
Alfredson Versus Silbernagel Exercise
Alfredson Versus Silbernagel Exercise
You might also like
- Valucare List of HospitalsDocument7 pagesValucare List of HospitalsShaina Bugayong64% (11)
- TB in The WorkplaceDocument60 pagesTB in The Workplacemefav7778520100% (2)
- The Bobath Concept - A Model To Illustrate Clinical Practice: Responding To Comments On Michielsen Et AlDocument3 pagesThe Bobath Concept - A Model To Illustrate Clinical Practice: Responding To Comments On Michielsen Et AlMayco BiasibettiNo ratings yet
- Studyprotocol Open AccessDocument17 pagesStudyprotocol Open AccessLeonardoValenzuelaNo ratings yet
- s12891 019 2796 5 PDFDocument22 pagess12891 019 2796 5 PDFAndré MesquitaNo ratings yet
- Effects of Combining Functional Exercises With ExeDocument9 pagesEffects of Combining Functional Exercises With ExeLuis GuioNo ratings yet
- Krauss 2016Document16 pagesKrauss 2016Alejandro GuzmanNo ratings yet
- Effectiveness and Efficiency of An 11-Week ExercisDocument17 pagesEffectiveness and Efficiency of An 11-Week ExercisVincentius Michael WilliantoNo ratings yet
- 2 Articulo MatrizDocument7 pages2 Articulo MatrizANGIE CAROLINA MEDINA VALLEJONo ratings yet
- Endurance and Strength Training in Pulmonary Rehabilitation For COPD PatientsDocument6 pagesEndurance and Strength Training in Pulmonary Rehabilitation For COPD PatientsMuhammad RedhaNo ratings yet
- Functional Electrical Stimulation With Exercises For Standing Balance and Weight Transfer in Acute Stroke PatientsDocument9 pagesFunctional Electrical Stimulation With Exercises For Standing Balance and Weight Transfer in Acute Stroke PatientsAugusto ManoelNo ratings yet
- Short Versus Long Rest Intervals For HypertrophyDocument12 pagesShort Versus Long Rest Intervals For Hypertrophylouthevelin0No ratings yet
- Endurance and Strength Training in Pulmonary Rehabilitation For COPD PatientsDocument6 pagesEndurance and Strength Training in Pulmonary Rehabilitation For COPD PatientsMuhammad RedhaNo ratings yet
- BMR 191803 PDFDocument10 pagesBMR 191803 PDFArchita AgarwalNo ratings yet
- Grgic 2017Document12 pagesGrgic 2017ChrisNo ratings yet
- Effectiveness of An 11-Week Exercise Intervention For Patients With Hip or Knee OsteoarthritisDocument17 pagesEffectiveness of An 11-Week Exercise Intervention For Patients With Hip or Knee Osteoarthritisyago.pessoaNo ratings yet
- Felcar 2018Document9 pagesFelcar 2018paulacagua06No ratings yet
- The Effectiveness of Physiotherapy Exercises in Subacromial Impingement Syndrome: A Systematic Review and Meta-AnalysisDocument20 pagesThe Effectiveness of Physiotherapy Exercises in Subacromial Impingement Syndrome: A Systematic Review and Meta-AnalysisBruno FellipeNo ratings yet
- Af - EpocDocument8 pagesAf - EpocOladysMelizaHoyosParraNo ratings yet
- Pone 0257595Document14 pagesPone 0257595Zulfah MidahNo ratings yet
- Trat Joelho PhisDocument12 pagesTrat Joelho PhisEduardo VieiraNo ratings yet
- bmr_2023_36-4_bmr-36-4-bmr220220_bmr-36-bmr220220Document15 pagesbmr_2023_36-4_bmr-36-4-bmr220220_bmr-36-bmr220220raina hanaNo ratings yet
- Bregenhof 2018Document13 pagesBregenhof 2018Rizal612No ratings yet
- SIS Specific or General ExerciseDocument18 pagesSIS Specific or General Exercise양종혁No ratings yet
- 1 s2.0 S2405844023078313 MainDocument14 pages1 s2.0 S2405844023078313 MainAsadm HosshNo ratings yet
