Download as pdf or txt
You might also like
- Cabin Crew Safety Training Manual PDFDocument217 pagesCabin Crew Safety Training Manual PDFsebastien100% (4)
- Ohybacka XONM 2000 - 2A-4 PDFDocument44 pagesOhybacka XONM 2000 - 2A-4 PDFKrajits ZdaryNo ratings yet
- IDIP Report Sample PDFDocument33 pagesIDIP Report Sample PDFKhuda Buksh67% (18)
- Reading For Writing:, QF El8ft1ñw-MvDocument16 pagesReading For Writing:, QF El8ft1ñw-MvRo DooNo ratings yet
- Further Mathematics For Economic Analysi PDFDocument310 pagesFurther Mathematics For Economic Analysi PDFTina CRNo ratings yet
- Goljan - 100pg - Hi - Yield - Notes 2Document101 pagesGoljan - 100pg - Hi - Yield - Notes 2tweetyw00No ratings yet
- A New Species of Forcipomyia (Diptera, Ceratopogonidae) Described in All Stages, With An Account of ItsDocument8 pagesA New Species of Forcipomyia (Diptera, Ceratopogonidae) Described in All Stages, With An Account of ItsA.JNo ratings yet
- Teaching The Heimlich ManeuverDocument3 pagesTeaching The Heimlich ManeuversherrillmattNo ratings yet
- Trematodes FlukesDocument14 pagesTrematodes FlukesAbby CruzNo ratings yet
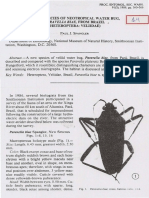
- 14 - Spangler 1989Document7 pages14 - Spangler 1989oséias martins magalhãesNo ratings yet
- Holmes 2001Document27 pagesHolmes 2001Pablo GutiérrezNo ratings yet
- 2005 Final Exam PDFDocument35 pages2005 Final Exam PDFAndreea AndraNo ratings yet
- Boc HemaDocument72 pagesBoc HemaFenyl Isis GuigayomaNo ratings yet
- Physiology of Virus-Infected Plants: (Agricultural College and Research Institute. Coimbatore)Document11 pagesPhysiology of Virus-Infected Plants: (Agricultural College and Research Institute. Coimbatore)Syed Mushahid Hussain NaqviNo ratings yet
- Destor V.W - Lab Exercise 15 - Digestive System - dvm2fDocument31 pagesDestor V.W - Lab Exercise 15 - Digestive System - dvm2fAbdul Rahman OgagangNo ratings yet
- PapersDocument164 pagesPaperstaniaNo ratings yet
- Efectos de La Parotina en Huesos LargosDocument6 pagesEfectos de La Parotina en Huesos LargosAlejandro GuzmanNo ratings yet
- Cardiovasculary SystemDocument12 pagesCardiovasculary Systempriyanka.2023.999No ratings yet
- Exercises and AnswersDocument9 pagesExercises and Answersحسين الخليفةNo ratings yet
- Anatomy of The Auditory Pathways With Emphasis On The Brain StemDocument14 pagesAnatomy of The Auditory Pathways With Emphasis On The Brain StemSal MonNo ratings yet
- STPM Trial 2009 Bio Q&A (Melaka)Document36 pagesSTPM Trial 2009 Bio Q&A (Melaka)SimPorNo ratings yet
- Bio ProjectDocument14 pagesBio Projectvinai PrasannaNo ratings yet
- Telegram Cloud Document 4 5893461163299045618 PDFDocument232 pagesTelegram Cloud Document 4 5893461163299045618 PDFAndreea FlorinaNo ratings yet
- Adobe Scan Mar 10, 2024Document22 pagesAdobe Scan Mar 10, 2024varadgade2020No ratings yet
- Cladistics - The Theory and Practice of Parsimony Analysis)Document240 pagesCladistics - The Theory and Practice of Parsimony Analysis)gushaNo ratings yet
- Characteristics of Firesetters in Different Developmental StagesDocument84 pagesCharacteristics of Firesetters in Different Developmental StagesmireilleNo ratings yet
- Alaa AdnanDocument3 pagesAlaa AdnanHadiNo ratings yet
- Review Present Perfect HomeworkDocument1 pageReview Present Perfect HomeworkAbimael GranilloNo ratings yet
- Help For StudentsDocument12 pagesHelp For StudentsMobin Ul HaqNo ratings yet
