
1 s2.0 S0021755719303821 Main PDF
1 s2.0 S0021755719303821 Main PDF
You might also like
- PH Red Cross First Aid and BLSDocument71 pagesPH Red Cross First Aid and BLSctuagent75% (20)
- Pediatric Emergency NursingDocument105 pagesPediatric Emergency NursingjhommmmmNo ratings yet
- Emergency Case Review: Advanced Cardiac Life Support (ACLS) 2015Document51 pagesEmergency Case Review: Advanced Cardiac Life Support (ACLS) 2015Lely Yuniarti AhqafNo ratings yet
- CPR SeminarDocument76 pagesCPR SeminarAmy Lalringhluani Chhakchhuak100% (3)
- Module 2 BTC Final...Document71 pagesModule 2 BTC Final...Florinda See80% (5)
- BLSDocument39 pagesBLSShua QuezNo ratings yet
- Epidemiology of Pediatric Cardiopulmonary Resuscitation: Review ArticleDocument13 pagesEpidemiology of Pediatric Cardiopulmonary Resuscitation: Review ArticleMateus BragaNo ratings yet
- AHA 2020 Resusitasi PediatrikDocument74 pagesAHA 2020 Resusitasi PediatrikmeritabasrilNo ratings yet
- Septic Shock BrazilDocument12 pagesSeptic Shock BrazilutamiprakosoNo ratings yet
- Part 5: Neonatal ResuscitationDocument30 pagesPart 5: Neonatal ResuscitationFandoko ChaniagoNo ratings yet
- Part 5: Neonatal ResuscitationDocument30 pagesPart 5: Neonatal ResuscitationMarcela ZerilloNo ratings yet
- 01 Update in Pediatric ResuscitationDocument26 pages01 Update in Pediatric ResuscitationdanielentuxtlaNo ratings yet
- Part 5: Neonatal ResuscitationDocument30 pagesPart 5: Neonatal ResuscitationAngela Giselle Garcia RuizNo ratings yet
- Resusitasi Neonatus 2020 AAPDocument30 pagesResusitasi Neonatus 2020 AAPWafiq AzizahNo ratings yet
- 1 s2.0 S003139551730069XDocument12 pages1 s2.0 S003139551730069XclaudiaNo ratings yet
- CDH and Pulmonary HypertensionDocument6 pagesCDH and Pulmonary HypertensionStollery SandboxNo ratings yet
- Journal Reading Anestesi - Alfatun JamiahDocument26 pagesJournal Reading Anestesi - Alfatun JamiahAlfatun JamiahNo ratings yet
- Part 5: Neonatal ResuscitationDocument30 pagesPart 5: Neonatal Resuscitationrubie ann tillorNo ratings yet
- Neonatal Resuscitation: Thomas E Wiswell MDDocument8 pagesNeonatal Resuscitation: Thomas E Wiswell MDm6000000No ratings yet
- Septic Shock Carcillo PDFDocument14 pagesSeptic Shock Carcillo PDFjesus_berber_2No ratings yet
- Articulo ViernesDocument6 pagesArticulo Viernesvelf5No ratings yet
- Survival of Pediatric Patients After CPRDocument11 pagesSurvival of Pediatric Patients After CPRMaria Regina CamargoNo ratings yet
- PALS 2020 guidelines-AHA1Document69 pagesPALS 2020 guidelines-AHA1NICU PICUNo ratings yet
- Seminars in Pediatric Surgery: Progress in Anesthesia and Management of The Newborn Surgical PatientDocument5 pagesSeminars in Pediatric Surgery: Progress in Anesthesia and Management of The Newborn Surgical PatientAsif KhanNo ratings yet
- Siben HTPPRNDocument20 pagesSiben HTPPRNLaura B. Gómez CortésNo ratings yet
- Hipertensión Pumonar Consenso SIBENDocument20 pagesHipertensión Pumonar Consenso SIBENJuan Carlos Mata PerezNo ratings yet
- Hipertensión Pulmonar Siben 2017Document20 pagesHipertensión Pulmonar Siben 2017Carolina Cabrera CernaNo ratings yet
- Bronchopulmonary Dysplasia - StatPearls - NCBI BookshelfDocument7 pagesBronchopulmonary Dysplasia - StatPearls - NCBI BookshelfLucas AnicichNo ratings yet