- A Systematic Review Protocol On The Effectiveness of Therapeutic Exercises Utilised by Physiotherapists To Improve Function in Patients With BurnsDocument7 pagesA Systematic Review Protocol On The Effectiveness of Therapeutic Exercises Utilised by Physiotherapists To Improve Function in Patients With BurnsSintia DeviNo ratings yet
- Comparison of Three Types of Exc in The Treatment of Rotator Cuff TendinopathyShoulder Impingement SyndromeDocument7 pagesComparison of Three Types of Exc in The Treatment of Rotator Cuff TendinopathyShoulder Impingement SyndromeKholis RedcrossNo ratings yet
- Muscle Energy Technique For Chronic Obstructive Pulmonary Disease: A Systematic ReviewDocument7 pagesMuscle Energy Technique For Chronic Obstructive Pulmonary Disease: A Systematic ReviewICA MULIADI VALENTINE HULUNo ratings yet
- Dosages of Swallowing Exercises in Stroke Rehabilitation - A Systematic ReviewDocument29 pagesDosages of Swallowing Exercises in Stroke Rehabilitation - A Systematic ReviewMaria DemetriouNo ratings yet
- Chapter 3 Intervention Description and RationaleDocument11 pagesChapter 3 Intervention Description and RationaleDanielle Mae LadringanNo ratings yet
- McDonough2010 Article TheBack2ActivityTrialEducation PDFDocument8 pagesMcDonough2010 Article TheBack2ActivityTrialEducation PDFSandro PerilloNo ratings yet
- Combination of Inspiratory and Expiratory Muscle Training in Same Respiratory Cycle Versus Different Cycles in COPD Patients: A Randomized TrialDocument11 pagesCombination of Inspiratory and Expiratory Muscle Training in Same Respiratory Cycle Versus Different Cycles in COPD Patients: A Randomized TrialZulfah MidahNo ratings yet
- The Effects On Pain, Physical Function, and Quality of Life of Quadriceps Strengthening Exercises Combined With Baduanjin Qigong in Older Adults With Knee Osteoarthritis: A Quasi-Experimental StudyDocument11 pagesThe Effects On Pain, Physical Function, and Quality of Life of Quadriceps Strengthening Exercises Combined With Baduanjin Qigong in Older Adults With Knee Osteoarthritis: A Quasi-Experimental StudySiti lestarinurhamidahNo ratings yet
- Ejercicio Manguito Rotador LitlewoodDocument9 pagesEjercicio Manguito Rotador LitlewoodAntonio tapiaNo ratings yet
- Comparacion Articulos de Tres Ejercicios para Manguito Rotador en InglesDocument26 pagesComparacion Articulos de Tres Ejercicios para Manguito Rotador en IngleskarolndNo ratings yet
- Protocolo Correção HipercifoseDocument10 pagesProtocolo Correção HipercifosetyanafmNo ratings yet
- Effects of Whole-Body Electromyostimulation On Health and Performance: A Systematic ReviewDocument14 pagesEffects of Whole-Body Electromyostimulation On Health and Performance: A Systematic Reviewprettysia suvarlyNo ratings yet
- Progressive Early Passive and Active Exercise Therapy After Surgical Rotator Cuff Repair - Study Protocol For A Randomized Controlled Trial (The CUT-N-MOVE Trial)Document12 pagesProgressive Early Passive and Active Exercise Therapy After Surgical Rotator Cuff Repair - Study Protocol For A Randomized Controlled Trial (The CUT-N-MOVE Trial)Luna Tatiana Garces DuranNo ratings yet