- TervitDocument5 pagesTervitSuhail MagrayNo ratings yet
- Davidson 013711865Document341 pagesDavidson 013711865be wattimNo ratings yet
- Adobe Scan Jun 10, 2023Document14 pagesAdobe Scan Jun 10, 2023Anushka SinghNo ratings yet
- "' Itry: Gan BacilliDocument13 pages"' Itry: Gan BacilliSandra PiedadeNo ratings yet
- Printed in U.S.A.: 1987 by The Williams & Wilkins Co. Vol. 48, No. 5Document12 pagesPrinted in U.S.A.: 1987 by The Williams & Wilkins Co. Vol. 48, No. 5AdmirNo ratings yet
- Slipinski 1989Document46 pagesSlipinski 1989bolosphex1634No ratings yet
- lolo: Central Intelugence AgencyDocument20 pageslolo: Central Intelugence Agencylewisw.stiNo ratings yet
- PIN:81563 Borah: City X.Ray LaboraioryDocument3 pagesPIN:81563 Borah: City X.Ray LaboraioryAgile Hospitals Pvt. Ltd.No ratings yet
- 2A The British Object Relations School W.R. Fairbairn and D.W. WinnicottDocument14 pages2A The British Object Relations School W.R. Fairbairn and D.W. WinnicottAdán Peralta GómezNo ratings yet
- Hayashi e Cedenho, 1980Document4 pagesHayashi e Cedenho, 1980Beatrice MacenteNo ratings yet
- La CP 90 122Document4 pagesLa CP 90 122Peyton ManualNo ratings yet
- Aoprove't::l For Release CIA-RDP9'6-00787R000100070001-5Document33 pagesAoprove't::l For Release CIA-RDP9'6-00787R000100070001-5clekupreNo ratings yet
- Micro Slide 06 Spore Forming BacilliDocument5 pagesMicro Slide 06 Spore Forming Bacillihamza jassarNo ratings yet
- Adobe Scan 23 Nov 2023 2Document10 pagesAdobe Scan 23 Nov 2023 2FlojohannNo ratings yet
- Fuel Alcohol ProductionDocument51 pagesFuel Alcohol ProductionplutocowNo ratings yet
- Community Medicine SpottersDocument14 pagesCommunity Medicine SpottersINFY GNo ratings yet
- High Yield Neuroanatomy 2nd EditionDocument151 pagesHigh Yield Neuroanatomy 2nd Editionlakshminivas PingaliNo ratings yet
- 1886 Goldsmid Pazig Treatise of Magical Incantations PDFDocument56 pages1886 Goldsmid Pazig Treatise of Magical Incantations PDFRichmond AsareNo ratings yet
- Papa Jim's Herbal Magic Workbook by Papa JimDocument57 pagesPapa Jim's Herbal Magic Workbook by Papa JimRandom Person100% (1)
- Reporte de Charles WhitmanDocument10 pagesReporte de Charles Whitmanp.camposNo ratings yet
- White House Drug Control StrategyDocument2 pagesWhite House Drug Control StrategyKimberly Marie SousaNo ratings yet
- Spector 1966Document20 pagesSpector 1966Rah MliNo ratings yet
- Cooney The Potential Uses of Television in Preschool Education (Research For Sesame Street)Document57 pagesCooney The Potential Uses of Television in Preschool Education (Research For Sesame Street)OnlineMattNo ratings yet
- TOEICDocument1 pageTOEICPharameswara Maharani Pertiwi IINo ratings yet
- Anatomy of Flowering PlantsDocument16 pagesAnatomy of Flowering Plantsabhishek80562506877No ratings yet
- Minoxidil Solution - Pattern Baldness Among FilipinosDocument6 pagesMinoxidil Solution - Pattern Baldness Among FilipinosOllafNo ratings yet
- Amjpathol00500 0148Document5 pagesAmjpathol00500 0148hindesarahNo ratings yet
- Be-T.Q - RH.J: Tjy J To PayDocument3 pagesBe-T.Q - RH.J: Tjy J To PayAli MasoodNo ratings yet
- Pathology Paper 1Document25 pagesPathology Paper 1ismarttech143No ratings yet
- Cs AGNDocument177 pagesCs AGNMa Rafaela Rosales PalomponNo ratings yet
- Onvi 6Document3 pagesOnvi 6EduarToleNo ratings yet