- Consenso Siben HTPPDocument14 pagesConsenso Siben HTPPCristinaNo ratings yet
- Kapur 2011Document8 pagesKapur 2011Ivan VeriswanNo ratings yet
- Ogs 63 293Document12 pagesOgs 63 293DavidNo ratings yet
- Artigo Ana e Frederico 2021Document10 pagesArtigo Ana e Frederico 2021CarolinaNo ratings yet
- Oxido NitricoDocument5 pagesOxido NitricoAmparito TitoNo ratings yet
- Respiratory Distress in ChildrenDocument16 pagesRespiratory Distress in ChildrenNanda WibowoNo ratings yet
- Dysphagia and Tube Feeding After Stroke Are Associated With Poorer Functional and Mortality Outcomes (2019)Document7 pagesDysphagia and Tube Feeding After Stroke Are Associated With Poorer Functional and Mortality Outcomes (2019)Jihan FaadhilahNo ratings yet
- Badertscher Et Al 2019 Prevalence of Pulmonary Embolism in Patients With SyncopeDocument11 pagesBadertscher Et Al 2019 Prevalence of Pulmonary Embolism in Patients With SyncopeNJEBARIKANUYE EugèneNo ratings yet
- 12 FullDocument4 pages12 FullyesumovsNo ratings yet
- PCP Pediatria Revision 2023Document35 pagesPCP Pediatria Revision 2023Jorge CamarilloNo ratings yet
- Thesis On Birth AsphyxiaDocument4 pagesThesis On Birth Asphyxiaimmkhuwhd100% (3)
- HT PedDocument18 pagesHT PedLina María CañónNo ratings yet
- Retrospective Analysis of Inpatient Polysomnogram Characteristics in Infants With Broncopulmonary DisplasiaDocument30 pagesRetrospective Analysis of Inpatient Polysomnogram Characteristics in Infants With Broncopulmonary DisplasiaJHONATAN MATA ARANDANo ratings yet
- Hypertension in Infancy: Diagnosis, Management and Outcome: ReviewDocument16 pagesHypertension in Infancy: Diagnosis, Management and Outcome: ReviewJulio César Valdivieso AguirreNo ratings yet
- 06-Seminars in Fetal DevelopmentDocument75 pages06-Seminars in Fetal DevelopmentGanesh Subramanian MohanNo ratings yet
- Anasarca in The NICUDocument4 pagesAnasarca in The NICUKarina Dwi SwastikaNo ratings yet
- Guidelines Extracorporeal Membrane Oxygenation For COVID-19Document11 pagesGuidelines Extracorporeal Membrane Oxygenation For COVID-19bacharelado2010No ratings yet
- Conocimiento de BLS Y ACLS en PerúDocument8 pagesConocimiento de BLS Y ACLS en PerúMarlon RojasNo ratings yet
- Anesthetic Considerations in Paediatric Patients: UpdateDocument5 pagesAnesthetic Considerations in Paediatric Patients: UpdateYenniNo ratings yet
- Neonatal Resuscitation - 2010 AHADocument17 pagesNeonatal Resuscitation - 2010 AHApioja22507No ratings yet
- Khemani2009Document7 pagesKhemani2009Dwi Putri SekariniNo ratings yet
- Special Issue ARTICLE Less Is More: Evidence-Based Management of BronchiolitisDocument11 pagesSpecial Issue ARTICLE Less Is More: Evidence-Based Management of BronchiolitisyundaNo ratings yet
- Clopidogrel in InfantsDocument8 pagesClopidogrel in InfantsCory JuárezNo ratings yet
- Trombolisis en PCR ExtrahospitalarioDocument12 pagesTrombolisis en PCR ExtrahospitalarioMariangel PerezNo ratings yet
- Pulmonary Embolism in Children: Cme R ADocument11 pagesPulmonary Embolism in Children: Cme R Azemenum temesgenNo ratings yet
- Management and Treatment Guidelines For Sepsis in Pediatric PatientsDocument9 pagesManagement and Treatment Guidelines For Sepsis in Pediatric PatientsIhsan PutraNo ratings yet
