Download as pdf or txt
You might also like
- What Do You Think of The Discounting Scheme That KAR Had Used Historically? Do You Think It Was Justified Given The Circumstances?Document3 pagesWhat Do You Think of The Discounting Scheme That KAR Had Used Historically? Do You Think It Was Justified Given The Circumstances?Lohith Kumar100% (1)
- GE2777 PentaPals The Urbanization in Davao City and Its Impacts To Climate ChangeDocument7 pagesGE2777 PentaPals The Urbanization in Davao City and Its Impacts To Climate Changewendell tatoy1No ratings yet
- Markvie TagsDocument28 pagesMarkvie Tagssrinivas100% (2)
- DownloadDocument9 pagesDownloadRhuan AlexandreNo ratings yet
- A Study On Premarital Screening For Sickle Cell Trait in Hilly Areas Around SalemDocument4 pagesA Study On Premarital Screening For Sickle Cell Trait in Hilly Areas Around SalemBIOMEDSCIDIRECT PUBLICATIONSNo ratings yet
- Nasopalatine Duct Cyst Restro StudyDocument8 pagesNasopalatine Duct Cyst Restro StudyTiara Oktavia SaputriNo ratings yet
- Chronic Osteo-Articular Changes in Patients With Sickle Cell DiseaseDocument5 pagesChronic Osteo-Articular Changes in Patients With Sickle Cell DiseaseAlexandra LealNo ratings yet
- Interdisciplinary Medicine and Dental Science: Dental Complications of Sickle Cell DiseaseDocument4 pagesInterdisciplinary Medicine and Dental Science: Dental Complications of Sickle Cell DiseaseLaura Mejia VergaraNo ratings yet
- Gut Microbiome Alterations in Alzheimer'S Disease: ReportsDocument11 pagesGut Microbiome Alterations in Alzheimer'S Disease: ReportsVictoria HristovaNo ratings yet
- 2007 28 259 M. Catherine Driscoll: Pediatrics in ReviewDocument12 pages2007 28 259 M. Catherine Driscoll: Pediatrics in ReviewcharlesNo ratings yet
- Dental Caries An Update Medical Model Risk AssesmentDocument6 pagesDental Caries An Update Medical Model Risk AssesmentJuan Andres EspinozaNo ratings yet
- Acuan - Oral Manifestation Di Kidney Disease 129 DataDocument13 pagesAcuan - Oral Manifestation Di Kidney Disease 129 DataCheeny MicaNo ratings yet
- Advances in The Treatment of Sickle CellDocument15 pagesAdvances in The Treatment of Sickle CellMayuri P KNo ratings yet
- RP-Case History of A Child With Sickle Cell Anemia in IndiaDocument5 pagesRP-Case History of A Child With Sickle Cell Anemia in IndiaMarie Kelsey Acena MacaraigNo ratings yet
- Brooks 2018Document37 pagesBrooks 2018Menma Uchiha Sumātona Kodomo-tachiNo ratings yet
- Costa JOE2013Document5 pagesCosta JOE2013KristineNo ratings yet
- A Living Biobank of Breast Cancer OrganoidsDocument25 pagesA Living Biobank of Breast Cancer Organoidsfernando dominguezNo ratings yet
- Actinic Cheilitis Clinicopathologic Profile and Association With Degree of DysplasiaDocument7 pagesActinic Cheilitis Clinicopathologic Profile and Association With Degree of DysplasiaYusuf DiansyahNo ratings yet
- DR - Muddassir Final Synopsis..Document22 pagesDR - Muddassir Final Synopsis..Sikander GirgoukarNo ratings yet
- Mechanisms Involved in Hearing Disorders of Thyroid Ontogeny: A Literature ReviewDocument5 pagesMechanisms Involved in Hearing Disorders of Thyroid Ontogeny: A Literature ReviewCaio LeônidasNo ratings yet
- Nutrients 14 03959Document15 pagesNutrients 14 03959CrisNo ratings yet
- Literature Review of Sickle Cell AnaemiaDocument5 pagesLiterature Review of Sickle Cell Anaemiaafdtveepo100% (1)
- Lingen Et Al-2011-Oral DiseasesDocument16 pagesLingen Et Al-2011-Oral DiseasesSAMUEL ESCARESNo ratings yet
- Journal Pre-Proof: Oral Surg Oral Med Oral Pathol Oral RadiolDocument23 pagesJournal Pre-Proof: Oral Surg Oral Med Oral Pathol Oral Radiolabhishekjha0082No ratings yet
- Jurnal Pedo IzzahDocument5 pagesJurnal Pedo IzzahSuper LonelyNo ratings yet
- Microbiome in Sjögren's Syndrome - Here We AreDocument2 pagesMicrobiome in Sjögren's Syndrome - Here We AreMartinaNo ratings yet
