yet
- REport BlooodDocument3 pagesREport Bloooddivid joneNo ratings yet











































































































Download as pdf or txt
You might also like
- Amboss NotesDocument12 pagesAmboss NotesVee Mend100% (2)
- September Recall ExportDocument1 pageSeptember Recall ExportMuhammad Abubakar100% (1)
- Differences Between Biological and Psychosocial Interventions.Document4 pagesDifferences Between Biological and Psychosocial Interventions.aval123No ratings yet
- Nighat Perveen W/O Muhammad Asghar Ali 306/A Centeral ParkDocument1 pageNighat Perveen W/O Muhammad Asghar Ali 306/A Centeral ParkusamaNo ratings yet
- Challenges in The Analysis of Adult Patients With Histories of Childhood Sexual Abuse - Glen O GabbardDocument11 pagesChallenges in The Analysis of Adult Patients With Histories of Childhood Sexual Abuse - Glen O GabbardJulián Alberto Muñoz Figueroa100% (1)
- Paediatrics MCQ PointsDocument117 pagesPaediatrics MCQ PointstharikaneelawathuraNo ratings yet
- Oleh: Pramitha Nayana L NIM 07201101032 Pembimbing: Dr. Johny Subandrio Erlan, SP - KK SMF Kulit Dan Kelamin FK Unej/RSD Dr. Soebandi JemberDocument21 pagesOleh: Pramitha Nayana L NIM 07201101032 Pembimbing: Dr. Johny Subandrio Erlan, SP - KK SMF Kulit Dan Kelamin FK Unej/RSD Dr. Soebandi JemberpramithanayaNo ratings yet
- Final Infectious Pe - 1Document49 pagesFinal Infectious Pe - 1Ahmad SobihNo ratings yet
- Neuro SGDocument29 pagesNeuro SGgew123No ratings yet
- ENT Lecture FinalDocument65 pagesENT Lecture FinalNejib M/AminNo ratings yet
- Filename: AMC PEDIATRICS 2005 To 2009 PDFDocument38 pagesFilename: AMC PEDIATRICS 2005 To 2009 PDFZahid QamarNo ratings yet
- Conradi Hünermann SyndromeDocument12 pagesConradi Hünermann Syndromejoerobinson8889323No ratings yet
- 2016 Coccidiomycosis1777978430-1Document4 pages2016 Coccidiomycosis1777978430-1nreena aslam100% (1)
- N. Meningitidis (MENINGOCOCCUS) : Meningococcemia/MeningitisDocument5 pagesN. Meningitidis (MENINGOCOCCUS) : Meningococcemia/MeningitisNestley TiongsonNo ratings yet
- OSPE Peads Medicine PDFDocument54 pagesOSPE Peads Medicine PDFKamran MallickNo ratings yet
- Peads NotesDocument18 pagesPeads Notesechofox11No ratings yet
- SyndromesDocument58 pagesSyndromesLGK maoreNo ratings yet
- Meningitis in Children 1204809002482509 3Document48 pagesMeningitis in Children 1204809002482509 3Ali FalihNo ratings yet
- ACFrOgBz6SCL6SA VJUDh46tP6NUDhw3P47 NPjiCaRlywgh9trN 5PhQeKcHqMl2xUsHtUBcc7n4mL1On5SlTP2X94BYDVb HoGkGegg5erftVOvtVci7Q4s0omLCXYn6dldjBQhk2bZ6Jpfl6cDocument24 pagesACFrOgBz6SCL6SA VJUDh46tP6NUDhw3P47 NPjiCaRlywgh9trN 5PhQeKcHqMl2xUsHtUBcc7n4mL1On5SlTP2X94BYDVb HoGkGegg5erftVOvtVci7Q4s0omLCXYn6dldjBQhk2bZ6Jpfl6cMalavika A GNo ratings yet
- 1-Ammar Notes (Med & Pedia)Document23 pages1-Ammar Notes (Med & Pedia)anmar alkhudhri100% (1)
- Final Infectious Pe - 1-EditDocument59 pagesFinal Infectious Pe - 1-EditAhmad SobihNo ratings yet