- Shock Septico IIDocument10 pagesShock Septico IISergio Bustos VorphalNo ratings yet
- Klebsiella PDFDocument4 pagesKlebsiella PDFOscarEduardoNo ratings yet
- Outcomes of Neonates With Perinatal Asphyxia at A Tertiary Academic Hospital in Johannesburg, South AfricaDocument6 pagesOutcomes of Neonates With Perinatal Asphyxia at A Tertiary Academic Hospital in Johannesburg, South Africaeen265No ratings yet
- Bronchiolitis and Pulse Oximetry Choosing Wisely With A Technological Pandora's Box JAMA Pediatrics 2016Document2 pagesBronchiolitis and Pulse Oximetry Choosing Wisely With A Technological Pandora's Box JAMA Pediatrics 2016nathalia_pastasNo ratings yet
- Respiratory Distress in Term Babies, Can We Predict The Outcome?Document5 pagesRespiratory Distress in Term Babies, Can We Predict The Outcome?Dr. Nimesha GamhewageNo ratings yet
- Anaesthesia and Perioperative Care: Mark Newton Stella A. Eguma Olamide O. DairoDocument6 pagesAnaesthesia and Perioperative Care: Mark Newton Stella A. Eguma Olamide O. DairoNana Virtuoso EsselNo ratings yet
- Awareness of Stroke Among Patients With Chronic Kidney Disease On Hemodialysis: A Cross-Sectional StudyDocument6 pagesAwareness of Stroke Among Patients With Chronic Kidney Disease On Hemodialysis: A Cross-Sectional StudyJeffry HaryantoNo ratings yet
- 1466 FullDocument15 pages1466 FullMelvy RozaNo ratings yet
- Referensi 2Document11 pagesReferensi 2Nophy NapitupuluNo ratings yet
- Agulnik 2016Document8 pagesAgulnik 2016Karma SetiyawanNo ratings yet
- Congenital Diaphragmatic Hernia:: Updates and OutcomesDocument16 pagesCongenital Diaphragmatic Hernia:: Updates and OutcomesIRIS SAYASNo ratings yet
- References: ReplyDocument1 pageReferences: Replygevowo3277No ratings yet
- KKLDocument2 pagesKKLgevowo3277No ratings yet
- Reply: Letters To The EditorDocument2 pagesReply: Letters To The Editorgevowo3277No ratings yet
- 415 2020 Article 9898Document2 pages415 2020 Article 9898gevowo3277No ratings yet
- Clinmed 19 3 261bDocument2 pagesClinmed 19 3 261bgevowo3277No ratings yet
- Update On The Neurology of COVID 19: LettertotheeditorDocument3 pagesUpdate On The Neurology of COVID 19: Lettertotheeditorgevowo3277No ratings yet
- Case Report: An Unconscious Man With Profound Drug-Induced HypoglycaemiaDocument6 pagesCase Report: An Unconscious Man With Profound Drug-Induced Hypoglycaemiagevowo3277No ratings yet
- Research Article: Comparing Nursing Student Competence in CPR Before and After A Pedagogical InterventionDocument6 pagesResearch Article: Comparing Nursing Student Competence in CPR Before and After A Pedagogical Interventiongevowo3277No ratings yet
- 2020 Article 709Document8 pages2020 Article 709gevowo3277No ratings yet
- Barriers To Bystander CPR in Deprived Communities: Findings From A Qualitative StudyDocument11 pagesBarriers To Bystander CPR in Deprived Communities: Findings From A Qualitative Studygevowo3277No ratings yet
- Turkjmedsci 50 585Document7 pagesTurkjmedsci 50 585gevowo3277No ratings yet
- Short-Term Results of Percutaneous Treatment ofDocument6 pagesShort-Term Results of Percutaneous Treatment ofgevowo3277No ratings yet
- The Cytokine Storm and COVID-19Document24 pagesThe Cytokine Storm and COVID-19gevowo3277No ratings yet