- C05515705 - Train Ride See Triangle ObjectDocument3 pagesC05515705 - Train Ride See Triangle Objectlewisw.stiNo ratings yet
- Anterior Pituitary Hormones and Their Modus OperandiDocument63 pagesAnterior Pituitary Hormones and Their Modus OperandiKyra ThomasNo ratings yet
- The Maddest Idea: An Isaac Biddlecomb NovelFrom EverandThe Maddest Idea: An Isaac Biddlecomb NovelRating: 3.5 out of 5 stars3.5/5 (9)
- CAVACDocument9 pagesCAVACDr-Sadaqat Ali RaoNo ratings yet
- Toxoplasmosis - A Global ThreatDocument8 pagesToxoplasmosis - A Global ThreatDr-Sadaqat Ali RaoNo ratings yet
- Large Animal Surgery Course ContentsDocument2 pagesLarge Animal Surgery Course ContentsDr-Sadaqat Ali RaoNo ratings yet
- Large Animal Surgery Course ContentsDocument2 pagesLarge Animal Surgery Course ContentsDr-Sadaqat Ali RaoNo ratings yet
- Edited Ghulam Muhammad and M. Athar: Practice TipsDocument2 pagesEdited Ghulam Muhammad and M. Athar: Practice TipsDr-Sadaqat Ali RaoNo ratings yet
- Veterinary Parasitology: Cengiz Gokbulut, Quintin A. Mckellar TDocument26 pagesVeterinary Parasitology: Cengiz Gokbulut, Quintin A. Mckellar TDr-Sadaqat Ali RaoNo ratings yet
- Laboratory Identification of Arthropod Ectoparasites: Blaine A. Mathison, Bobbi S. PrittDocument20 pagesLaboratory Identification of Arthropod Ectoparasites: Blaine A. Mathison, Bobbi S. PrittDr-Sadaqat Ali RaoNo ratings yet
- Women's Studies International Forum: Meagan TylerDocument10 pagesWomen's Studies International Forum: Meagan TylerDr-Sadaqat Ali RaoNo ratings yet
- Trisodium Citrate Use in Dairy Cows and Effects On Daily Milk Yield and QualityDocument4 pagesTrisodium Citrate Use in Dairy Cows and Effects On Daily Milk Yield and QualityDr-Sadaqat Ali RaoNo ratings yet
- Veterinary Parasitology: Research PaperDocument5 pagesVeterinary Parasitology: Research PaperDr-Sadaqat Ali RaoNo ratings yet
- 1 s2.0 S0304401718302978 MainDocument32 pages1 s2.0 S0304401718302978 MainDr-Sadaqat Ali RaoNo ratings yet
- Flavor Experiences During Formula Feeding Are Related To Preferences During ChildhoodDocument12 pagesFlavor Experiences During Formula Feeding Are Related To Preferences During ChildhoodDr-Sadaqat Ali RaoNo ratings yet
- Acta Tropica: SciencedirectDocument7 pagesActa Tropica: SciencedirectDr-Sadaqat Ali RaoNo ratings yet
- Veterinary Parasitology: Cengiz Gokbulut, Quintin A. Mckellar TDocument26 pagesVeterinary Parasitology: Cengiz Gokbulut, Quintin A. Mckellar TDr-Sadaqat Ali RaoNo ratings yet
- Purchased by The U.S. Dept. of Agriculture, For Official UseDocument7 pagesPurchased by The U.S. Dept. of Agriculture, For Official UseDr-Sadaqat Ali RaoNo ratings yet
- Vetipedia - Drugs (Trade Names)Document11 pagesVetipedia - Drugs (Trade Names)Dr-Sadaqat Ali RaoNo ratings yet
- Chronic Wound Pedis (D) : Zulfikri Saleh Islami (K1A115049) Supervisor: Dr. Saktrio Darmono Subarno, Sp. BP-REDocument28 pagesChronic Wound Pedis (D) : Zulfikri Saleh Islami (K1A115049) Supervisor: Dr. Saktrio Darmono Subarno, Sp. BP-REZulfikri IslamiNo ratings yet
- Book Review: Thoracic Imaging: Pulmonary and Cardiovascular Radiology, 2nd Ed. by W. Richard Webb and Charles R. HigginsDocument1 pageBook Review: Thoracic Imaging: Pulmonary and Cardiovascular Radiology, 2nd Ed. by W. Richard Webb and Charles R. HigginsDr Apoorva ReddyNo ratings yet
- Principle of Good Clinical PracticeDocument39 pagesPrinciple of Good Clinical PracticeVasavi ChittemreddyNo ratings yet
