Download as pdf or txt
You might also like
- Coital Alignment TechniqueDocument2 pagesCoital Alignment Techniquenathan50% (6)
- Nursing Care Plan For HematuriaDocument2 pagesNursing Care Plan For HematuriaTee Wood63% (8)
- Assessment of Asymptomatic Microscopic Hematuria in AdultsDocument19 pagesAssessment of Asymptomatic Microscopic Hematuria in AdultsJood AL AbriNo ratings yet
- Hematuria em AdultosDocument10 pagesHematuria em AdultosalexandrecpcNo ratings yet
- Guidelines For UrologyDocument91 pagesGuidelines For UrologyAruna HarikrishnanNo ratings yet
- HMT 2020Document48 pagesHMT 2020Blesie AdvinculaNo ratings yet
- 2014.correlacion Citologia Tracto Urinario en Fresco y Con Tincion de PAP 1Document8 pages2014.correlacion Citologia Tracto Urinario en Fresco y Con Tincion de PAP 1analia9601No ratings yet
- Jurnal HematuriaDocument6 pagesJurnal HematuriaErlin IrawatiNo ratings yet
- HematuriaDocument4 pagesHematuriaArian SuryaNo ratings yet
- 2 Haematuria & Bladder CancerDocument37 pages2 Haematuria & Bladder Cancerallthingali217No ratings yet
- 2019-Urinary Tract CytologyDocument14 pages2019-Urinary Tract CytologyLucas Da SilvaNo ratings yet
- MGT Hematuria A+e.fullDocument7 pagesMGT Hematuria A+e.fullsarahisthedonNo ratings yet
- Genitourinary AssignmentDocument3 pagesGenitourinary AssignmentPal SedNo ratings yet
- Evaluation of HaematuriaDocument22 pagesEvaluation of HaematuriadamdooweNo ratings yet
- Stratifying Risk of Urinary Tract Malignant Tumors in Patients With Asymptomatic Microscopic HematuriaDocument10 pagesStratifying Risk of Urinary Tract Malignant Tumors in Patients With Asymptomatic Microscopic Hematuriavaibhav vinkareNo ratings yet
- Shen 2010Document6 pagesShen 2010Gangsar DamaiNo ratings yet
- Guidelines Hematuria de Nition and Screening Test MethodsDocument4 pagesGuidelines Hematuria de Nition and Screening Test MethodsTim Engineer HD RSUD Dr. SoetomoNo ratings yet
- The Diagnosis of Prostatitis: Category I ABPDocument4 pagesThe Diagnosis of Prostatitis: Category I ABPDaphne CelineNo ratings yet
- Jurnal Sitologi UrineDocument10 pagesJurnal Sitologi UrineAjip JenNo ratings yet
- The (Fixed) Urinary Sediment, A Simple and Useful Diagnostic Hematuria - CellfixDocument6 pagesThe (Fixed) Urinary Sediment, A Simple and Useful Diagnostic Hematuria - CellfixTatiane FernandesNo ratings yet
- Committee 3: Diagnostic Terminology: BackgroundDocument36 pagesCommittee 3: Diagnostic Terminology: BackgroundDaniel KurtyczNo ratings yet
- HematuriaDocument9 pagesHematuriaTel Avid YaredNo ratings yet
- Bladder Tumor Markers Beyond Cytology in PDFDocument29 pagesBladder Tumor Markers Beyond Cytology in PDFMariana CreciunNo ratings yet
- 10 0000@www Jrheum Org@32@5@828Document5 pages10 0000@www Jrheum Org@32@5@828Yasser AlghrafyNo ratings yet
- Chronic Prostatitis A Possible Cause of HematospermiaDocument6 pagesChronic Prostatitis A Possible Cause of HematospermiaZlatan ZvizdicNo ratings yet
- Mu 31Document4 pagesMu 31Lovkesh GoyalNo ratings yet
- Urothelial Marker - GU PDFDocument31 pagesUrothelial Marker - GU PDFDetty NoviantyNo ratings yet
- Page 4062693Document53 pagesPage 4062693alexandermarcusNo ratings yet