- Resuscitation: European Resuscitation Council Guidelines 2021: Education For ResuscitationDocument20 pagesResuscitation: European Resuscitation Council Guidelines 2021: Education For Resuscitationmipan zuzuNo ratings yet
- اسنان باطنة Clinical FinalDocument40 pagesاسنان باطنة Clinical FinalShady AnwarNo ratings yet
- Cardiac Arrest in PregnancyDocument49 pagesCardiac Arrest in PregnancyTori Kehlani TanieluNo ratings yet
- Curriculum Vitae Education UsmDocument3 pagesCurriculum Vitae Education Usmapi-360825472No ratings yet
- Kuwait Pediatric GuideLinesDocument124 pagesKuwait Pediatric GuideLinesAlwaallh MohammedNo ratings yet
- BosetDocument2 pagesBosetsyamsul_mansurNo ratings yet
- SAM 350P User ManualDocument40 pagesSAM 350P User ManualkristiaNo ratings yet
- PALS Precourse Self-Assessment Score ReportDocument3 pagesPALS Precourse Self-Assessment Score ReportMaya LaPradeNo ratings yet
- Assessment of The Levels Ofcardiopulmonary Resuscitation (CPR) Among Medical Students in Northern Saudi ArabiaDocument9 pagesAssessment of The Levels Ofcardiopulmonary Resuscitation (CPR) Among Medical Students in Northern Saudi ArabiaIJAR JOURNALNo ratings yet
- Future of Work Report Ai August 2023Document30 pagesFuture of Work Report Ai August 2023rationalthinkerdd100% (1)
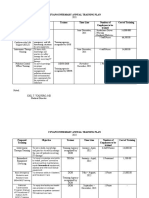
- Cuyapo Infirmary Annual Training Plan Proposed Training Objective Trainer Time Line Number of Employees To Be Trained Cost of TrainingDocument3 pagesCuyapo Infirmary Annual Training Plan Proposed Training Objective Trainer Time Line Number of Employees To Be Trained Cost of TrainingCuyapo Infirmary Lying-In HospitalNo ratings yet
- Cardiac Arrest - BLS-ACLS - Dr. KhaledDocument93 pagesCardiac Arrest - BLS-ACLS - Dr. Khaledrony ghoshNo ratings yet
- Adult CPR and Aed SkillsDocument2 pagesAdult CPR and Aed SkillsJiezl Abellano AfinidadNo ratings yet
- Basic Life Support (BLS)Document23 pagesBasic Life Support (BLS)Abdul Wahed MohammadNo ratings yet
- Dateline Fall 2020 WebDocument24 pagesDateline Fall 2020 WebindydentalsocietyNo ratings yet
- Module 1-NSTPDocument23 pagesModule 1-NSTPJj BranchNo ratings yet
- CPR GuidelinesDocument30 pagesCPR GuidelineswvhvetNo ratings yet
- ACLS Study Guide: Ecg Strip InterpretationDocument12 pagesACLS Study Guide: Ecg Strip InterpretationMariana Berger100% (2)
- Acta Medica 11 The Sinking of The MV Doña Paz A Critique On Maritime Disaster Preparedness in The Philippines Policy ImplicationsDocument12 pagesActa Medica 11 The Sinking of The MV Doña Paz A Critique On Maritime Disaster Preparedness in The Philippines Policy ImplicationsCristian AndresNo ratings yet
- Nota BLS Siri 1Document37 pagesNota BLS Siri 1PUSAT LATIHAN AADK100% (1)
- Paula Johnson Resume Updated 4-2017Document10 pagesPaula Johnson Resume Updated 4-2017pjohnson181No ratings yet
- OBSTR VA SUP EVALUACTaller Obstr Alta UpToDateDocument18 pagesOBSTR VA SUP EVALUACTaller Obstr Alta UpToDateDiegoNo ratings yet
- 2024 Obstetric Life Support Manual 1ed - CRC Press MVRDocument212 pages2024 Obstetric Life Support Manual 1ed - CRC Press MVRMelchor Alcántara BarreraNo ratings yet
- PH Red Cross First Aid and BLSDocument71 pagesPH Red Cross First Aid and BLSGenaro PalacioNo ratings yet





































































































