Download as pdf or txt
You might also like
- Internal Medicine: Over 200 Case StudiesFrom EverandInternal Medicine: Over 200 Case StudiesRating: 4.5 out of 5 stars4.5/5 (18)
- Sertifikat Webinar Halodoc Diagnosis and Neurotropic Vitamines in Neuropathy - Clinical Pearls - Dr. Ismail MarzukiDocument1 pageSertifikat Webinar Halodoc Diagnosis and Neurotropic Vitamines in Neuropathy - Clinical Pearls - Dr. Ismail Marzukidr. Ukie Hasibuan100% (1)
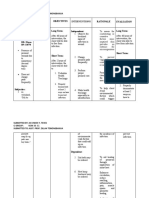
- Alcohol Withdrawal Care PlanDocument1 pageAlcohol Withdrawal Care PlanVanessaMUeller100% (1)
- Geriatric Practice PDFDocument558 pagesGeriatric Practice PDFGemmita Trujillo100% (9)
- Teves, J. Owen NCP Risk For Infection R:T Episiotomy WoundDocument3 pagesTeves, J. Owen NCP Risk For Infection R:T Episiotomy WoundJoi Owen Teves100% (2)
- Types of Special NeedsDocument9 pagesTypes of Special NeedsThangaraj Msw100% (1)
- Management of Neurologic ConditionsDocument193 pagesManagement of Neurologic ConditionsAnna ReyesNo ratings yet
- NeurologyDocument37 pagesNeurologyDevangkumar PatelNo ratings yet
- Headache: Rosen's Chapters 17 and 105 November 9, 2006 by George FiliadisDocument45 pagesHeadache: Rosen's Chapters 17 and 105 November 9, 2006 by George Filiadisradiologi igdNo ratings yet
- HeadacheDocument92 pagesHeadacheMilap Shah100% (1)
- Medicine 1Document109 pagesMedicine 1Itinderpal SinghNo ratings yet
- Hypertensive Encwphalopathy 1Document25 pagesHypertensive Encwphalopathy 1saldy meirisandyNo ratings yet
- Medicine - Riley HarrisonDocument106 pagesMedicine - Riley HarrisonFiras AliNo ratings yet
- Headache: Assoc Professor Dr. VinothiniDocument27 pagesHeadache: Assoc Professor Dr. VinothiniVivienneNo ratings yet
- Ischemic Cardiac DiseaseDocument34 pagesIschemic Cardiac DiseaseGopala HariNo ratings yet
- HeadacheDocument36 pagesHeadacheabenezer g/kirstosNo ratings yet
- Headache: Rosen's Chapters 17 and 105 November 9, 2006 by George FiliadisDocument45 pagesHeadache: Rosen's Chapters 17 and 105 November 9, 2006 by George Filiadishemanthshah2801No ratings yet
- Cerebrovascular Disease (Autosaved)Document83 pagesCerebrovascular Disease (Autosaved)Henry BonaNo ratings yet
- Headache: An Overview: Danish Ejaz BhattiDocument43 pagesHeadache: An Overview: Danish Ejaz BhattiPGHCNo ratings yet
- 5 - HeadacheDocument11 pages5 - HeadacheRawabi rawabi1997No ratings yet
- MIGRAINE Neurovision 2019Document40 pagesMIGRAINE Neurovision 2019Bagadi SuneelNo ratings yet
- Pharma Act 2 FinalDocument29 pagesPharma Act 2 Finalrofaida.omar40No ratings yet
- CT ScanLesson VIDocument60 pagesCT ScanLesson VILalaine De JesusNo ratings yet
- Approach To The Patient With Headache and Facial PainDocument25 pagesApproach To The Patient With Headache and Facial Painfaza ghaniNo ratings yet
- Headache and Facial PainDocument81 pagesHeadache and Facial PainΖέτα ΤσίρκαNo ratings yet
- Head Trauma: Dr. Andy Wijaya, SpemDocument20 pagesHead Trauma: Dr. Andy Wijaya, SpemThomas AlbertNo ratings yet