- The Effects of Serial Casting On Lower Limb Function For Children With Cerebral Palsy: A Systematic Review With Meta-AnalysisDocument23 pagesThe Effects of Serial Casting On Lower Limb Function For Children With Cerebral Palsy: A Systematic Review With Meta-AnalysisDaniel MarvasoNo ratings yet
- Chest Expander Spring A Low Cost Home Physiotherapybased Exercise Rehabilitation After Total Hip ArthroplastyDocument11 pagesChest Expander Spring A Low Cost Home Physiotherapybased Exercise Rehabilitation After Total Hip ArthroplastyAmar DahmaniNo ratings yet
- Aluko2013 2Document11 pagesAluko2013 2Dr Ahmed NabilNo ratings yet
- The Effectiveness of A 12 Week Exercise Programme in Hip Osteoarthritis A Randomised Controlled TrialDocument6 pagesThe Effectiveness of A 12 Week Exercise Programme in Hip Osteoarthritis A Randomised Controlled TrialHerald Scholarly Open AccessNo ratings yet
- Paper 1Document9 pagesPaper 1Pablo Cuevas SaldivarNo ratings yet
- Benefits of High-Intensity Exercise Training To Patients With Chronic Obstructive Pulmonary Disease: A Controlled StudyDocument10 pagesBenefits of High-Intensity Exercise Training To Patients With Chronic Obstructive Pulmonary Disease: A Controlled StudyCésarNo ratings yet
- 1 s2.0 S1836955322001163 MainDocument2 pages1 s2.0 S1836955322001163 MainIhuoma AnaghaNo ratings yet
- Work-Related Medical RehabilitDocument12 pagesWork-Related Medical RehabilitMonicawindyNo ratings yet
- Low Back PainDocument9 pagesLow Back PaintamiNo ratings yet
- RPGDocument9 pagesRPGangelica barrazaNo ratings yet
- Dalgas 2008Document19 pagesDalgas 2008Pilat BogdanNo ratings yet
- Sensors 22 08069Document15 pagesSensors 22 08069Farhat SultanNo ratings yet
- Bateman 2019Document7 pagesBateman 2019physiodeepeshNo ratings yet
- Studyprotocol Open AccessDocument14 pagesStudyprotocol Open AccessMahmoud El MohamdyNo ratings yet
- Efects of Adding Aerobic Physical ActivityDocument18 pagesEfects of Adding Aerobic Physical Activitydavid fernandezNo ratings yet
- Concurrent Training For Sports Performance - The 2 Sides of The MedalDocument8 pagesConcurrent Training For Sports Performance - The 2 Sides of The MedalDouglas MarinNo ratings yet
- Fasten AuDocument10 pagesFasten AuDina M LestaryNo ratings yet
- University of Essex School of Sport, Rehabilitation and Exercise Sciences SE720 Using Evidence in Healthcare Practice Assignment WorkbookDocument85 pagesUniversity of Essex School of Sport, Rehabilitation and Exercise Sciences SE720 Using Evidence in Healthcare Practice Assignment WorkbookShibli LondonNo ratings yet
- Effects of Continuous and Interval Training On Different Fitness Parameters in AthletesDocument4 pagesEffects of Continuous and Interval Training On Different Fitness Parameters in AthletesYared TegegneNo ratings yet
- Rehabilitation and Return To Sports After Acl ReconstructionDocument5 pagesRehabilitation and Return To Sports After Acl ReconstructionjasonoytumandukNo ratings yet
- IntervalexercisetrialAnnals2006 PDFDocument12 pagesIntervalexercisetrialAnnals2006 PDFrunmenNo ratings yet
- Fidalgo Et Al - 2019Document15 pagesFidalgo Et Al - 2019TAINAH DE PAULANo ratings yet
- Lit Review 1Document6 pagesLit Review 1api-749269676No ratings yet
- Basic Exercise Physiology: Clinical and Laboratory PerspectivesFrom EverandBasic Exercise Physiology: Clinical and Laboratory PerspectivesNo ratings yet
- Abbate - Holding The Tiger's TailDocument262 pagesAbbate - Holding The Tiger's TailJohnson100% (2)
