Download as pdf or txt
You might also like
- Performance Evaluation (Intra-Partal)Document5 pagesPerformance Evaluation (Intra-Partal)PWEPWEE DIEDIEPIEENo ratings yet
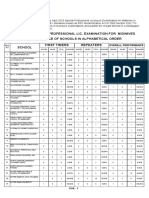
- April 2023 Special Professional Lic. Examination For MidwivesDocument2 pagesApril 2023 Special Professional Lic. Examination For MidwivesRapplerNo ratings yet
- FC OB July 2021Document13 pagesFC OB July 2021Johnmer Avelino100% (1)
- Biology Project IndexDocument3 pagesBiology Project Indexmansi60% (5)
- Objective Definition of Shoulder Dystocia: A Prospective EvaluationDocument4 pagesObjective Definition of Shoulder Dystocia: A Prospective Evaluationbahtiar bleachNo ratings yet
- International Journal of Health Sciences and Research: Fetal Umbilical Cord Circumference Measurement and Birth WeightDocument6 pagesInternational Journal of Health Sciences and Research: Fetal Umbilical Cord Circumference Measurement and Birth WeightFatma ElzaytNo ratings yet
- Fetal Growth Velocity in Diabetics and The Risk For Shoulder Dystocia: A Case-Control StudyDocument6 pagesFetal Growth Velocity in Diabetics and The Risk For Shoulder Dystocia: A Case-Control Studyaulia ilmaNo ratings yet
- Bo Fill 1997Document5 pagesBo Fill 1997Sarly FebrianaNo ratings yet
- Maternal Pre-Pregnancy Obesity and The Risk of Shoulder Dystocia: A Meta-AnalysisDocument29 pagesMaternal Pre-Pregnancy Obesity and The Risk of Shoulder Dystocia: A Meta-Analysisaulia ilmaNo ratings yet
- Singleton Term Breech Deliveries in Nulliparous and Multiparous Women: A 5-Year Experience at The University of Miami/Jackson Memorial HospitalDocument6 pagesSingleton Term Breech Deliveries in Nulliparous and Multiparous Women: A 5-Year Experience at The University of Miami/Jackson Memorial HospitalSarah SilaenNo ratings yet
- Newborn Shoulder Width: Prospective Study Consecutive MeasurementsDocument5 pagesNewborn Shoulder Width: Prospective Study Consecutive MeasurementsLucas Daniel SmithNo ratings yet
- Articulo 5Document6 pagesArticulo 5Monica ReyesNo ratings yet
- Development and Validation of A Machine Learning Model For Prediction ofDocument9 pagesDevelopment and Validation of A Machine Learning Model For Prediction ofFahira RizkyNo ratings yet
- Jurnal ObstetriDocument7 pagesJurnal ObstetrikoasimutNo ratings yet
- Mir Ghani 2006Document4 pagesMir Ghani 2006Sarly FebrianaNo ratings yet
- CHSJ 47 04 10 2021Document6 pagesCHSJ 47 04 10 2021mihail.boldeanuNo ratings yet
- JBR 26 04 235Document6 pagesJBR 26 04 235Khuriyatun NadhifahNo ratings yet
- Original Article Symphysio Fundal Height (SFH) Measurement As A Predictor of Birth WeightDocument5 pagesOriginal Article Symphysio Fundal Height (SFH) Measurement As A Predictor of Birth Weightyudha adi saputaNo ratings yet
- Jurnal PerinaDocument7 pagesJurnal PerinaBhismo PasetyoNo ratings yet
- Estimated Fetal Weight: Comparison of Clinical Versus Ultrasound EstimateDocument6 pagesEstimated Fetal Weight: Comparison of Clinical Versus Ultrasound EstimateNadia AyuningtiasNo ratings yet
- The Interactive Effect of Prepregnancy Overweight/Obesity and Isolated Maternal Hypothyroxinemia On MacrosomiaDocument8 pagesThe Interactive Effect of Prepregnancy Overweight/Obesity and Isolated Maternal Hypothyroxinemia On MacrosomiaAndres GallegosNo ratings yet
- WHO - Um Interventions For Preventing Shoulder DystociaDocument4 pagesWHO - Um Interventions For Preventing Shoulder Dystociavishramki2009No ratings yet