- Pharm Care in Stroke-1Document45 pagesPharm Care in Stroke-1Achmad Triwidodo AmoeNo ratings yet
- SAH RevisedDocument41 pagesSAH RevisedZari NovelaNo ratings yet
- A. Severe Migraine Attack B. Cluster Headache C. Subarachnoid Hemorrhage D. Hypertensive Encephalopathy E. EncephalitisDocument4 pagesA. Severe Migraine Attack B. Cluster Headache C. Subarachnoid Hemorrhage D. Hypertensive Encephalopathy E. EncephalitisVgdgNo ratings yet
- Pharm Stroke: Care PadaDocument38 pagesPharm Stroke: Care PadaDimas RfNo ratings yet
- HypertensionDocument8 pagesHypertensionaraNo ratings yet
- Updated Headache 21-22Document48 pagesUpdated Headache 21-22jwxxi11No ratings yet
- 4th Problem Emergency Medicine Group 1Document82 pages4th Problem Emergency Medicine Group 1Jonathan TandajuNo ratings yet
- Headache - Approach To The Adult PatientDocument52 pagesHeadache - Approach To The Adult PatientfjnaressiNo ratings yet
- Nasta Pemicu 1 Gawat DaruratDocument21 pagesNasta Pemicu 1 Gawat DaruratThediDarmaWijayaNo ratings yet
- Pemicu 1: Yinvill 405120025 Kelompok 8Document99 pagesPemicu 1: Yinvill 405120025 Kelompok 8yinvilllNo ratings yet
- MigraineDocument30 pagesMigraineFathimathNo ratings yet
- Neurology SlidesDocument38 pagesNeurology Slidesdrmalsharrakhi_32794100% (1)
- Review NeuroDocument48 pagesReview NeuroNefrologia SamaritanaNo ratings yet
- Headache OverviewDocument29 pagesHeadache OverviewFiqna SyaniNo ratings yet
- HTN - Emerg EDDocument37 pagesHTN - Emerg EDAyesh EKNo ratings yet
- Farmakoterapi StrokeDocument33 pagesFarmakoterapi StrokeMuhammad Aldi SetiawanNo ratings yet
- Unit 2 Anti Migraine and Drugs For Trigeminal Neuralgia Pharmacy-IIDocument38 pagesUnit 2 Anti Migraine and Drugs For Trigeminal Neuralgia Pharmacy-IIAsad MirajNo ratings yet
- HY NeuroDocument22 pagesHY Neurojulia.e.c.uclaNo ratings yet
- NPLEX Combination Review Neurology - C: Paul S. Anderson, ND Medical Board Review ServicesDocument46 pagesNPLEX Combination Review Neurology - C: Paul S. Anderson, ND Medical Board Review ServicesValeria AcevedoNo ratings yet
- Medical Problems in DentistryDocument13 pagesMedical Problems in DentistryعصامالعبيديNo ratings yet
- Cefaleas 2018Document87 pagesCefaleas 2018Anonimo DesconocidoNo ratings yet
- Headac HE: Chapter 21, Harrison'S Internal MedicineDocument21 pagesHeadac HE: Chapter 21, Harrison'S Internal MedicineFernando AnibanNo ratings yet
- Sunkara DB Neurological DisordersDocument41 pagesSunkara DB Neurological DisordersAngela SaoNo ratings yet
- Materi Ppds Prep Stroke, Vertigo, ImagingDocument106 pagesMateri Ppds Prep Stroke, Vertigo, Imagingintanurpratiwi4No ratings yet
- Case Based Presentation: Hypertension in The ICU: by Noemie Chessex and Colleagues UBCDocument52 pagesCase Based Presentation: Hypertension in The ICU: by Noemie Chessex and Colleagues UBCmabs_LVNo ratings yet
- Pemicu 4 Saraf - VeniaDocument42 pagesPemicu 4 Saraf - Veniavenia endah tamaraNo ratings yet
- Disease Study: A. Myasthenia GravisDocument6 pagesDisease Study: A. Myasthenia GravisMark Lemuel AbadaNo ratings yet