- Adrenaline (Child, Adult, IM, IV... ) Ya Corticosteroids Too Asthma Ya Croup o ..Document17 pagesAdrenaline (Child, Adult, IM, IV... ) Ya Corticosteroids Too Asthma Ya Croup o ..raji selvakumaranNo ratings yet
- Notes in Pediatrics. 2 Ed. 2001/02 Senior & Junior Peds RotationsDocument18 pagesNotes in Pediatrics. 2 Ed. 2001/02 Senior & Junior Peds Rotationsopis08100% (1)
- Aipg11 AnswersDocument175 pagesAipg11 AnswersVivek ChoukseNo ratings yet
- Edward Syndrome: Continuing Education ActivityDocument14 pagesEdward Syndrome: Continuing Education ActivitylalaaNo ratings yet
- Stevens-Johnson SyndromeDocument4 pagesStevens-Johnson SyndromeBelleNo ratings yet
- Dandy Walker MalformationDocument27 pagesDandy Walker MalformationNurul AtiqahNo ratings yet
- LymphomaDocument40 pagesLymphomaMans Fans100% (1)
- Pediatric MCQDocument17 pagesPediatric MCQAhmed Kassem100% (1)
- Meningococcal Infection (Lec4)Document8 pagesMeningococcal Infection (Lec4)Ali Al.JuffairiNo ratings yet
- Outcome Analysis of Shunt Surgery in Hydrocephalus: Riginal RticleDocument4 pagesOutcome Analysis of Shunt Surgery in Hydrocephalus: Riginal RticleiqbalNo ratings yet
- Moh RevisionDocument113 pagesMoh RevisionNeelamBadruddin67% (3)
- Management of Gradenigo Syndrome in A ChildDocument4 pagesManagement of Gradenigo Syndrome in A ChildmitaNo ratings yet
- Nclex Notes 1Document17 pagesNclex Notes 1itokumo100% (2)
- Chapter VI.17. Kawasaki Disease Kara S. Yamamoto, MD Marian E. Melish, MDDocument12 pagesChapter VI.17. Kawasaki Disease Kara S. Yamamoto, MD Marian E. Melish, MDgretch_carreonNo ratings yet
- Toacs 6Document159 pagesToacs 6Mobin Ur Rehman Khan100% (2)
- Referensi ToxoDocument37 pagesReferensi ToxoAndi IshaqNo ratings yet
- PediatricDocument32 pagesPediatricsallyNo ratings yet
- Facial Nerve PalsyDocument3 pagesFacial Nerve PalsyGayle VillarizaNo ratings yet
- Amc Pediatrics 2005 To 2009Document37 pagesAmc Pediatrics 2005 To 2009florettyNo ratings yet
- 2010 Childhood LeukaemiaDocument64 pages2010 Childhood LeukaemiaAnastasiafynnNo ratings yet
- eMRCS Pathology 326 MCQsDocument101 pageseMRCS Pathology 326 MCQsSaad KhanNo ratings yet
- Birthinjuries Dr.M.maniDocument65 pagesBirthinjuries Dr.M.manimaniNo ratings yet
- Herpes Zoster Oticus in A 12 Year Old Child and Review of Literature - A CaseDocument5 pagesHerpes Zoster Oticus in A 12 Year Old Child and Review of Literature - A CaseClodeyaRizolaNo ratings yet
- PediaDocument20 pagesPediaMedha ReddyNo ratings yet
- PediatricsDocument38 pagesPediatricskhanNo ratings yet
- Pediatric SmleDocument59 pagesPediatric SmleMoayad Zeyad M100% (1)
- Brain Abscess PDFDocument28 pagesBrain Abscess PDFdoctordilafrozaNo ratings yet
- Lymphoma: 2011-2012 Prof - Dr.Rejin Kebudi, M.DDocument57 pagesLymphoma: 2011-2012 Prof - Dr.Rejin Kebudi, M.Dmia rachmiNo ratings yet
- Clinical Diseases With Chromosomal AbnormalitiesDocument52 pagesClinical Diseases With Chromosomal AbnormalitiesAzifah ZakariaNo ratings yet