- Clinical Presentations of Sjogren's Syndrome in Benghazi, PDFDocument6 pagesClinical Presentations of Sjogren's Syndrome in Benghazi, PDFKhaled AlsaeitiNo ratings yet
- s11695 022 06410 4 PDFDocument7 pagess11695 022 06410 4 PDFTan BulNo ratings yet
- Clinical Features and Antimicrobial Susceptibility of Oral B 2022 Journal ofDocument6 pagesClinical Features and Antimicrobial Susceptibility of Oral B 2022 Journal ofDavid ABCNo ratings yet
- Diagnosis of Hirschsprung Disease: Lusine Ambartsumyan, Caitlin Smith, and Raj P KapurDocument15 pagesDiagnosis of Hirschsprung Disease: Lusine Ambartsumyan, Caitlin Smith, and Raj P KapurGhina Mauizha WulandariNo ratings yet
- Detection of Deletions at 7q11.23 in Williams-BeurenDocument6 pagesDetection of Deletions at 7q11.23 in Williams-BeurenAmisadai ArévaloNo ratings yet
- Pediatrics in Review 2012 McCavit 195 206Document14 pagesPediatrics in Review 2012 McCavit 195 206cindyNo ratings yet
- A Review of Sickle Cell Disease and ReplyDocument15 pagesA Review of Sickle Cell Disease and ReplyGisella Del Río HernándezNo ratings yet
- IJCDOral Mucositis 2014Document11 pagesIJCDOral Mucositis 2014Aarya Haridasan NairNo ratings yet
- Art:10.1186/s12903 015 0052 4Document8 pagesArt:10.1186/s12903 015 0052 4Laura Mejia VergaraNo ratings yet
- Histologic Subtypes of Oral Squamous Cell Carcinoma: Prognostic RelevanceDocument7 pagesHistologic Subtypes of Oral Squamous Cell Carcinoma: Prognostic RelevanceDeyfa RehadiNo ratings yet
- Int Endodontic J - 2021 - Tib Rcio MachadoDocument24 pagesInt Endodontic J - 2021 - Tib Rcio Machadoisabel sotoNo ratings yet
- Research Article: Williams-Beuren Syndrome: A Clinical Study of 55 Brazilian Patients and The Diagnostic Use of MLPADocument7 pagesResearch Article: Williams-Beuren Syndrome: A Clinical Study of 55 Brazilian Patients and The Diagnostic Use of MLPApejavzNo ratings yet
- Melioidosis: Review ArticleDocument10 pagesMelioidosis: Review ArticlePutri YunandaNo ratings yet
- Condrodisplacia de Un TerneroDocument6 pagesCondrodisplacia de Un TerneroAbraham Perez CueterNo ratings yet
- Cancer Cytopathology - 2020 - Velleuer - Diagnostic Accuracy of Brush Biopsy Based Cytology For The Early Detection of OralDocument11 pagesCancer Cytopathology - 2020 - Velleuer - Diagnostic Accuracy of Brush Biopsy Based Cytology For The Early Detection of Oralopy dasNo ratings yet
- Is It Sjogren's Syndrome or Burning Mouth SyndromeDocument25 pagesIs It Sjogren's Syndrome or Burning Mouth SyndromeGentianaNo ratings yet
- Bilateral Mandibular Osteomyelitis Mimicking Periapical Cysts in A Patient With Sickle Cell AnemiaDocument6 pagesBilateral Mandibular Osteomyelitis Mimicking Periapical Cysts in A Patient With Sickle Cell AnemiaLaura Mejia VergaraNo ratings yet
- A Review Literature On Sickle Cell Anemia: Akanksha PatelDocument21 pagesA Review Literature On Sickle Cell Anemia: Akanksha PatelNoe Essono KolloNo ratings yet
- Patient With Sickle Cell AnemiaDocument14 pagesPatient With Sickle Cell AnemiaAbilio Torres100% (1)
- Anemia ResearchDocument31 pagesAnemia ResearchMike Faustino SolangonNo ratings yet
- EDT Genetic Analysis of XRCC1 Polymorphism in Leukemia FINALDocument41 pagesEDT Genetic Analysis of XRCC1 Polymorphism in Leukemia FINALAli Haider DhariwalNo ratings yet
- Sickle Cell Anemia A Succinct Look Into Recently Tested Disease Modifying InterventionsDocument10 pagesSickle Cell Anemia A Succinct Look Into Recently Tested Disease Modifying InterventionsAthenaeum Scientific PublishersNo ratings yet
- Ijsc 2527Document6 pagesIjsc 2527Pedro AzevedoNo ratings yet
- Association of Microbiome With Oral Squamous CellDocument21 pagesAssociation of Microbiome With Oral Squamous CellGhimpu DanielaNo ratings yet
- Tomanin Et Al-2018-Human MutationDocument15 pagesTomanin Et Al-2018-Human MutationLaura Daniela MurilloNo ratings yet