- Clinical Protocol in Pediatrics, 2012Document96 pagesClinical Protocol in Pediatrics, 2012floare de colt100% (1)
- CR Piopneumothoraks Nicky FIXdDocument62 pagesCR Piopneumothoraks Nicky FIXdPutri RahmawatiNo ratings yet
- DownloadDocument15 pagesDownloadMiriam SanchezNo ratings yet
- Improvised Water Filter CupDocument18 pagesImprovised Water Filter CupJohn Carlo100% (1)
- Wingila Mpamila Worksheet 8Document2 pagesWingila Mpamila Worksheet 8welcome martinNo ratings yet
- Moh - Issp - TemplateDocument25 pagesMoh - Issp - TemplateRocky MontañerNo ratings yet
- Critical AnalysisDocument2 pagesCritical Analysisjuaxxo50% (2)
- Effectiveness of Performance Appraisal System Towards "Dabur India LTD."Document85 pagesEffectiveness of Performance Appraisal System Towards "Dabur India LTD."Ashwani kumarNo ratings yet
- Footprints: Celebrating 40 Years of God's Faithfulness: Bangalore Baptist Hospital 1973-2012 (Sample Pages)Document22 pagesFootprints: Celebrating 40 Years of God's Faithfulness: Bangalore Baptist Hospital 1973-2012 (Sample Pages)imasubscribderNo ratings yet
- Psychology of Sport and Exercise: P. Wylleman, C.G. Harwood, A.-M. Elbe, A. Reints, D. de CaluweDocument12 pagesPsychology of Sport and Exercise: P. Wylleman, C.G. Harwood, A.-M. Elbe, A. Reints, D. de CaluweAraya ThimlamomNo ratings yet
- Spine Hook Surgical TechniqueDocument1 pageSpine Hook Surgical TechniqueToño VeraNo ratings yet
- Oral Health Status of Immigrant and Refugee Children in North America: A Scoping ReviewDocument18 pagesOral Health Status of Immigrant and Refugee Children in North America: A Scoping ReviewFaiqotul KumalaNo ratings yet
- Company Profile: Sistema Inteligente de Color, Descubrir Tu Valor ExcepcionalDocument4 pagesCompany Profile: Sistema Inteligente de Color, Descubrir Tu Valor ExcepcionalOmar Stalin Lucio RonNo ratings yet
- Safety Data Sheet: NPK/NP/NK ( 70% AN) : Non-HazardousDocument16 pagesSafety Data Sheet: NPK/NP/NK ( 70% AN) : Non-HazardousMahmoud MahmoudmNo ratings yet
- All-Industrial Rental Index Declines at An Increasing RateDocument6 pagesAll-Industrial Rental Index Declines at An Increasing Ratemaz_luthNo ratings yet
- Isoupdate March09Document20 pagesIsoupdate March09Sakthivel MurthyNo ratings yet
- SDS Conductivity Standard 15 μScm MSDS USDocument6 pagesSDS Conductivity Standard 15 μScm MSDS USMd. Firozur RahmanNo ratings yet
- Seizures and The Epilepsies in Infants, Children, and AdolescentsDocument8 pagesSeizures and The Epilepsies in Infants, Children, and AdolescentsCecille Ann CayetanoNo ratings yet
- Parkwayfit: Fitness Assessment ProgramDocument29 pagesParkwayfit: Fitness Assessment Programarief aceNo ratings yet
- Duxbury Clipper 06 - 17 - 2009Document44 pagesDuxbury Clipper 06 - 17 - 2009Duxbury ClipperNo ratings yet
- Tourism Eng - x5Document27 pagesTourism Eng - x5sanelisiwedywili473No ratings yet
- Consensus Statement On Vitamin D Status Assessment and Supplementation Whys, Whens, and HowsDocument30 pagesConsensus Statement On Vitamin D Status Assessment and Supplementation Whys, Whens, and HowsChanukya GvNo ratings yet
- LaxativesDocument19 pagesLaxativesNazia SalmanNo ratings yet
- Correlation of Chronological, Skeletal, and Dental Age in North Indian PopulationDocument8 pagesCorrelation of Chronological, Skeletal, and Dental Age in North Indian Populationcalmua1234No ratings yet