- Urinalysis and Urinary Tract Infection: Update For CliniciansDocument7 pagesUrinalysis and Urinary Tract Infection: Update For CliniciansGuneyden GuneydenNo ratings yet
- HematuriaDocument15 pagesHematurianisaw_2No ratings yet
- Cel Tumorales Mostoles 2008-CytopathologyDocument4 pagesCel Tumorales Mostoles 2008-CytopathologygemaNo ratings yet
- Ymj 60 174Document8 pagesYmj 60 174Jairo Lino BNo ratings yet
- 1856-Cian - The Role of Cytology in Urinalysis of Dogs and CaDocument4 pages1856-Cian - The Role of Cytology in Urinalysis of Dogs and CaYaiza Garcia CasadoNo ratings yet
- FollowDocument21 pagesFollowMCFNo ratings yet
- Uti Asbu Guidance FinalDocument14 pagesUti Asbu Guidance FinalJohn Vincent Dy OcampoNo ratings yet
- 1 s2.0 S2667008923000253 MainDocument4 pages1 s2.0 S2667008923000253 Mainal malikNo ratings yet
- The Paris System For Reporting Urinary CytologyDocument9 pagesThe Paris System For Reporting Urinary Cytologyrafasp.arqtNo ratings yet
- Bladder NCCNDocument17 pagesBladder NCCNJoriza TamayoNo ratings yet
- HematuriaDocument8 pagesHematuriaAby Medina RodríguezNo ratings yet
- Urine CytologyDocument15 pagesUrine CytologyNaruto ShikamaruNo ratings yet
- Guidelines For The Management of Abnormal Uterine Bleeding Guidelines For The Management of Abnormal Uterine BleedingDocument6 pagesGuidelines For The Management of Abnormal Uterine Bleeding Guidelines For The Management of Abnormal Uterine Bleedingyousef ibrahimNo ratings yet
- Marqueurs Tumoraux Et Surveillance KC VessieDocument16 pagesMarqueurs Tumoraux Et Surveillance KC VessienimaelhajjiNo ratings yet
- Revisión Del Carcinoma de Vesicula: Poster No.: Congress: Type: AuthorsDocument26 pagesRevisión Del Carcinoma de Vesicula: Poster No.: Congress: Type: AuthorsArturo García MarquezNo ratings yet
- Nuclear Medicine GuideDocument3 pagesNuclear Medicine GuidejeffsunilNo ratings yet
- Ascites MalignantDocument5 pagesAscites MalignantAlizaPinkyNo ratings yet
- 1-s2.0-S0378603X14000503-mainDocument8 pages1-s2.0-S0378603X14000503-mainAdam DanuartaNo ratings yet
- 114-Article Text-170-1-10-20180209Document6 pages114-Article Text-170-1-10-20180209Munazzah MehakNo ratings yet
- Renal Biopsy of Dogs and CatsDocument12 pagesRenal Biopsy of Dogs and CatsfrankyNo ratings yet
- Adult Nursing 2 Teaching PlanDocument5 pagesAdult Nursing 2 Teaching PlanJerilee SoCute WattsNo ratings yet
- Imaging in PediatricDocument25 pagesImaging in PediatricAlina MedrihanNo ratings yet
- Intl J Gynecology Obste - 2021 - BerekDocument25 pagesIntl J Gynecology Obste - 2021 - BerekKalaivathanan VathananNo ratings yet
- Annals of Medicine and Surgery: Uwe Scheuermann, Rizky Widyaningsih, Maria Hoppe-Lotichius, Michael Heise, Gerd OttoDocument7 pagesAnnals of Medicine and Surgery: Uwe Scheuermann, Rizky Widyaningsih, Maria Hoppe-Lotichius, Michael Heise, Gerd OttoClinton InfantNo ratings yet
- Blick 2011Document11 pagesBlick 2011nimaelhajjiNo ratings yet
- Prevalence of Variceal Bleeding in ALD PatientsDocument5 pagesPrevalence of Variceal Bleeding in ALD PatientsvarishNo ratings yet
- How To Evaluate Dipstick Hematuria CCJM 2008Document7 pagesHow To Evaluate Dipstick Hematuria CCJM 2008CANELO_PIANONo ratings yet