- The State of The County Address 2015Document153 pagesThe State of The County Address 2015api-245299850No ratings yet
- MelanomaDocument175 pagesMelanomaHelenaIbarraNo ratings yet
- Alumni Directory PDFDocument40 pagesAlumni Directory PDFvinodkharNo ratings yet
- TraumaDocument16 pagesTraumaAnzala KhanNo ratings yet
- Acute Critical Care Nursing HandoutDocument17 pagesAcute Critical Care Nursing HandoutRuby Ann Dimayuga100% (1)
- EntreprenurseDocument63 pagesEntreprenursevmaquilingNo ratings yet
- Krishna Institute of Medical Sciences Deemed University: Name of Investigator Budget Sr. Project No. Name of ProjectDocument38 pagesKrishna Institute of Medical Sciences Deemed University: Name of Investigator Budget Sr. Project No. Name of ProjectchahatpuriNo ratings yet
- Jurnal MassageDocument8 pagesJurnal MassageDyah PridamiNo ratings yet
- Consumer Protection Act 1999, Act 599 17Document93 pagesConsumer Protection Act 1999, Act 599 17Ho Shun MingNo ratings yet
- #1 Sosialisasi E-Report IKP RS Eksternal - 2021Document37 pages#1 Sosialisasi E-Report IKP RS Eksternal - 2021Benny GunawanNo ratings yet
- PaternalismDocument4 pagesPaternalismJeibel BullecerNo ratings yet
- BMJNPH 2022 000477.fullDocument18 pagesBMJNPH 2022 000477.fullcatiatexNo ratings yet
- A Lawyer Can Assist With Your Car Accident Claim - Here's HowDocument4 pagesA Lawyer Can Assist With Your Car Accident Claim - Here's HowTariqul Islam AyanNo ratings yet
- Manulife Costco Emergency Medical Policy Travel Insurance Canadians Policy enDocument14 pagesManulife Costco Emergency Medical Policy Travel Insurance Canadians Policy enSara AdelNo ratings yet
- NCP For Case Presentation (Acute Pain, Episiotomy)Document3 pagesNCP For Case Presentation (Acute Pain, Episiotomy)Jenny Ajoc100% (2)
- Hamdard Community CentreDocument5 pagesHamdard Community CentreAnonymous S2xezUotINo ratings yet
- Vac SeatsDocument2 pagesVac SeatsRasha Pulath20No ratings yet
- Scotterven Medicaldevicespasswordstopwnage 150722215821 Lva1 App6892Document67 pagesScotterven Medicaldevicespasswordstopwnage 150722215821 Lva1 App6892Kooganeswaran AarumugamNo ratings yet
- 7.0 Patient EducationDocument25 pages7.0 Patient Educationx483xDNo ratings yet
- Vice Chancellor DR NTR University of Health Sciences VijayawadaDocument3 pagesVice Chancellor DR NTR University of Health Sciences Vijayawadabrunda maneepuriNo ratings yet
- Endovascular Aortic Aneurysm Repair (EVAR)Document5 pagesEndovascular Aortic Aneurysm Repair (EVAR)D FNo ratings yet
- Quarter 2 Lesson 6 Treatment For Common Sports InjuryDocument6 pagesQuarter 2 Lesson 6 Treatment For Common Sports InjuryRowan Yñigo TamayoNo ratings yet
- Notes - Up Till September 9, 2021Document40 pagesNotes - Up Till September 9, 2021vedant wakankarNo ratings yet
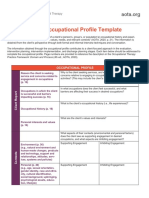
- AOTA Occupational Profile TemplateDocument2 pagesAOTA Occupational Profile Templatemelissa calabreseNo ratings yet
- Rishum 1 262421216 2Document1 pageRishum 1 262421216 2HellcroZNo ratings yet
- AL Molecular Diagnostic Laboratory Inc.: Dasmariñas, CaviteDocument2 pagesAL Molecular Diagnostic Laboratory Inc.: Dasmariñas, CaviteJazzmine C. RubricoNo ratings yet