- Headache: Dep. of Neurology, General Hospital of Ningxia Medical University Cell Phone:13709599000Document50 pagesHeadache: Dep. of Neurology, General Hospital of Ningxia Medical University Cell Phone:13709599000ArvindhanNo ratings yet
- Meningitis TBDocument10 pagesMeningitis TBSiq Febri SmnjtkNo ratings yet
- Headache NotesDocument25 pagesHeadache NotesAin AmanyNo ratings yet
- Sistim EkstrapiramidalDocument44 pagesSistim EkstrapiramidaljanaNo ratings yet
- Online Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreDocument112 pagesOnline Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreabctutorNo ratings yet
- Stroke and Spinal Cord 7 30Document39 pagesStroke and Spinal Cord 7 30Dr. Swarup DasNo ratings yet
- Neurology Review: Omar K. MRCP Ireland 2015Document58 pagesNeurology Review: Omar K. MRCP Ireland 2015Manmeet SNo ratings yet
- Headache Neuroimaging FinalDocument85 pagesHeadache Neuroimaging Finaldinesh kumarNo ratings yet
- Arrhythmia 6 YrDocument72 pagesArrhythmia 6 YrPiyush MalikNo ratings yet
- Medicine 2e Sample PagesDocument18 pagesMedicine 2e Sample PagesScholastica ChinazoNo ratings yet
- Chapter 62 Stroke Study GuideDocument4 pagesChapter 62 Stroke Study GuideValerie BarrNo ratings yet
- Neurology Equations Made Simple: Differential Diagnosis and NeuroemergenciesFrom EverandNeurology Equations Made Simple: Differential Diagnosis and NeuroemergenciesNo ratings yet
- PR Obat PT. DSSP Power Sumsel September 2022Document34 pagesPR Obat PT. DSSP Power Sumsel September 2022dr. Ukie HasibuanNo ratings yet
- Safety Helmet Color MOADocument1 pageSafety Helmet Color MOAdr. Ukie HasibuanNo ratings yet
- Form Nama PCR Test Pt. SupracoDocument1 pageForm Nama PCR Test Pt. Supracodr. Ukie HasibuanNo ratings yet
- DSSP-S05-HSE-FM-0071 Checklist For Outsourcing Service WorkDocument1 pageDSSP-S05-HSE-FM-0071 Checklist For Outsourcing Service Workdr. Ukie HasibuanNo ratings yet
- KTP & Vaksin Kloter 1Document3 pagesKTP & Vaksin Kloter 1dr. Ukie HasibuanNo ratings yet
- Materi Fire Rescue BagDocument3 pagesMateri Fire Rescue Bagdr. Ukie HasibuanNo ratings yet
- Inhouse Visit ChecklistDocument7 pagesInhouse Visit Checklistdr. Ukie HasibuanNo ratings yet
- 1 - Form Site Leaving PermitDocument2 pages1 - Form Site Leaving Permitdr. Ukie HasibuanNo ratings yet
- Form Nama Rapid Test Pt. PpsDocument1 pageForm Nama Rapid Test Pt. Ppsdr. Ukie HasibuanNo ratings yet
- Drawing FutsalDocument1 pageDrawing Futsaldr. Ukie HasibuanNo ratings yet
- PR Obat IHC DSSP Power Sumsel V November 2020Document84 pagesPR Obat IHC DSSP Power Sumsel V November 2020dr. Ukie HasibuanNo ratings yet
- Webinar Diabetes PDFDocument2 pagesWebinar Diabetes PDFdr. Ukie HasibuanNo ratings yet
- Effects of Bimanual Functional Practice Training On Functional Performance of Upper Extremity in Chronic Stroke SRJI Vol 2 Issue 3 Year 2013Document10 pagesEffects of Bimanual Functional Practice Training On Functional Performance of Upper Extremity in Chronic Stroke SRJI Vol 2 Issue 3 Year 2013Dr. Krishna N. SharmaNo ratings yet