- Preterm Birth by Vacuum Extraction and Neonatal Outcome: A Population-Based Cohort StudyDocument9 pagesPreterm Birth by Vacuum Extraction and Neonatal Outcome: A Population-Based Cohort StudypfannenstielNo ratings yet
- Crecimiento y Desarrollo FetalDocument16 pagesCrecimiento y Desarrollo Fetalalejandra mejia jimenezNo ratings yet
- Ehrenkranz 1999Document12 pagesEhrenkranz 1999amyNo ratings yet
- Diabetic MaternlaDocument4 pagesDiabetic MaternlaAde Gustina SiahaanNo ratings yet
- Shoulder DystociaDocument9 pagesShoulder DystociaRorschach VargasNo ratings yet
- Lee Et Al-2016-BJOG An International Journal of Obstetrics & GynaecologyDocument8 pagesLee Et Al-2016-BJOG An International Journal of Obstetrics & GynaecologyDhia UlfajriNo ratings yet
- Short Stature Is Associated With An Increased Risk of Caesarean Deliveries in Low Risk PopulationDocument6 pagesShort Stature Is Associated With An Increased Risk of Caesarean Deliveries in Low Risk PopulationManangioma ManNo ratings yet
- Shoulder Dystocia: Risk Factors, Predictability, and PreventabilityDocument5 pagesShoulder Dystocia: Risk Factors, Predictability, and PreventabilityDaniel Ramirez QuintanaNo ratings yet
- RiskfactorretainedplacentaDocument9 pagesRiskfactorretainedplacentaDONNYNo ratings yet
- 07 Eo - 16 00005Document6 pages07 Eo - 16 00005Lenin GutierrezNo ratings yet
- Risk Factors and Outcomes of Fetal Macrosomia in A Tertiary Centre in Tanzania: A Case-Control StudyDocument8 pagesRisk Factors and Outcomes of Fetal Macrosomia in A Tertiary Centre in Tanzania: A Case-Control StudyMarianella Saravia LopezNo ratings yet
- Thenewfriedmancurve PDFDocument5 pagesThenewfriedmancurve PDFreioctabianoNo ratings yet
- Epidemiology of Inguinal Hernia in Preterm Neonates: ResultsDocument4 pagesEpidemiology of Inguinal Hernia in Preterm Neonates: ResultsGokull ShautriNo ratings yet
- Malaria in Pregnancy: The Difficulties in Measuring BirthweightDocument8 pagesMalaria in Pregnancy: The Difficulties in Measuring BirthweightEffika YuliaNo ratings yet
- Fracture of The Clavicle in The Newborn Following Normal Labor and DeliveryDocument6 pagesFracture of The Clavicle in The Newborn Following Normal Labor and DeliveryAlberto OrtizNo ratings yet
- The Impact of Maternal Body Mass Index On The Phenotype of Pre-Eclampsia: A Prospective Cohort StudyDocument7 pagesThe Impact of Maternal Body Mass Index On The Phenotype of Pre-Eclampsia: A Prospective Cohort StudyAchmad Deza FaristaNo ratings yet
- Pi Is 0002937813006170Document7 pagesPi Is 0002937813006170Raisa AriesthaNo ratings yet
- Anthropometric Measurements at Birth As Predictor of Low Birth Weight PDFDocument5 pagesAnthropometric Measurements at Birth As Predictor of Low Birth Weight PDFPeregrine Albertus Ricco AzaliNo ratings yet
- The Macrosomic Fetus: A Challenge in Current Obstetrics: Tore HenriksenDocument12 pagesThe Macrosomic Fetus: A Challenge in Current Obstetrics: Tore HenriksenLNFNo ratings yet
- Hadlock Ultrassonography in Obstetrics and Gynecology Cap 9 1994Document16 pagesHadlock Ultrassonography in Obstetrics and Gynecology Cap 9 1994Antonio Alfim Malanchini RibeiroNo ratings yet
- Fetal Macrosomia UptodateDocument22 pagesFetal Macrosomia UptodateWinny Roman AybarNo ratings yet
- Chapter One PHDDocument55 pagesChapter One PHDL3mi DNo ratings yet
- D'Souza-2019-Maternal Body Mass Index and PregDocument17 pagesD'Souza-2019-Maternal Body Mass Index and PregMARIATUL QIFTIYAHNo ratings yet
- Fetal PII002822Document11 pagesFetal PII002822Ophay Rusty'sNo ratings yet