- Carrer Interview 14Document3 pagesCarrer Interview 14api-252808904No ratings yet
























































































Download as pdf or txt
You might also like
- Valucare List of HospitalsDocument7 pagesValucare List of HospitalsShaina Bugayong64% (11)
- TB in The WorkplaceDocument60 pagesTB in The Workplacemefav7778520100% (2)
- The Bobath Concept - A Model To Illustrate Clinical Practice: Responding To Comments On Michielsen Et AlDocument3 pagesThe Bobath Concept - A Model To Illustrate Clinical Practice: Responding To Comments On Michielsen Et AlMayco BiasibettiNo ratings yet
- Studyprotocol Open AccessDocument17 pagesStudyprotocol Open AccessLeonardoValenzuelaNo ratings yet
- s12891 019 2796 5 PDFDocument22 pagess12891 019 2796 5 PDFAndré MesquitaNo ratings yet
- Effects of Combining Functional Exercises With ExeDocument9 pagesEffects of Combining Functional Exercises With ExeLuis GuioNo ratings yet
- Krauss 2016Document16 pagesKrauss 2016Alejandro GuzmanNo ratings yet
- Effectiveness and Efficiency of An 11-Week ExercisDocument17 pagesEffectiveness and Efficiency of An 11-Week ExercisVincentius Michael WilliantoNo ratings yet
- 2 Articulo MatrizDocument7 pages2 Articulo MatrizANGIE CAROLINA MEDINA VALLEJONo ratings yet
- Endurance and Strength Training in Pulmonary Rehabilitation For COPD PatientsDocument6 pagesEndurance and Strength Training in Pulmonary Rehabilitation For COPD PatientsMuhammad RedhaNo ratings yet
- Functional Electrical Stimulation With Exercises For Standing Balance and Weight Transfer in Acute Stroke PatientsDocument9 pagesFunctional Electrical Stimulation With Exercises For Standing Balance and Weight Transfer in Acute Stroke PatientsAugusto ManoelNo ratings yet
- Short Versus Long Rest Intervals For HypertrophyDocument12 pagesShort Versus Long Rest Intervals For Hypertrophylouthevelin0No ratings yet
- Endurance and Strength Training in Pulmonary Rehabilitation For COPD PatientsDocument6 pagesEndurance and Strength Training in Pulmonary Rehabilitation For COPD PatientsMuhammad RedhaNo ratings yet
- BMR 191803 PDFDocument10 pagesBMR 191803 PDFArchita AgarwalNo ratings yet
- Grgic 2017Document12 pagesGrgic 2017ChrisNo ratings yet
- Effectiveness of An 11-Week Exercise Intervention For Patients With Hip or Knee OsteoarthritisDocument17 pagesEffectiveness of An 11-Week Exercise Intervention For Patients With Hip or Knee Osteoarthritisyago.pessoaNo ratings yet
- Felcar 2018Document9 pagesFelcar 2018paulacagua06No ratings yet
- The Effectiveness of Physiotherapy Exercises in Subacromial Impingement Syndrome: A Systematic Review and Meta-AnalysisDocument20 pagesThe Effectiveness of Physiotherapy Exercises in Subacromial Impingement Syndrome: A Systematic Review and Meta-AnalysisBruno FellipeNo ratings yet
- Af - EpocDocument8 pagesAf - EpocOladysMelizaHoyosParraNo ratings yet
- Pone 0257595Document14 pagesPone 0257595Zulfah MidahNo ratings yet
- Trat Joelho PhisDocument12 pagesTrat Joelho PhisEduardo VieiraNo ratings yet
- bmr_2023_36-4_bmr-36-4-bmr220220_bmr-36-bmr220220Document15 pagesbmr_2023_36-4_bmr-36-4-bmr220220_bmr-36-bmr220220raina hanaNo ratings yet
- Bregenhof 2018Document13 pagesBregenhof 2018Rizal612No ratings yet
- SIS Specific or General ExerciseDocument18 pagesSIS Specific or General Exercise양종혁No ratings yet