- Cerebral PalsyDocument25 pagesCerebral PalsyDr.P.NatarajanNo ratings yet
- Massa Kat 2019Document17 pagesMassa Kat 2019nayyarNo ratings yet
- Reti No Blast OmaDocument55 pagesReti No Blast OmaIndranil GhoshNo ratings yet
- Spotters AnswersDocument53 pagesSpotters AnswersParthiban RajNo ratings yet
- Eye Docs PediatricsDocument133 pagesEye Docs PediatricsMuneeb ShahzadNo ratings yet
- NocardiaDocument6 pagesNocardiadocalsultanNo ratings yet
- 2008 Article 20Document3 pages2008 Article 20tria dianaNo ratings yet
- Enarm Train Quiz AnswDocument284 pagesEnarm Train Quiz AnswanndreaoliveraNo ratings yet
- Dermatology Notes for Medical StudentsFrom EverandDermatology Notes for Medical StudentsRating: 4 out of 5 stars4/5 (5)
- Fast Facts: Blastic Plasmacytoid Dendritic Cell Neoplasm: Shedding light on a rare diseaseFrom EverandFast Facts: Blastic Plasmacytoid Dendritic Cell Neoplasm: Shedding light on a rare diseaseNo ratings yet
- Med Nov 19 NightdocxDocument21 pagesMed Nov 19 NightdocxusamaNo ratings yet
- Morning 20nov SurgeryDocument23 pagesMorning 20nov SurgeryusamaNo ratings yet
- Open Access Textbook of General SurgeryDocument7 pagesOpen Access Textbook of General SurgeryusamaNo ratings yet
- Night 20nov SurgeryDocument21 pagesNight 20nov SurgeryusamaNo ratings yet
- University of Health Sciences, Lahore: Admission Form ForDocument2 pagesUniversity of Health Sciences, Lahore: Admission Form ForusamaNo ratings yet
- Open Access Textbook of General Surgery: Shock P NavsariaDocument4 pagesOpen Access Textbook of General Surgery: Shock P NavsariausamaNo ratings yet
- Bromides Is What We NeedDocument3 pagesBromides Is What We Needusama100% (1)
- Surgery NotesDocument24 pagesSurgery NotesusamaNo ratings yet
- Open Access Textbook of General Surgery: Wound Healing G ChinneryDocument6 pagesOpen Access Textbook of General Surgery: Wound Healing G ChinneryusamaNo ratings yet
- Past PaperssssDocument231 pagesPast PaperssssusamaNo ratings yet
- 1.7 Fluids PDFDocument6 pages1.7 Fluids PDFusamaNo ratings yet
- Infectious Diseases Notes PDFDocument1 pageInfectious Diseases Notes PDFusamaNo ratings yet
- Application Form For The Post ofDocument2 pagesApplication Form For The Post ofusamaNo ratings yet
- 240519ds4043 PDFDocument1 page240519ds4043 PDFusamaNo ratings yet
- Bromides Is What We NeedDocument3 pagesBromides Is What We Needusama100% (1)
- Flow Chart Showng Evalution in Community Medicine: Mbbs Third ProfessionalDocument9 pagesFlow Chart Showng Evalution in Community Medicine: Mbbs Third ProfessionalusamaNo ratings yet
- General Pearls .TXT Version 1Document9 pagesGeneral Pearls .TXT Version 1usamaNo ratings yet
- Final English Notes B SC PDFDocument31 pagesFinal English Notes B SC PDFusamaNo ratings yet
- Visual Mnemonics For Pathology: Marbas, Laurie LDocument3 pagesVisual Mnemonics For Pathology: Marbas, Laurie LusamaNo ratings yet