- Effect of Birth Weight On Adverse Obstetric.20 PDFDocument6 pagesEffect of Birth Weight On Adverse Obstetric.20 PDFTriponiaNo ratings yet
- Del 153Document6 pagesDel 153Fan AccountNo ratings yet
- Low-Risk Planned Caesarean Versus Planned Vaginal Delivery at Term: Early and Late Infantile OutcomesDocument11 pagesLow-Risk Planned Caesarean Versus Planned Vaginal Delivery at Term: Early and Late Infantile OutcomesEduarda QuartinNo ratings yet
- Outcome of Teenage PregnancyDocument5 pagesOutcome of Teenage PregnancyKN DumpNo ratings yet
- Evidence FGDocument14 pagesEvidence FGpeter_mrNo ratings yet
- Kaplan1998 PDFDocument6 pagesKaplan1998 PDFAmsir LimbongNo ratings yet
- 18014-Article Text-58443-1-10-20170813Document5 pages18014-Article Text-58443-1-10-20170813Lyka San MiguelNo ratings yet
- Maternal Underweight and The Risk of Spontaneous Abortion: Original ArticleDocument5 pagesMaternal Underweight and The Risk of Spontaneous Abortion: Original ArticleKristine Joy DivinoNo ratings yet
- 08 AimukhametovaDocument10 pages08 AimukhametovahendraNo ratings yet
- Labor and Delivery Experiences of Mothers With Suspected Large BabiesDocument5 pagesLabor and Delivery Experiences of Mothers With Suspected Large BabiesAlleyan Hannah DenumNo ratings yet
- Cephalopelvic Disproportion JournalDocument6 pagesCephalopelvic Disproportion JournalAdipta KurniawanNo ratings yet
- Slide 1Document14 pagesSlide 1Rahmat Fauzi SiregarNo ratings yet
- Risk Factors and Outcomes of Umbilical Cord Prolapse: Evaluation of 94 CasesDocument3 pagesRisk Factors and Outcomes of Umbilical Cord Prolapse: Evaluation of 94 CasesElva Diany SyamsudinNo ratings yet
- Maternal and Perinatal Outcome in Varyin PDFDocument8 pagesMaternal and Perinatal Outcome in Varyin PDFOky HermawanNo ratings yet
- An Investigation of Fetal Growth in Relation To Pregnancy CharacteristicsDocument175 pagesAn Investigation of Fetal Growth in Relation To Pregnancy CharacteristicsDr_SoranusNo ratings yet
- Shoulder Dystocia and Birth Injury: Prevention and TreatmentFrom EverandShoulder Dystocia and Birth Injury: Prevention and TreatmentNo ratings yet
- Global Landscape of Nutrition Challenges in Infants and ChildrenFrom EverandGlobal Landscape of Nutrition Challenges in Infants and ChildrenNo ratings yet
- 150 The Use of p40 Helps To Differentiate Squamous Cell Carcinoma From AdenocarcinomaDocument1 page150 The Use of p40 Helps To Differentiate Squamous Cell Carcinoma From AdenocarcinomadoctorkwekkwekNo ratings yet
- FlyerDocument1 pageFlyerdoctorkwekkwekNo ratings yet
- Capitol Citiwide, Inc.: Emerging Concepts Ob - Gyn Practical ClinicianDocument2 pagesCapitol Citiwide, Inc.: Emerging Concepts Ob - Gyn Practical CliniciandoctorkwekkwekNo ratings yet
- PDS 2014 Annual Report PDFDocument18 pagesPDS 2014 Annual Report PDFdoctorkwekkwekNo ratings yet
- PressedDocument3 pagesPresseddoctorkwekkwekNo ratings yet
- FootSizingChart PDFDocument1 pageFootSizingChart PDFdoctorkwekkwekNo ratings yet
- Efficacy and Safety of Indomethacin Therapy For PolyhydramniosDocument6 pagesEfficacy and Safety of Indomethacin Therapy For PolyhydramniosdoctorkwekkwekNo ratings yet
- Children (12 Months To 12 Years of Age)Document13 pagesChildren (12 Months To 12 Years of Age)doctorkwekkwekNo ratings yet
- Information: General Parenting TipsDocument2 pagesInformation: General Parenting TipsdoctorkwekkwekNo ratings yet
- Memo 2020-17 SUBMISSION OF DEPARTMENTAL INTERIM GUIDELINES FOR COVID-19Document1 pageMemo 2020-17 SUBMISSION OF DEPARTMENTAL INTERIM GUIDELINES FOR COVID-19doctorkwekkwekNo ratings yet