- 1 s2.0 S2405844023078313 MainDocument14 pages1 s2.0 S2405844023078313 MainAsadm HosshNo ratings yet
- A Systematic Review Protocol On The Effectiveness of Therapeutic Exercises Utilised by Physiotherapists To Improve Function in Patients With BurnsDocument7 pagesA Systematic Review Protocol On The Effectiveness of Therapeutic Exercises Utilised by Physiotherapists To Improve Function in Patients With BurnsSintia DeviNo ratings yet
- Comparison of Three Types of Exc in The Treatment of Rotator Cuff TendinopathyShoulder Impingement SyndromeDocument7 pagesComparison of Three Types of Exc in The Treatment of Rotator Cuff TendinopathyShoulder Impingement SyndromeKholis RedcrossNo ratings yet
- Muscle Energy Technique For Chronic Obstructive Pulmonary Disease: A Systematic ReviewDocument7 pagesMuscle Energy Technique For Chronic Obstructive Pulmonary Disease: A Systematic ReviewICA MULIADI VALENTINE HULUNo ratings yet
- Dosages of Swallowing Exercises in Stroke Rehabilitation - A Systematic ReviewDocument29 pagesDosages of Swallowing Exercises in Stroke Rehabilitation - A Systematic ReviewMaria DemetriouNo ratings yet
- Chapter 3 Intervention Description and RationaleDocument11 pagesChapter 3 Intervention Description and RationaleDanielle Mae LadringanNo ratings yet
- McDonough2010 Article TheBack2ActivityTrialEducation PDFDocument8 pagesMcDonough2010 Article TheBack2ActivityTrialEducation PDFSandro PerilloNo ratings yet
- Combination of Inspiratory and Expiratory Muscle Training in Same Respiratory Cycle Versus Different Cycles in COPD Patients: A Randomized TrialDocument11 pagesCombination of Inspiratory and Expiratory Muscle Training in Same Respiratory Cycle Versus Different Cycles in COPD Patients: A Randomized TrialZulfah MidahNo ratings yet
- The Effects On Pain, Physical Function, and Quality of Life of Quadriceps Strengthening Exercises Combined With Baduanjin Qigong in Older Adults With Knee Osteoarthritis: A Quasi-Experimental StudyDocument11 pagesThe Effects On Pain, Physical Function, and Quality of Life of Quadriceps Strengthening Exercises Combined With Baduanjin Qigong in Older Adults With Knee Osteoarthritis: A Quasi-Experimental StudySiti lestarinurhamidahNo ratings yet
- Ejercicio Manguito Rotador LitlewoodDocument9 pagesEjercicio Manguito Rotador LitlewoodAntonio tapiaNo ratings yet
- Comparacion Articulos de Tres Ejercicios para Manguito Rotador en InglesDocument26 pagesComparacion Articulos de Tres Ejercicios para Manguito Rotador en IngleskarolndNo ratings yet
- Protocolo Correção HipercifoseDocument10 pagesProtocolo Correção HipercifosetyanafmNo ratings yet
- Effects of Whole-Body Electromyostimulation On Health and Performance: A Systematic ReviewDocument14 pagesEffects of Whole-Body Electromyostimulation On Health and Performance: A Systematic Reviewprettysia suvarlyNo ratings yet
- Progressive Early Passive and Active Exercise Therapy After Surgical Rotator Cuff Repair - Study Protocol For A Randomized Controlled Trial (The CUT-N-MOVE Trial)Document12 pagesProgressive Early Passive and Active Exercise Therapy After Surgical Rotator Cuff Repair - Study Protocol For A Randomized Controlled Trial (The CUT-N-MOVE Trial)Luna Tatiana Garces DuranNo ratings yet