- Sci Digest Circ Respir Systems v1Document36 pagesSci Digest Circ Respir Systems v1draganNo ratings yet
- OB PathophysiologyDocument2 pagesOB PathophysiologyCathy SantosNo ratings yet
- Laporan Inhouse Clinic PT SIIX 2023Document135 pagesLaporan Inhouse Clinic PT SIIX 2023Tabita SilalahiNo ratings yet
- Call For ProposalsDocument5 pagesCall For ProposalsNITHYAPREMININo ratings yet
- Surgical Gastroenterologist in ChennaiDocument2 pagesSurgical Gastroenterologist in ChennaiSrivatsan GurumurthyNo ratings yet
- Urine Collection: Collecting A Clean Catch UrineDocument5 pagesUrine Collection: Collecting A Clean Catch UrineAngelene CalivaNo ratings yet
- Suicide and Undetermined Death by DrowningDocument10 pagesSuicide and Undetermined Death by DrowningJorge GomezNo ratings yet
- Mudra VigyanDocument13 pagesMudra VigyanYeathy Raj K NaiduNo ratings yet
- Give To CMC : Email DirectoryDocument11 pagesGive To CMC : Email DirectoryDanish KhanNo ratings yet
- DR ActivityDocument2 pagesDR ActivityVia Teresa AtienzaNo ratings yet
- Patofisiologi Addison DiseaseDocument4 pagesPatofisiologi Addison DiseaseDicoGunawijayaNo ratings yet
- "Article-PDF-naresh Sharma Binita Srivastava Hind P Bhatia Arch-849Document3 pages"Article-PDF-naresh Sharma Binita Srivastava Hind P Bhatia Arch-849Ruchi ShahNo ratings yet
- 1 SMDocument6 pages1 SMedi_wsNo ratings yet
- Microbiology Nca-Cls: Terms in This SetDocument18 pagesMicrobiology Nca-Cls: Terms in This SetjustinNo ratings yet
- BHP Ethical Issue in DialysisDocument3 pagesBHP Ethical Issue in DialysisIka Mutia SilvianaNo ratings yet
- Presentation On: Kgmu College of NursingDocument42 pagesPresentation On: Kgmu College of NursingSweety YadavNo ratings yet
- Notes of 2020Document90 pagesNotes of 2020eolhc rezarf100% (1)
- Yati Soenarto - RACP AucklandDocument34 pagesYati Soenarto - RACP AucklandIntan HartandyNo ratings yet
- CABG Surgical Case Study EditeDocument18 pagesCABG Surgical Case Study Editemaduwanthaharsha88No ratings yet
- The One Minute Preceptor 5 Microskills For One-On-One Teaching PDFDocument7 pagesThe One Minute Preceptor 5 Microskills For One-On-One Teaching PDFunderwood@eject.co.zaNo ratings yet
- Contents of The CHN RLE Written RequirementsDocument4 pagesContents of The CHN RLE Written RequirementsRoshie Kaye AbalorioNo ratings yet
- CSBP Post Stroke Checklist ENDocument2 pagesCSBP Post Stroke Checklist ENEduardo BessoloNo ratings yet
- Gero Study GuideDocument42 pagesGero Study GuideAbby Schmidt100% (1)
- Bronchial AsthmaDocument39 pagesBronchial AsthmaSaeed mohamed100% (1)
- Uso Correcto de CubrebocasDocument24 pagesUso Correcto de CubrebocasMarco LeónNo ratings yet
- Assisting-in-Lumbar-Puncture Procedure GuideDocument6 pagesAssisting-in-Lumbar-Puncture Procedure GuideLeigh Chanelle OngNo ratings yet
- Rule 11DDDocument3 pagesRule 11DDIonut ColcearNo ratings yet
- REport BlooodDocument3 pagesREport Bloooddivid joneNo ratings yet