Download as pdf or txt
You might also like
- 2nd Term Biology Note For Ss2Document33 pages2nd Term Biology Note For Ss2Ukwuma Michael Chijioke100% (21)
- Build Your Own Recumbent TrikeDocument242 pagesBuild Your Own Recumbent TrikeArte Colombiano100% (4)
- JMedLife 09 297 4Document5 pagesJMedLife 09 297 4verotugasNo ratings yet
- Tog 12690Document9 pagesTog 12690saeed hasan saeedNo ratings yet
- 11 Abnormal PlacentationDocument29 pages11 Abnormal PlacentationMaria Gabriela CristanchoNo ratings yet
- Good Clinical Practice Advice: Management of Twin PregnancyDocument8 pagesGood Clinical Practice Advice: Management of Twin PregnancyHambrian WijayaNo ratings yet
- 2004, Vol.31, Issues 1, Ultrasound in ObstetricsDocument213 pages2004, Vol.31, Issues 1, Ultrasound in ObstetricsFebrinata MahadikaNo ratings yet
- Twin PregnancyDocument20 pagesTwin PregnancyReynaldo Ali MarazaNo ratings yet
- Management of Monochorionic Twin Pregnancy: Green-Top Guideline No. 51Document13 pagesManagement of Monochorionic Twin Pregnancy: Green-Top Guideline No. 51indra_strongNo ratings yet
- The Role of Ultrasound in ObstetricsDocument9 pagesThe Role of Ultrasound in ObstetricsHanun FaizaNo ratings yet
- Spontaneous Preterm Birth Prevention in Multiple PregnancyDocument7 pagesSpontaneous Preterm Birth Prevention in Multiple PregnancyElias Melo JrNo ratings yet
- UOG - 2019 - Curado - Early and Late Onset Selective Fetal Growth Restriction in MonochorionicDocument6 pagesUOG - 2019 - Curado - Early and Late Onset Selective Fetal Growth Restriction in MonochorionicnehamohindrooNo ratings yet
- Embarazo EctopicoDocument10 pagesEmbarazo EctopicocfsaludNo ratings yet
- Jurnal Ultrasound 1Document6 pagesJurnal Ultrasound 1weniNo ratings yet
- KPD 2Document9 pagesKPD 2Muh AqwilNo ratings yet
- Management of Multiple Gestations: Mary E. D'Alton - Noelle BreslinDocument7 pagesManagement of Multiple Gestations: Mary E. D'Alton - Noelle BreslinAnonymous nhaFUpOLNo ratings yet
- Children 10 01114Document24 pagesChildren 10 01114Sulaeman Andrianto SusiloNo ratings yet
- Multiple Pregnancy: ReviewDocument7 pagesMultiple Pregnancy: ReviewMudassar SattarNo ratings yet
- GTN 3Document12 pagesGTN 3giant nitaNo ratings yet
- Jsafog 13 137Document5 pagesJsafog 13 137Elizabeth Duprat GaxiolaNo ratings yet
- Assessment of Factors Increasing The Risk of Prelabour Rupture of Membranes and Its Effect On Fetomaternal OutcomeDocument9 pagesAssessment of Factors Increasing The Risk of Prelabour Rupture of Membranes and Its Effect On Fetomaternal OutcomeIJAR JOURNALNo ratings yet
- Advances in Prenatal and Perinatal Diagnosis and Management of GastroschisisDocument36 pagesAdvances in Prenatal and Perinatal Diagnosis and Management of GastroschisisLondonNo ratings yet
- PPROMDocument16 pagesPPROMdavid wyantoNo ratings yet
- Hydatidiform Mole Vs PMDDocument6 pagesHydatidiform Mole Vs PMDNADIANo ratings yet
- Prenatal Diagnosis of Congenital Epulis: Implications For DeliveryDocument3 pagesPrenatal Diagnosis of Congenital Epulis: Implications For DeliveryRiznasyarielia Nikmatun NafisahNo ratings yet
- 16multiple GestationsDocument76 pages16multiple Gestationskinfe hailemariamNo ratings yet
- 6 - Preterm Pregnancy With Sacrococcygeal TeratomaDocument5 pages6 - Preterm Pregnancy With Sacrococcygeal TeratomarobertuserikkantonaNo ratings yet
- Twin Pregnancy: Prenatal Issues - UpToDateDocument70 pagesTwin Pregnancy: Prenatal Issues - UpToDateadityoNo ratings yet
- Systematic Review Placenta Calcification and Fetal OutcomeDocument22 pagesSystematic Review Placenta Calcification and Fetal OutcomeRizka AdiNo ratings yet
- European Association of Perinatal Medicine (EAPM)Document5 pagesEuropean Association of Perinatal Medicine (EAPM)zeni okta wiyantiNo ratings yet
- 3151 12154 1 PB PDFDocument5 pages3151 12154 1 PB PDFmohamad safiiNo ratings yet
