Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Maths No ProblemDocument14 pagesMaths No ProblemJamila Mammadova100% (2)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Pubs HPE OmniStack 4 1 3 For Vsphere Upgrade GuideDocument63 pagesPubs HPE OmniStack 4 1 3 For Vsphere Upgrade GuideYeraldo MarinNo ratings yet
- Personal Protective Equipment (Ppe) Inspection Checklist: Safety HelmetDocument1 pagePersonal Protective Equipment (Ppe) Inspection Checklist: Safety Helmetvini100% (3)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Bachelor of Nursing Science With HonoursDocument12 pagesBachelor of Nursing Science With HonoursviniNo ratings yet
- SH-F43 - PTW Format - R02Document2 pagesSH-F43 - PTW Format - R02vini100% (1)
- SH-F05 - Induction FormDocument1 pageSH-F05 - Induction FormviniNo ratings yet
- Template Take Home ExaminationDocument9 pagesTemplate Take Home ExaminationviniNo ratings yet
- SH-F35 - Site Safety Inspection - ToolsDocument1 pageSH-F35 - Site Safety Inspection - ToolsviniNo ratings yet
- Sample Format Worker NamelistDocument1 pageSample Format Worker NamelistviniNo ratings yet
- SH-F17 - First Aid InspectionDocument2 pagesSH-F17 - First Aid InspectionviniNo ratings yet
- Critical Thinking Edisi ForumDocument24 pagesCritical Thinking Edisi ForumviniNo ratings yet
- PRO410 Traffic ManagementDocument15 pagesPRO410 Traffic ManagementviniNo ratings yet
- Covid Safety SOPDocument2 pagesCovid Safety SOPviniNo ratings yet
- Mcentura 18 May 2020: 1) Transformer RoomDocument3 pagesMcentura 18 May 2020: 1) Transformer RoomviniNo ratings yet
- Reflective Report Entrepreneurship 2Document2 pagesReflective Report Entrepreneurship 2viniNo ratings yet
- Assignment/ Tugasan - Basic Security ManagementDocument8 pagesAssignment/ Tugasan - Basic Security ManagementviniNo ratings yet
- 04 Xbos3103 CGDocument6 pages04 Xbos3103 CGviniNo ratings yet
- Ergonomics-Guideline - Workstation Ergonomic GuidelinesDocument5 pagesErgonomics-Guideline - Workstation Ergonomic GuidelinesviniNo ratings yet
- Covid-19: Social Distancing Guidelines For Workplace, Homes and IndividualsDocument4 pagesCovid-19: Social Distancing Guidelines For Workplace, Homes and IndividualsviniNo ratings yet
- PTW Tracking Log: Allied Engineering Construction Sdn. Bhd. Urc Engineering Sdn. BHDDocument1 pagePTW Tracking Log: Allied Engineering Construction Sdn. Bhd. Urc Engineering Sdn. BHDviniNo ratings yet
- Employers Views On Importance of English ProficieDocument13 pagesEmployers Views On Importance of English ProficieviniNo ratings yet
- Diabetic Control Using Genetic Fuzzy-PI ControllerDocument7 pagesDiabetic Control Using Genetic Fuzzy-PI ControllerIndana Firdausi NuzulaNo ratings yet
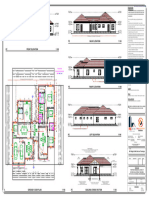
- MR Regis N MRS Dorcas Taruvinga - 050209Document1 pageMR Regis N MRS Dorcas Taruvinga - 050209pzarchitectural99No ratings yet
- Presented By: Thermistor - Fan Speed Control Using LabviewDocument16 pagesPresented By: Thermistor - Fan Speed Control Using LabviewKomal ZalwarNo ratings yet
- Kunci-Jawaban Howard AntonDocument41 pagesKunci-Jawaban Howard AntonAlyagariniNo ratings yet
- CHEM1 Chapter 2 - MeasurementDocument147 pagesCHEM1 Chapter 2 - MeasurementRomalyn GalinganNo ratings yet
- Indian ClimateDocument7 pagesIndian ClimatePrakash Kumar Kumar100% (1)
- SchizophreniaDocument39 pagesSchizophreniaChikezie OnwukweNo ratings yet
- Title of The Paper: (Font: Arial 14Pts)Document3 pagesTitle of The Paper: (Font: Arial 14Pts)RN Builder IpohNo ratings yet
- Ake PH3 00 Par DWG SW 55002Document1 pageAke PH3 00 Par DWG SW 55002JericFuentesNo ratings yet
- Learn To Use Microsoft Word 2016Document385 pagesLearn To Use Microsoft Word 2016Íthalo Santana100% (2)
- Report Evaporator Sculptor Behr 120405Document11 pagesReport Evaporator Sculptor Behr 120405gosculptorNo ratings yet
- Some Remarks On Fuzzy N-Normed SpacesDocument7 pagesSome Remarks On Fuzzy N-Normed SpacesRyanEliasNo ratings yet
- Service Manual: DSC-F505VDocument34 pagesService Manual: DSC-F505VAnonymous Lfgk6vygNo ratings yet
- Strategic Intent Envisioning and MissionDocument23 pagesStrategic Intent Envisioning and Mission14122001riya2001No ratings yet
- Applied Economics Module 1Document30 pagesApplied Economics Module 1愛結No ratings yet
- Cono Rc-45-Ii, Serie 52378Document50 pagesCono Rc-45-Ii, Serie 52378omar muñoz100% (1)
- Diasporic Writing QuestionsDocument31 pagesDiasporic Writing QuestionsMEIMOONA HUSNAIN100% (1)
- Remembering The Father of Indian Constitution - Dr. B R Ambedkar and His Role in Framing Indian ConstitutionDocument7 pagesRemembering The Father of Indian Constitution - Dr. B R Ambedkar and His Role in Framing Indian ConstitutionEditor IJTSRDNo ratings yet
- Sky Star 300Document2 pagesSky Star 300Onitry RecordNo ratings yet
- Controllogix FestoDocument43 pagesControllogix FestoEdwin Ramirez100% (1)
- Science X QP Set BDocument7 pagesScience X QP Set BYogesh KhannaNo ratings yet
- Huawei HCIA-AI V3.0 Certification ExamDocument3 pagesHuawei HCIA-AI V3.0 Certification ExamAbraham MogosNo ratings yet
- HOPE 12 Budget of WorkDocument2 pagesHOPE 12 Budget of WorkRonald Francis Sanchez VirayNo ratings yet
- E. TABLE OF CONTENTSDocument9 pagesE. TABLE OF CONTENTSAlexa Nicole GayosoNo ratings yet
- Acedemic Integrity AssignmentDocument3 pagesAcedemic Integrity Assignmentapi-308899749No ratings yet
- Iit Jee (Links)Document5 pagesIit Jee (Links)Tarun MankadNo ratings yet
- Process Design and Economics For The Conversion of The Lignocellulosic To HydrocarbonsDocument133 pagesProcess Design and Economics For The Conversion of The Lignocellulosic To HydrocarbonsCristhian Camilo Vargas QuinteroNo ratings yet
- QuestionDocument4 pagesQuestionKira NguyễnNo ratings yet