- Sensitivity and Specificity Analysis of Urine nmp22 Cytokeratin18 Ca 199 and Cytology For Diagnosing Bladder Malignancy 1103Document4 pagesSensitivity and Specificity Analysis of Urine nmp22 Cytokeratin18 Ca 199 and Cytology For Diagnosing Bladder Malignancy 1103sagaNo ratings yet
- Effects of Transurethral Resection of Prostate On Flow Rate and Voided Volume On Patients With Benign Prostatic HyperplasiaDocument4 pagesEffects of Transurethral Resection of Prostate On Flow Rate and Voided Volume On Patients With Benign Prostatic HyperplasiaKamran AfzalNo ratings yet
- Adult Urology: ElsevierDocument6 pagesAdult Urology: Elsevierderr barrNo ratings yet
- Philippine Clinical Practice Guidelines On The Diagnosis andDocument83 pagesPhilippine Clinical Practice Guidelines On The Diagnosis andREnren ConsolNo ratings yet
- Imaging of the Liver and Intra-hepatic Biliary Tract: Volume 2: Tumoral PathologiesFrom EverandImaging of the Liver and Intra-hepatic Biliary Tract: Volume 2: Tumoral PathologiesNo ratings yet
- Lower Genital Tract Precancer: Colposcopy, Pathology and TreatmentFrom EverandLower Genital Tract Precancer: Colposcopy, Pathology and TreatmentNo ratings yet
- Fast Facts: Cholangiocarcinoma: Diagnostic and therapeutic advances are improving outcomesFrom EverandFast Facts: Cholangiocarcinoma: Diagnostic and therapeutic advances are improving outcomesNo ratings yet
- Evaluation of Laboratory Measurements For Clinical Assessment of Kidney Disease - DOQIDocument35 pagesEvaluation of Laboratory Measurements For Clinical Assessment of Kidney Disease - DOQIErnestoNo ratings yet
- Tubulointerstitial Renal Disease - Curr Opin Nephrol HypertenDocument11 pagesTubulointerstitial Renal Disease - Curr Opin Nephrol HypertenErnestoNo ratings yet
- The Persistently Troublesome Cough - Am J Respir Crit Care Med 2002Document6 pagesThe Persistently Troublesome Cough - Am J Respir Crit Care Med 2002ErnestoNo ratings yet
- Diagnosis and Treatment of Cough - N Engl J Med 2000Document7 pagesDiagnosis and Treatment of Cough - N Engl J Med 2000ErnestoNo ratings yet
- Mechanisms of Platypnea-Orthodeoxia. What Causes Water To Flow Uphill - Circulation 2002Document2 pagesMechanisms of Platypnea-Orthodeoxia. What Causes Water To Flow Uphill - Circulation 2002ErnestoNo ratings yet
- Controversies in The Evaluation and Management of Chronic Cough - Am J Respir Crit Care Med 2011Document8 pagesControversies in The Evaluation and Management of Chronic Cough - Am J Respir Crit Care Med 2011ErnestoNo ratings yet
- Diagnostic Value of The Physical Examination in Patients With Dyspnea - Cleve Clin J Med 2017Document9 pagesDiagnostic Value of The Physical Examination in Patients With Dyspnea - Cleve Clin J Med 2017ErnestoNo ratings yet
- Cardiopulmonary Laboratory Biomarkers in The Evaluation of Acute Dyspnea - Open Acces Emerg Med 2016Document11 pagesCardiopulmonary Laboratory Biomarkers in The Evaluation of Acute Dyspnea - Open Acces Emerg Med 2016ErnestoNo ratings yet
- 2002, Feb - Persistence of The Prothrombotic State After Acute Coronary Syndromes Implications For TreatmentDocument12 pages2002, Feb - Persistence of The Prothrombotic State After Acute Coronary Syndromes Implications For TreatmentErnestoNo ratings yet