Download as pdf or txt
You might also like
- PH Red Cross First Aid and BLSDocument71 pagesPH Red Cross First Aid and BLSctuagent75% (20)
- Pediatric Emergency NursingDocument105 pagesPediatric Emergency NursingjhommmmmNo ratings yet
- Emergency Case Review: Advanced Cardiac Life Support (ACLS) 2015Document51 pagesEmergency Case Review: Advanced Cardiac Life Support (ACLS) 2015Lely Yuniarti AhqafNo ratings yet
- CPR SeminarDocument76 pagesCPR SeminarAmy Lalringhluani Chhakchhuak100% (3)
- Module 2 BTC Final...Document71 pagesModule 2 BTC Final...Florinda See80% (5)
- BLSDocument39 pagesBLSShua QuezNo ratings yet
- Epidemiology of Pediatric Cardiopulmonary Resuscitation: Review ArticleDocument13 pagesEpidemiology of Pediatric Cardiopulmonary Resuscitation: Review ArticleMateus BragaNo ratings yet
- AHA 2020 Resusitasi PediatrikDocument74 pagesAHA 2020 Resusitasi PediatrikmeritabasrilNo ratings yet
- Septic Shock BrazilDocument12 pagesSeptic Shock BrazilutamiprakosoNo ratings yet
- Part 5: Neonatal ResuscitationDocument30 pagesPart 5: Neonatal ResuscitationFandoko ChaniagoNo ratings yet
- Part 5: Neonatal ResuscitationDocument30 pagesPart 5: Neonatal ResuscitationMarcela ZerilloNo ratings yet
- 01 Update in Pediatric ResuscitationDocument26 pages01 Update in Pediatric ResuscitationdanielentuxtlaNo ratings yet
- Part 5: Neonatal ResuscitationDocument30 pagesPart 5: Neonatal ResuscitationAngela Giselle Garcia RuizNo ratings yet
- Resusitasi Neonatus 2020 AAPDocument30 pagesResusitasi Neonatus 2020 AAPWafiq AzizahNo ratings yet
- 1 s2.0 S003139551730069XDocument12 pages1 s2.0 S003139551730069XclaudiaNo ratings yet
- CDH and Pulmonary HypertensionDocument6 pagesCDH and Pulmonary HypertensionStollery SandboxNo ratings yet
- Journal Reading Anestesi - Alfatun JamiahDocument26 pagesJournal Reading Anestesi - Alfatun JamiahAlfatun JamiahNo ratings yet
- Part 5: Neonatal ResuscitationDocument30 pagesPart 5: Neonatal Resuscitationrubie ann tillorNo ratings yet
- Neonatal Resuscitation: Thomas E Wiswell MDDocument8 pagesNeonatal Resuscitation: Thomas E Wiswell MDm6000000No ratings yet
- Septic Shock Carcillo PDFDocument14 pagesSeptic Shock Carcillo PDFjesus_berber_2No ratings yet
- Articulo ViernesDocument6 pagesArticulo Viernesvelf5No ratings yet
- Survival of Pediatric Patients After CPRDocument11 pagesSurvival of Pediatric Patients After CPRMaria Regina CamargoNo ratings yet
- PALS 2020 guidelines-AHA1Document69 pagesPALS 2020 guidelines-AHA1NICU PICUNo ratings yet
- Seminars in Pediatric Surgery: Progress in Anesthesia and Management of The Newborn Surgical PatientDocument5 pagesSeminars in Pediatric Surgery: Progress in Anesthesia and Management of The Newborn Surgical PatientAsif KhanNo ratings yet
- Siben HTPPRNDocument20 pagesSiben HTPPRNLaura B. Gómez CortésNo ratings yet
- Hipertensión Pumonar Consenso SIBENDocument20 pagesHipertensión Pumonar Consenso SIBENJuan Carlos Mata PerezNo ratings yet
- Hipertensión Pulmonar Siben 2017Document20 pagesHipertensión Pulmonar Siben 2017Carolina Cabrera CernaNo ratings yet
- Bronchopulmonary Dysplasia - StatPearls - NCBI BookshelfDocument7 pagesBronchopulmonary Dysplasia - StatPearls - NCBI BookshelfLucas AnicichNo ratings yet