- The Effects of Serial Casting On Lower Limb Function For Children With Cerebral Palsy: A Systematic Review With Meta-AnalysisDocument23 pagesThe Effects of Serial Casting On Lower Limb Function For Children With Cerebral Palsy: A Systematic Review With Meta-AnalysisDaniel MarvasoNo ratings yet
- Chest Expander Spring A Low Cost Home Physiotherapybased Exercise Rehabilitation After Total Hip ArthroplastyDocument11 pagesChest Expander Spring A Low Cost Home Physiotherapybased Exercise Rehabilitation After Total Hip ArthroplastyAmar DahmaniNo ratings yet
- Aluko2013 2Document11 pagesAluko2013 2Dr Ahmed NabilNo ratings yet
- The Effectiveness of A 12 Week Exercise Programme in Hip Osteoarthritis A Randomised Controlled TrialDocument6 pagesThe Effectiveness of A 12 Week Exercise Programme in Hip Osteoarthritis A Randomised Controlled TrialHerald Scholarly Open AccessNo ratings yet
- Paper 1Document9 pagesPaper 1Pablo Cuevas SaldivarNo ratings yet
- Benefits of High-Intensity Exercise Training To Patients With Chronic Obstructive Pulmonary Disease: A Controlled StudyDocument10 pagesBenefits of High-Intensity Exercise Training To Patients With Chronic Obstructive Pulmonary Disease: A Controlled StudyCésarNo ratings yet
- 1 s2.0 S1836955322001163 MainDocument2 pages1 s2.0 S1836955322001163 MainIhuoma AnaghaNo ratings yet
- Work-Related Medical RehabilitDocument12 pagesWork-Related Medical RehabilitMonicawindyNo ratings yet
- Low Back PainDocument9 pagesLow Back PaintamiNo ratings yet
- RPGDocument9 pagesRPGangelica barrazaNo ratings yet
- Dalgas 2008Document19 pagesDalgas 2008Pilat BogdanNo ratings yet
- Sensors 22 08069Document15 pagesSensors 22 08069Farhat SultanNo ratings yet
- Bateman 2019Document7 pagesBateman 2019physiodeepeshNo ratings yet
- Studyprotocol Open AccessDocument14 pagesStudyprotocol Open AccessMahmoud El MohamdyNo ratings yet
- Efects of Adding Aerobic Physical ActivityDocument18 pagesEfects of Adding Aerobic Physical Activitydavid fernandezNo ratings yet
- Concurrent Training For Sports Performance - The 2 Sides of The MedalDocument8 pagesConcurrent Training For Sports Performance - The 2 Sides of The MedalDouglas MarinNo ratings yet
- Fasten AuDocument10 pagesFasten AuDina M LestaryNo ratings yet
- University of Essex School of Sport, Rehabilitation and Exercise Sciences SE720 Using Evidence in Healthcare Practice Assignment WorkbookDocument85 pagesUniversity of Essex School of Sport, Rehabilitation and Exercise Sciences SE720 Using Evidence in Healthcare Practice Assignment WorkbookShibli LondonNo ratings yet
- Effects of Continuous and Interval Training On Different Fitness Parameters in AthletesDocument4 pagesEffects of Continuous and Interval Training On Different Fitness Parameters in AthletesYared TegegneNo ratings yet
- Rehabilitation and Return To Sports After Acl ReconstructionDocument5 pagesRehabilitation and Return To Sports After Acl ReconstructionjasonoytumandukNo ratings yet
- IntervalexercisetrialAnnals2006 PDFDocument12 pagesIntervalexercisetrialAnnals2006 PDFrunmenNo ratings yet
- Fidalgo Et Al - 2019Document15 pagesFidalgo Et Al - 2019TAINAH DE PAULANo ratings yet
- Lit Review 1Document6 pagesLit Review 1api-749269676No ratings yet
- Basic Exercise Physiology: Clinical and Laboratory PerspectivesFrom EverandBasic Exercise Physiology: Clinical and Laboratory PerspectivesNo ratings yet