- Memo 2020-28 Interim For Ob-Gyn UltrasoundDocument4 pagesMemo 2020-28 Interim For Ob-Gyn UltrasounddoctorkwekkwekNo ratings yet
- Memo 16-INFECTION PREVENTION AND CONTROL PRACTICES FOR IMMEDIATE COMPLIANCEDocument1 pageMemo 16-INFECTION PREVENTION AND CONTROL PRACTICES FOR IMMEDIATE COMPLIANCEdoctorkwekkwekNo ratings yet
- Kalusugan ReflectionDocument3 pagesKalusugan ReflectionRizza Mae CallejaNo ratings yet
- Cord ProlapseDocument16 pagesCord ProlapseMike Evangelista100% (1)
- A Case-Control Study of Hypoxic-Ischemic Encephalopathy in Newborn Infants at 36 Weeks GestationDocument19 pagesA Case-Control Study of Hypoxic-Ischemic Encephalopathy in Newborn Infants at 36 Weeks Gestationnistor97No ratings yet
- Caculba P2wk1-Gosodpa-Rle Day 2Document4 pagesCaculba P2wk1-Gosodpa-Rle Day 2Joyce Mae Vega SarmientoNo ratings yet
- Advanced Training Skills Modules: Why, What & How?Document28 pagesAdvanced Training Skills Modules: Why, What & How?WAGS CommitteeNo ratings yet
- Diagnosis of PregnancyDocument23 pagesDiagnosis of PregnancyNeelesh BhandariNo ratings yet
- Vaginalbleedinginlate Pregnancy: Janet S. Young,, Lindsey M. WhiteDocument14 pagesVaginalbleedinginlate Pregnancy: Janet S. Young,, Lindsey M. WhiteEka NataNo ratings yet
- CHN FinaleDocument163 pagesCHN FinaleJessa Kris RialubinNo ratings yet
- Active Management of The Third Stage of LabourDocument25 pagesActive Management of The Third Stage of LabourRedroses flowers0% (1)
- Abnormal Labor - ClinicalKeyDocument32 pagesAbnormal Labor - ClinicalKeyJunior KenNo ratings yet
- Aspirin Plus Heparin or Aspirini Alone in WomanDocument20 pagesAspirin Plus Heparin or Aspirini Alone in WomanYafet Yanri SirupangNo ratings yet
- Presentation PBLM WTH ObjDocument12 pagesPresentation PBLM WTH ObjKavi rajputNo ratings yet
- Macro Teaching - PartogramDocument15 pagesMacro Teaching - PartogramSheena Sharma100% (1)
- FORM F NewDocument2 pagesFORM F NewNilesh Ghadge50% (2)
- High Risk Pregnancy: Alliah Claire Carnice BaguioDocument3 pagesHigh Risk Pregnancy: Alliah Claire Carnice BaguiokirbsNo ratings yet
- PARTOGRAMDocument17 pagesPARTOGRAMKrutthivaasa PriyaNo ratings yet
- 2143 9373 1 PBDocument6 pages2143 9373 1 PBRahmat AiduladhaNo ratings yet
- RH Incompatibility: Go ToDocument4 pagesRH Incompatibility: Go ToFadhila AnasNo ratings yet
- NorplantDocument3 pagesNorplantHeidrunKeNo ratings yet
- Unit 4 Maternal ConceptsDocument8 pagesUnit 4 Maternal ConceptsEunice TrinidadNo ratings yet
- Rajiv Gandhi University of Health Sciences, Karnataka, Bangalore Proforma For Registration of Subjects For DissertationDocument9 pagesRajiv Gandhi University of Health Sciences, Karnataka, Bangalore Proforma For Registration of Subjects For DissertationTiara Febriani NurantiNo ratings yet
- Macaraig, Jhena S.reportDocument14 pagesMacaraig, Jhena S.reportHYUNGNo ratings yet
- Lesson Plan SK IDocument13 pagesLesson Plan SK IsasikalaNo ratings yet
- Ansali, Merlyn T. BSN II-D: Theories of Labor OnsetDocument2 pagesAnsali, Merlyn T. BSN II-D: Theories of Labor OnsetMerlyn AnsaliNo ratings yet
- Hubungan Antara Panjang, Insersi, Dan Indeks Pilinan Tali Pusat Terhadap Berat Badan Lahir Pada Persalinan Preterm Di RSUP Sanglah, Denpasar, BaliDocument5 pagesHubungan Antara Panjang, Insersi, Dan Indeks Pilinan Tali Pusat Terhadap Berat Badan Lahir Pada Persalinan Preterm Di RSUP Sanglah, Denpasar, BaliGufront MustofaNo ratings yet
- Teenage PregnancyDocument18 pagesTeenage PregnancyAriel Jr Riñon MaganaNo ratings yet