- Consenso Siben HTPPDocument14 pagesConsenso Siben HTPPCristinaNo ratings yet
- Kapur 2011Document8 pagesKapur 2011Ivan VeriswanNo ratings yet
- Ogs 63 293Document12 pagesOgs 63 293DavidNo ratings yet
- Artigo Ana e Frederico 2021Document10 pagesArtigo Ana e Frederico 2021CarolinaNo ratings yet
- Oxido NitricoDocument5 pagesOxido NitricoAmparito TitoNo ratings yet
- Respiratory Distress in ChildrenDocument16 pagesRespiratory Distress in ChildrenNanda WibowoNo ratings yet
- Dysphagia and Tube Feeding After Stroke Are Associated With Poorer Functional and Mortality Outcomes (2019)Document7 pagesDysphagia and Tube Feeding After Stroke Are Associated With Poorer Functional and Mortality Outcomes (2019)Jihan FaadhilahNo ratings yet
- Badertscher Et Al 2019 Prevalence of Pulmonary Embolism in Patients With SyncopeDocument11 pagesBadertscher Et Al 2019 Prevalence of Pulmonary Embolism in Patients With SyncopeNJEBARIKANUYE EugèneNo ratings yet
- 12 FullDocument4 pages12 FullyesumovsNo ratings yet
- PCP Pediatria Revision 2023Document35 pagesPCP Pediatria Revision 2023Jorge CamarilloNo ratings yet
- Thesis On Birth AsphyxiaDocument4 pagesThesis On Birth Asphyxiaimmkhuwhd100% (3)
- HT PedDocument18 pagesHT PedLina María CañónNo ratings yet
- Retrospective Analysis of Inpatient Polysomnogram Characteristics in Infants With Broncopulmonary DisplasiaDocument30 pagesRetrospective Analysis of Inpatient Polysomnogram Characteristics in Infants With Broncopulmonary DisplasiaJHONATAN MATA ARANDANo ratings yet
- Hypertension in Infancy: Diagnosis, Management and Outcome: ReviewDocument16 pagesHypertension in Infancy: Diagnosis, Management and Outcome: ReviewJulio César Valdivieso AguirreNo ratings yet
- 06-Seminars in Fetal DevelopmentDocument75 pages06-Seminars in Fetal DevelopmentGanesh Subramanian MohanNo ratings yet
- Anasarca in The NICUDocument4 pagesAnasarca in The NICUKarina Dwi SwastikaNo ratings yet
- Guidelines Extracorporeal Membrane Oxygenation For COVID-19Document11 pagesGuidelines Extracorporeal Membrane Oxygenation For COVID-19bacharelado2010No ratings yet
- Conocimiento de BLS Y ACLS en PerúDocument8 pagesConocimiento de BLS Y ACLS en PerúMarlon RojasNo ratings yet
- Anesthetic Considerations in Paediatric Patients: UpdateDocument5 pagesAnesthetic Considerations in Paediatric Patients: UpdateYenniNo ratings yet
- Neonatal Resuscitation - 2010 AHADocument17 pagesNeonatal Resuscitation - 2010 AHApioja22507No ratings yet
- Khemani2009Document7 pagesKhemani2009Dwi Putri SekariniNo ratings yet
- Special Issue ARTICLE Less Is More: Evidence-Based Management of BronchiolitisDocument11 pagesSpecial Issue ARTICLE Less Is More: Evidence-Based Management of BronchiolitisyundaNo ratings yet
- Clopidogrel in InfantsDocument8 pagesClopidogrel in InfantsCory JuárezNo ratings yet
- Trombolisis en PCR ExtrahospitalarioDocument12 pagesTrombolisis en PCR ExtrahospitalarioMariangel PerezNo ratings yet
- Pulmonary Embolism in Children: Cme R ADocument11 pagesPulmonary Embolism in Children: Cme R Azemenum temesgenNo ratings yet
- Management and Treatment Guidelines For Sepsis in Pediatric PatientsDocument9 pagesManagement and Treatment Guidelines For Sepsis in Pediatric PatientsIhsan PutraNo ratings yet