- ECPM2016 ABSTRACTBOOKTheJournalofMaternal-FetalNeonatalMedicine PDFDocument314 pagesECPM2016 ABSTRACTBOOKTheJournalofMaternal-FetalNeonatalMedicine PDFDiana-Elena ComandasuNo ratings yet
- Ijss Jan Oa25 - 2017Document4 pagesIjss Jan Oa25 - 2017Esther Ellise AbundoNo ratings yet
- The Umbilic Cord Attachment Anomality and Discordant Growth of Fetus in Twin PregnancyDocument6 pagesThe Umbilic Cord Attachment Anomality and Discordant Growth of Fetus in Twin PregnancyCentral Asian StudiesNo ratings yet
- Progesterone To Prevent Spontaneous Preterm BirthDocument28 pagesProgesterone To Prevent Spontaneous Preterm BirthMiriam Rebeca Wills ThomasNo ratings yet
- 1-s2.0-S1521693422001316-mainDocument11 pages1-s2.0-S1521693422001316-mainPutri ImnidaNo ratings yet
- Guidelines For First Trimester Ultrasound Exam Part2 2004Document5 pagesGuidelines For First Trimester Ultrasound Exam Part2 2004cara0319No ratings yet
- 1fg BasgDocument5 pages1fg BasgPrasetio Kristianto BudionoNo ratings yet
- Print 1 FixDocument10 pagesPrint 1 Fixafriskha bulawanNo ratings yet
- C-Obs 42 Management of Monochorionic Twins New Mar 11Document4 pagesC-Obs 42 Management of Monochorionic Twins New Mar 11indra_strongNo ratings yet
- Diagnostic Challenges in Congenital Cytomegalovirus Infection in Pregnancy A Case ReportDocument6 pagesDiagnostic Challenges in Congenital Cytomegalovirus Infection in Pregnancy A Case ReportBen HonorseekerNo ratings yet
- TatsutaDocument5 pagesTatsutatiaranindyNo ratings yet
- 单绒毛膜双胞胎怀孕的胎儿死亡预测,并伴有III型选择性胎儿生长受限制Ultrasound Obstet GynecolDocument8 pages单绒毛膜双胞胎怀孕的胎儿死亡预测,并伴有III型选择性胎儿生长受限制Ultrasound Obstet GynecolchenziendrNo ratings yet
- Rustico 2016Document23 pagesRustico 2016Andrea Ponce AmesNo ratings yet
- Scar PregnancyDocument11 pagesScar Pregnancyasshagab04No ratings yet
- A 5-Year Review of Pattern of Placenta Previa in Ilorin, NigeriaDocument6 pagesA 5-Year Review of Pattern of Placenta Previa in Ilorin, Nigeriaamalia chairunnisaNo ratings yet
- Risk of Cerebral Palsy in Relation To Pregnancy Disorders and Preterm Birth: A National Cohort StudyDocument7 pagesRisk of Cerebral Palsy in Relation To Pregnancy Disorders and Preterm Birth: A National Cohort StudyFarin MauliaNo ratings yet
- Obgyn Ob PRPM Pt1 13Document6 pagesObgyn Ob PRPM Pt1 13SalmonteNo ratings yet
- Guideline No. 430 - Diagnosis and Management of Preterm Prelabour Rupture of MembranesDocument17 pagesGuideline No. 430 - Diagnosis and Management of Preterm Prelabour Rupture of MembranesluismcanalNo ratings yet
- Screening For Congenital AnomaliesDocument7 pagesScreening For Congenital AnomaliesFamilia CieletNo ratings yet
- CT1Document18 pagesCT1Merlin MaelissaNo ratings yet
- Prolonged Pregnancy:When Should We Intervene?Document11 pagesProlonged Pregnancy:When Should We Intervene?Raul DoctoNo ratings yet
- Frequency of Morbidly Adherent Placenta in Previous Scar: Fakhar Un Nissa, Saira Dars, Shazia Awan, Firdous MumtazDocument5 pagesFrequency of Morbidly Adherent Placenta in Previous Scar: Fakhar Un Nissa, Saira Dars, Shazia Awan, Firdous MumtazprobouNo ratings yet
- Fibroid TumorsDocument5 pagesFibroid TumorscacingpandoraNo ratings yet
- Role of Ultrasound in The Evaluation of First-Trimester PregnancyDocument13 pagesRole of Ultrasound in The Evaluation of First-Trimester PregnancyLorena RiveraNo ratings yet
- Diagnosis and Management of Ectopic Pregnancy: Europe PMC Funders GroupDocument20 pagesDiagnosis and Management of Ectopic Pregnancy: Europe PMC Funders GrouptapayanaNo ratings yet
- Normal and Abnormal Early PregnancyDocument30 pagesNormal and Abnormal Early PregnancyKhrisna AdjiNo ratings yet
- Clinical Study of Rupture Uterus - Assessment of Maternal and Fetal OutcomeDocument7 pagesClinical Study of Rupture Uterus - Assessment of Maternal and Fetal OutcomeIOSRjournalNo ratings yet
- Articulo 8Document15 pagesArticulo 8Monica ReyesNo ratings yet