- Abbate - Holding The Tiger's TailDocument262 pagesAbbate - Holding The Tiger's TailJohnson100% (2)
- The State of The County Address 2015Document153 pagesThe State of The County Address 2015api-245299850No ratings yet
- MelanomaDocument175 pagesMelanomaHelenaIbarraNo ratings yet
- Alumni Directory PDFDocument40 pagesAlumni Directory PDFvinodkharNo ratings yet
- TraumaDocument16 pagesTraumaAnzala KhanNo ratings yet
- Acute Critical Care Nursing HandoutDocument17 pagesAcute Critical Care Nursing HandoutRuby Ann Dimayuga100% (1)
- EntreprenurseDocument63 pagesEntreprenursevmaquilingNo ratings yet
- Krishna Institute of Medical Sciences Deemed University: Name of Investigator Budget Sr. Project No. Name of ProjectDocument38 pagesKrishna Institute of Medical Sciences Deemed University: Name of Investigator Budget Sr. Project No. Name of ProjectchahatpuriNo ratings yet
- Jurnal MassageDocument8 pagesJurnal MassageDyah PridamiNo ratings yet
- Consumer Protection Act 1999, Act 599 17Document93 pagesConsumer Protection Act 1999, Act 599 17Ho Shun MingNo ratings yet
- #1 Sosialisasi E-Report IKP RS Eksternal - 2021Document37 pages#1 Sosialisasi E-Report IKP RS Eksternal - 2021Benny GunawanNo ratings yet
- PaternalismDocument4 pagesPaternalismJeibel BullecerNo ratings yet
- BMJNPH 2022 000477.fullDocument18 pagesBMJNPH 2022 000477.fullcatiatexNo ratings yet
- A Lawyer Can Assist With Your Car Accident Claim - Here's HowDocument4 pagesA Lawyer Can Assist With Your Car Accident Claim - Here's HowTariqul Islam AyanNo ratings yet
- Manulife Costco Emergency Medical Policy Travel Insurance Canadians Policy enDocument14 pagesManulife Costco Emergency Medical Policy Travel Insurance Canadians Policy enSara AdelNo ratings yet
- NCP For Case Presentation (Acute Pain, Episiotomy)Document3 pagesNCP For Case Presentation (Acute Pain, Episiotomy)Jenny Ajoc100% (2)
- Hamdard Community CentreDocument5 pagesHamdard Community CentreAnonymous S2xezUotINo ratings yet
- Vac SeatsDocument2 pagesVac SeatsRasha Pulath20No ratings yet
- Scotterven Medicaldevicespasswordstopwnage 150722215821 Lva1 App6892Document67 pagesScotterven Medicaldevicespasswordstopwnage 150722215821 Lva1 App6892Kooganeswaran AarumugamNo ratings yet
- 7.0 Patient EducationDocument25 pages7.0 Patient Educationx483xDNo ratings yet
- Vice Chancellor DR NTR University of Health Sciences VijayawadaDocument3 pagesVice Chancellor DR NTR University of Health Sciences Vijayawadabrunda maneepuriNo ratings yet
- Endovascular Aortic Aneurysm Repair (EVAR)Document5 pagesEndovascular Aortic Aneurysm Repair (EVAR)D FNo ratings yet
- Quarter 2 Lesson 6 Treatment For Common Sports InjuryDocument6 pagesQuarter 2 Lesson 6 Treatment For Common Sports InjuryRowan Yñigo TamayoNo ratings yet
- Notes - Up Till September 9, 2021Document40 pagesNotes - Up Till September 9, 2021vedant wakankarNo ratings yet
- AOTA Occupational Profile TemplateDocument2 pagesAOTA Occupational Profile Templatemelissa calabreseNo ratings yet
- Rishum 1 262421216 2Document1 pageRishum 1 262421216 2HellcroZNo ratings yet
- AL Molecular Diagnostic Laboratory Inc.: Dasmariñas, CaviteDocument2 pagesAL Molecular Diagnostic Laboratory Inc.: Dasmariñas, CaviteJazzmine C. RubricoNo ratings yet
- Carrer Interview 14Document3 pagesCarrer Interview 14api-252808904No ratings yet