- Shock Septico IIDocument10 pagesShock Septico IISergio Bustos VorphalNo ratings yet
- Klebsiella PDFDocument4 pagesKlebsiella PDFOscarEduardoNo ratings yet
- Outcomes of Neonates With Perinatal Asphyxia at A Tertiary Academic Hospital in Johannesburg, South AfricaDocument6 pagesOutcomes of Neonates With Perinatal Asphyxia at A Tertiary Academic Hospital in Johannesburg, South Africaeen265No ratings yet
- Bronchiolitis and Pulse Oximetry Choosing Wisely With A Technological Pandora's Box JAMA Pediatrics 2016Document2 pagesBronchiolitis and Pulse Oximetry Choosing Wisely With A Technological Pandora's Box JAMA Pediatrics 2016nathalia_pastasNo ratings yet
- Respiratory Distress in Term Babies, Can We Predict The Outcome?Document5 pagesRespiratory Distress in Term Babies, Can We Predict The Outcome?Dr. Nimesha GamhewageNo ratings yet
- Anaesthesia and Perioperative Care: Mark Newton Stella A. Eguma Olamide O. DairoDocument6 pagesAnaesthesia and Perioperative Care: Mark Newton Stella A. Eguma Olamide O. DairoNana Virtuoso EsselNo ratings yet
- Awareness of Stroke Among Patients With Chronic Kidney Disease On Hemodialysis: A Cross-Sectional StudyDocument6 pagesAwareness of Stroke Among Patients With Chronic Kidney Disease On Hemodialysis: A Cross-Sectional StudyJeffry HaryantoNo ratings yet
- 1466 FullDocument15 pages1466 FullMelvy RozaNo ratings yet
- Referensi 2Document11 pagesReferensi 2Nophy NapitupuluNo ratings yet
- Agulnik 2016Document8 pagesAgulnik 2016Karma SetiyawanNo ratings yet
- Congenital Diaphragmatic Hernia:: Updates and OutcomesDocument16 pagesCongenital Diaphragmatic Hernia:: Updates and OutcomesIRIS SAYASNo ratings yet
- References: ReplyDocument1 pageReferences: Replygevowo3277No ratings yet
- KKLDocument2 pagesKKLgevowo3277No ratings yet
- Reply: Letters To The EditorDocument2 pagesReply: Letters To The Editorgevowo3277No ratings yet
- 415 2020 Article 9898Document2 pages415 2020 Article 9898gevowo3277No ratings yet
- Clinmed 19 3 261bDocument2 pagesClinmed 19 3 261bgevowo3277No ratings yet
- Update On The Neurology of COVID 19: LettertotheeditorDocument3 pagesUpdate On The Neurology of COVID 19: Lettertotheeditorgevowo3277No ratings yet
- Case Report: An Unconscious Man With Profound Drug-Induced HypoglycaemiaDocument6 pagesCase Report: An Unconscious Man With Profound Drug-Induced Hypoglycaemiagevowo3277No ratings yet
- Research Article: Comparing Nursing Student Competence in CPR Before and After A Pedagogical InterventionDocument6 pagesResearch Article: Comparing Nursing Student Competence in CPR Before and After A Pedagogical Interventiongevowo3277No ratings yet
- 2020 Article 709Document8 pages2020 Article 709gevowo3277No ratings yet
- Barriers To Bystander CPR in Deprived Communities: Findings From A Qualitative StudyDocument11 pagesBarriers To Bystander CPR in Deprived Communities: Findings From A Qualitative Studygevowo3277No ratings yet
- Turkjmedsci 50 585Document7 pagesTurkjmedsci 50 585gevowo3277No ratings yet
- Short-Term Results of Percutaneous Treatment ofDocument6 pagesShort-Term Results of Percutaneous Treatment ofgevowo3277No ratings yet