- Ayush 231553Document4 pagesAyush 231553swaroop24x7No ratings yet
- Anatomy GuDocument13 pagesAnatomy Gujefel umarNo ratings yet
- Bahasa Inggris Role Play Review Anatomi Fisiologi ManusiaDocument5 pagesBahasa Inggris Role Play Review Anatomi Fisiologi Manusianono NonoNo ratings yet
- 2023 Pca CV Expert Panel Virtual Meeting - Pre-ReadDocument48 pages2023 Pca CV Expert Panel Virtual Meeting - Pre-ReadPashoKiatNo ratings yet
- Phimosis and ParaphimosisDocument3 pagesPhimosis and ParaphimosisJoshua PowersNo ratings yet
- Imaging in Genitourinary SystemDocument36 pagesImaging in Genitourinary SystemAlkaustariyah LubisNo ratings yet
- Incremental and TwiceDocument12 pagesIncremental and TwiceAgung KaryawinaraNo ratings yet
- Results and Discussions: Condom Distribution Among Grade 11 Students in DEGMNHS S.Y. 2016-2017Document37 pagesResults and Discussions: Condom Distribution Among Grade 11 Students in DEGMNHS S.Y. 2016-2017John OpeñaNo ratings yet
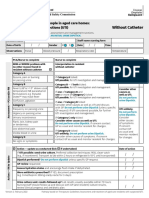
- Form Ams Clinical Pathway Fillable Form Without CatheterDocument1 pageForm Ams Clinical Pathway Fillable Form Without CatheterTeenu JobyNo ratings yet
- Koas - Farmakoterapi ISKDocument37 pagesKoas - Farmakoterapi ISKRIFATUL ISLAMIYAHNo ratings yet
- Best Orthopedic Specialist Surgeon Clinic & Doctor in MumbaiDocument40 pagesBest Orthopedic Specialist Surgeon Clinic & Doctor in Mumbaipranjal kodkaniNo ratings yet
- Prune Belly SyndromeDocument39 pagesPrune Belly SyndromeHudaNo ratings yet
- BPH Guideline 2019Document10 pagesBPH Guideline 2019Nun AdeninNo ratings yet
- MatchDocument52 pagesMatchYihalemNo ratings yet
- Complications of Transurethral Resection of Prostate (Turp)Document8 pagesComplications of Transurethral Resection of Prostate (Turp)Agung IndraNo ratings yet
- Continuous Bladder IrrigationDocument13 pagesContinuous Bladder IrrigationMichelle Migrino PachoNo ratings yet
- SMS Hospital Jaipur OPD Doctor List: Name Department QualificationDocument5 pagesSMS Hospital Jaipur OPD Doctor List: Name Department QualificationBhupender SainiNo ratings yet
- Embryology of Urinary SystemDocument4 pagesEmbryology of Urinary SystemZllison Mae Teodoro MangabatNo ratings yet
- Ceklist Februari 2015 Team Jakarta 2.irpanDocument75 pagesCeklist Februari 2015 Team Jakarta 2.irpanIrwan DonyNo ratings yet
- C 39Document8 pagesC 39Tammie Gore100% (2)
- Latihan Soal MCQ UrologiDocument43 pagesLatihan Soal MCQ Urologidytul100% (1)
- English For Doctors Customer BookletDocument23 pagesEnglish For Doctors Customer BookletFrugeo GRI Limited70% (10)
- Kinking of The Lower UreterDocument2 pagesKinking of The Lower UreterDella Rimawati HarismaNo ratings yet
- Differential Diagnosis UrolithiasisDocument10 pagesDifferential Diagnosis UrolithiasisAldila Rc X ManiaNo ratings yet
- mcq renalفاطمه جاسم محمدDocument4 pagesmcq renalفاطمه جاسم محمدFatema Al-KananiNo ratings yet
- 3 Anatomy and Physiology (Male)Document18 pages3 Anatomy and Physiology (Male)AYO NELSONNo ratings yet
- 15 UrinalysisDocument9 pages15 UrinalysisJaney Ceniza تNo ratings yet
- UroLap 2.0 - BrochureDocument3 pagesUroLap 2.0 - Brochurehindi channelNo ratings yet