- Introduction To Medtech NotesDocument44 pagesIntroduction To Medtech NotesJanelle RemorozaNo ratings yet
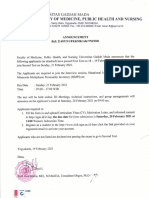
- Announcement First Test IUP FKKMK 1Document7 pagesAnnouncement First Test IUP FKKMK 1Razan WieansahNo ratings yet
- Renal Failure Nursing Care PlanDocument2 pagesRenal Failure Nursing Care Planemman_abz33% (3)
- Pneumonia CBLDocument22 pagesPneumonia CBLImAlien OrGodNo ratings yet
- Laboratory Corporation of AmericaDocument156 pagesLaboratory Corporation of AmericaJohn CollinsNo ratings yet
- Powerpoint - Prof Suzanne KurtzDocument80 pagesPowerpoint - Prof Suzanne Kurtzlizleeas100% (1)
- Efficacy of Homoeopathy in SarcoidosisDocument77 pagesEfficacy of Homoeopathy in SarcoidosisDr. Rajneesh Kumar Sharma MD HomNo ratings yet
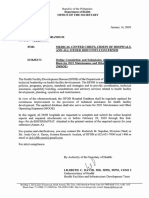
- 2021 Budget Mooe GuidelinesDocument11 pages2021 Budget Mooe GuidelinesWilbert Reuyan100% (2)
- A Drug Study On: Furosemide TabletDocument7 pagesA Drug Study On: Furosemide TabletRaijenne VersolaNo ratings yet
- Chameli Devi Group of Institutions, IndoreDocument13 pagesChameli Devi Group of Institutions, IndoreVinay ProjectNo ratings yet
- Emphysema PDFDocument52 pagesEmphysema PDFrigobertoguerragNo ratings yet
- Extracellular Vimentin Mimics VEGF and Is A Target For Anti-Angiogenic ImmunotherapyDocument20 pagesExtracellular Vimentin Mimics VEGF and Is A Target For Anti-Angiogenic ImmunotherapyElse HuijbersNo ratings yet
- 1 List Signals Discussed Prac September 2012 enDocument60 pages1 List Signals Discussed Prac September 2012 enAmany HagageNo ratings yet
- Q.P Code: 544222Document16 pagesQ.P Code: 544222وليد خالدNo ratings yet
- Jisha New CV Final 2Document5 pagesJisha New CV Final 2Mary JisNo ratings yet
- LaryngitisDocument24 pagesLaryngitisfatihahannisahumaira100% (1)
- Rational Use of AntibioticsDocument85 pagesRational Use of AntibioticsAHMAD MAHIR BIN CHE RAHMATNo ratings yet
- Ciad 696Document10 pagesCiad 696vsjsqz97nrNo ratings yet
- Instant Download Economics of Money Banking and Financial Markets Canadian 6th Edition Mishkin Solutions Manual PDF Full ChapterDocument33 pagesInstant Download Economics of Money Banking and Financial Markets Canadian 6th Edition Mishkin Solutions Manual PDF Full Chapternhattranel7k1100% (7)
- NCPDocument2 pagesNCPczeremar chanNo ratings yet
- Ruggiero - The Cooperation of Physicians and The State in The Control of Violence in Renaissance VeDocument11 pagesRuggiero - The Cooperation of Physicians and The State in The Control of Violence in Renaissance Veboogeeleey voogeeleyNo ratings yet
- Guideline Variceal BleedingDocument18 pagesGuideline Variceal BleedingLuh Putu Swastiyani Purnami, M.DNo ratings yet
- Haemodynamic Monitoring: WWW - Vygon.co - UkDocument12 pagesHaemodynamic Monitoring: WWW - Vygon.co - UkJuita yuliarniNo ratings yet
- Pharmaceutical ExcipientsDocument5 pagesPharmaceutical Excipientsmads56091No ratings yet
- CPA TheValueOfPhysio2012 ICU-V1Document2 pagesCPA TheValueOfPhysio2012 ICU-V1Miguel Andrés Campos DiazNo ratings yet