- The Cytokine Storm and COVID-19Document24 pagesThe Cytokine Storm and COVID-19gevowo3277No ratings yet
- Resuscitation: European Resuscitation Council Guidelines 2021: Education For ResuscitationDocument20 pagesResuscitation: European Resuscitation Council Guidelines 2021: Education For Resuscitationmipan zuzuNo ratings yet
- اسنان باطنة Clinical FinalDocument40 pagesاسنان باطنة Clinical FinalShady AnwarNo ratings yet
- Cardiac Arrest in PregnancyDocument49 pagesCardiac Arrest in PregnancyTori Kehlani TanieluNo ratings yet
- Curriculum Vitae Education UsmDocument3 pagesCurriculum Vitae Education Usmapi-360825472No ratings yet
- Kuwait Pediatric GuideLinesDocument124 pagesKuwait Pediatric GuideLinesAlwaallh MohammedNo ratings yet
- BosetDocument2 pagesBosetsyamsul_mansurNo ratings yet
- SAM 350P User ManualDocument40 pagesSAM 350P User ManualkristiaNo ratings yet
- PALS Precourse Self-Assessment Score ReportDocument3 pagesPALS Precourse Self-Assessment Score ReportMaya LaPradeNo ratings yet
- Assessment of The Levels Ofcardiopulmonary Resuscitation (CPR) Among Medical Students in Northern Saudi ArabiaDocument9 pagesAssessment of The Levels Ofcardiopulmonary Resuscitation (CPR) Among Medical Students in Northern Saudi ArabiaIJAR JOURNALNo ratings yet
- Future of Work Report Ai August 2023Document30 pagesFuture of Work Report Ai August 2023rationalthinkerdd100% (1)
- Cuyapo Infirmary Annual Training Plan Proposed Training Objective Trainer Time Line Number of Employees To Be Trained Cost of TrainingDocument3 pagesCuyapo Infirmary Annual Training Plan Proposed Training Objective Trainer Time Line Number of Employees To Be Trained Cost of TrainingCuyapo Infirmary Lying-In HospitalNo ratings yet
- Cardiac Arrest - BLS-ACLS - Dr. KhaledDocument93 pagesCardiac Arrest - BLS-ACLS - Dr. Khaledrony ghoshNo ratings yet
- Adult CPR and Aed SkillsDocument2 pagesAdult CPR and Aed SkillsJiezl Abellano AfinidadNo ratings yet
- Basic Life Support (BLS)Document23 pagesBasic Life Support (BLS)Abdul Wahed MohammadNo ratings yet
- Dateline Fall 2020 WebDocument24 pagesDateline Fall 2020 WebindydentalsocietyNo ratings yet
- Module 1-NSTPDocument23 pagesModule 1-NSTPJj BranchNo ratings yet
- CPR GuidelinesDocument30 pagesCPR GuidelineswvhvetNo ratings yet
- ACLS Study Guide: Ecg Strip InterpretationDocument12 pagesACLS Study Guide: Ecg Strip InterpretationMariana Berger100% (2)
- Acta Medica 11 The Sinking of The MV Doña Paz A Critique On Maritime Disaster Preparedness in The Philippines Policy ImplicationsDocument12 pagesActa Medica 11 The Sinking of The MV Doña Paz A Critique On Maritime Disaster Preparedness in The Philippines Policy ImplicationsCristian AndresNo ratings yet
- Nota BLS Siri 1Document37 pagesNota BLS Siri 1PUSAT LATIHAN AADK100% (1)
- Paula Johnson Resume Updated 4-2017Document10 pagesPaula Johnson Resume Updated 4-2017pjohnson181No ratings yet
- OBSTR VA SUP EVALUACTaller Obstr Alta UpToDateDocument18 pagesOBSTR VA SUP EVALUACTaller Obstr Alta UpToDateDiegoNo ratings yet
- 2024 Obstetric Life Support Manual 1ed - CRC Press MVRDocument212 pages2024 Obstetric Life Support Manual 1ed - CRC Press MVRMelchor Alcántara BarreraNo ratings yet
- PH Red Cross First Aid and BLSDocument71 pagesPH Red Cross First Aid and BLSGenaro PalacioNo ratings yet