- Pathology of Female Cancers: Precursor and Early-Stage Breast, Ovarian and Uterine CarcinomasFrom EverandPathology of Female Cancers: Precursor and Early-Stage Breast, Ovarian and Uterine CarcinomasTakuya MoriyaNo ratings yet
- Fast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeFrom EverandFast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeNo ratings yet
- Diagnosis of Endometrial Biopsies and Curettings: A Practical ApproachFrom EverandDiagnosis of Endometrial Biopsies and Curettings: A Practical ApproachNo ratings yet
- DHS Coast Guard LetterDocument13 pagesDHS Coast Guard LetterThe Hill NewspaperNo ratings yet
- Taylor Lift Trucks Spec Ce8a3eDocument8 pagesTaylor Lift Trucks Spec Ce8a3eIvan ManuelNo ratings yet
- Ford 970Document4 pagesFord 970amanNo ratings yet
- Gear Windage: A Review: Carol N. EastwickDocument6 pagesGear Windage: A Review: Carol N. EastwickR Prabhu SekarNo ratings yet
- Risk Management in Islamic BankingDocument17 pagesRisk Management in Islamic BankingEdi SusiloNo ratings yet
- 3 Phase Full Wave Bridge ConverterDocument4 pages3 Phase Full Wave Bridge Convertersubhasishpodder100% (1)
- Classification of HotelsDocument14 pagesClassification of HotelsJeevesh ViswambharanNo ratings yet
- Chart Patterns: Symmetrical Triangles The Ascending TriangleDocument8 pagesChart Patterns: Symmetrical Triangles The Ascending TriangleGene Stanley100% (1)
- Apache Kafka Quick Start GuideDocument180 pagesApache Kafka Quick Start GuidesleepercodeNo ratings yet
- Poliomyelitis: By: Reema I. DabbasDocument35 pagesPoliomyelitis: By: Reema I. DabbasReema DabbasNo ratings yet
- Comprobante SantanderDocument26 pagesComprobante SantanderCristinaNo ratings yet
- Replication and Disaster Recovery Administration Guide: Hitachi Unified NAS Module Hitachi NAS Platform Release 12.7Document97 pagesReplication and Disaster Recovery Administration Guide: Hitachi Unified NAS Module Hitachi NAS Platform Release 12.7PrasadValluraNo ratings yet
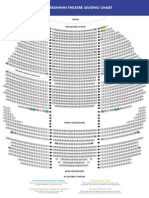
- The Gershwin Theatre Seating Chart: StageDocument1 pageThe Gershwin Theatre Seating Chart: StageCharles DavidsonNo ratings yet
- Basic TaxationDocument45 pagesBasic TaxationTessa De Claro89% (9)
- A Summary of Role and Reference GrammarDocument30 pagesA Summary of Role and Reference GrammarabarchanNo ratings yet
- B.Sc. SEM IDocument4 pagesB.Sc. SEM IsameerNo ratings yet
- Home Learning IB GR 12 June 4, 7 - 11Document6 pagesHome Learning IB GR 12 June 4, 7 - 11Arnel Ordas AvilaNo ratings yet
- ASON SLA Classification of ServicesDocument6 pagesASON SLA Classification of ServicesWondale KebedeNo ratings yet
- Abhishek Shukla Project Reporton (Power Purchase)Document57 pagesAbhishek Shukla Project Reporton (Power Purchase)beast singhNo ratings yet
- Consultants/Contractors Confirmation Check List: Consultant/Contractor UndertakingDocument1 pageConsultants/Contractors Confirmation Check List: Consultant/Contractor Undertakingom_23123062No ratings yet
- JAMB English Language Past Questions and Answers 2010 - 2018Document84 pagesJAMB English Language Past Questions and Answers 2010 - 2018Joel Adams100% (6)
- Sony PCM-7040 1st EdDocument81 pagesSony PCM-7040 1st EdnicureddogsfloNo ratings yet
- Operation Manual Hydraulic Drifter ED-100: ISO 9001:ISO 14001 CertifiedDocument55 pagesOperation Manual Hydraulic Drifter ED-100: ISO 9001:ISO 14001 CertifiedDaniel F Barros100% (2)
- Homestay Application FormDocument4 pagesHomestay Application FormlazikotoshpulatovaNo ratings yet
- Semprof SweetinaDocument20 pagesSemprof SweetinaSweetina MerkusiNo ratings yet
- Gagne VS BrunerDocument5 pagesGagne VS Bruner86mmc100% (1)
- Application of IntegralsDocument14 pagesApplication of IntegralsSanjayNo ratings yet
- DownloadLecture 10 - Entropy, Clausius InequalityDocument4 pagesDownloadLecture 10 - Entropy, Clausius Inequalityeuglena6No ratings yet