- Fped 08 00038Document22 pagesFped 08 00038Gisella Del Río HernándezNo ratings yet
- American J of Med Genetics PT A - 2021 - Ewing - Microdeletion of 9q22 3 A Patient With Minimal Deletion Size AssociatedDocument14 pagesAmerican J of Med Genetics PT A - 2021 - Ewing - Microdeletion of 9q22 3 A Patient With Minimal Deletion Size Associatedhennysusanto18No ratings yet
- Oral Leukoplakia Remains A Challenging Condition: A Villa - S SonisDocument5 pagesOral Leukoplakia Remains A Challenging Condition: A Villa - S SonisDaniela Suarez TamayoNo ratings yet
- Jurnal OM TransleteDocument7 pagesJurnal OM TransleterisjunNo ratings yet
- Restrepo Et Al-2016-International Journal of Paediatric Dentistry PDFDocument9 pagesRestrepo Et Al-2016-International Journal of Paediatric Dentistry PDFJakeCrNo ratings yet
- Deletion Syndrome in Colombian Patients With Syndromic Cleft Lipand/or PalateDocument7 pagesDeletion Syndrome in Colombian Patients With Syndromic Cleft Lipand/or Palateangee.bautista19No ratings yet
- Thesis On Sickle Cell DiseaseDocument8 pagesThesis On Sickle Cell Diseaseafbtfukel100% (1)
- 1 s2.0 S2589004221008932 MainDocument11 pages1 s2.0 S2589004221008932 MainBen DresimNo ratings yet
- Lesões Malignas - Med OralDocument8 pagesLesões Malignas - Med OralCaio GonçalvesNo ratings yet
- Prevalence of Hemoglobinosis in School Environments: Case of The City of Abengourou in Ivory CoastDocument6 pagesPrevalence of Hemoglobinosis in School Environments: Case of The City of Abengourou in Ivory CoastIJAR JOURNALNo ratings yet
- Archives of Gerontology and Geriatrics: A. Fattori, M.R. Santimaria, R.M.A. Alves, M.E. Guariento, A.L. NeriDocument7 pagesArchives of Gerontology and Geriatrics: A. Fattori, M.R. Santimaria, R.M.A. Alves, M.E. Guariento, A.L. NeriCarlos CarrilloNo ratings yet
- Bilateral Mandibular Osteomyelitis Mimicking Periapical Cysts in A Patient With Sickle Cell AnemiaDocument6 pagesBilateral Mandibular Osteomyelitis Mimicking Periapical Cysts in A Patient With Sickle Cell AnemiaLaura Mejia VergaraNo ratings yet
- Art:10.1186/s12903 015 0052 4Document8 pagesArt:10.1186/s12903 015 0052 4Laura Mejia VergaraNo ratings yet
- The Association Between Dental and Periodontal Diseases and Sickle Cell Disease. A Pilot Case-Control StudyDocument4 pagesThe Association Between Dental and Periodontal Diseases and Sickle Cell Disease. A Pilot Case-Control StudyLaura Mejia VergaraNo ratings yet
- Interdisciplinary Medicine and Dental Science: Dental Complications of Sickle Cell DiseaseDocument4 pagesInterdisciplinary Medicine and Dental Science: Dental Complications of Sickle Cell DiseaseLaura Mejia VergaraNo ratings yet
- Dental Alterations in Sickle Cell Disease: April 2016Document6 pagesDental Alterations in Sickle Cell Disease: April 2016Laura Mejia VergaraNo ratings yet
- International Rules For Seed Testing 2022Document14 pagesInternational Rules For Seed Testing 2022Lolpo Kolpo100% (2)
- The Modern Dwelling in Germany 1890-1914Document29 pagesThe Modern Dwelling in Germany 1890-1914Inside BodyNo ratings yet
- Nokia Case StudyDocument12 pagesNokia Case Studysatyam basaiyeNo ratings yet
- Basic Tools and Equipment Used in Meal PreparationDocument37 pagesBasic Tools and Equipment Used in Meal Preparationhersal fae gerardo100% (2)
- Quint-Ups 24DC 24DC 40Document6 pagesQuint-Ups 24DC 24DC 40abdullahNo ratings yet
- Oil SensorsDocument6 pagesOil SensorssxpNo ratings yet
- Kunci Gitar One Ok Rock - Be The Light Chord Dasar Kunci Gitar & Lirik Lagu ©ChordTela PDFDocument4 pagesKunci Gitar One Ok Rock - Be The Light Chord Dasar Kunci Gitar & Lirik Lagu ©ChordTela PDFGriya Adi PartaNo ratings yet
- Literature Review 2. 1 Definition 2. 1. 1 Definition of NsaidsDocument17 pagesLiterature Review 2. 1 Definition 2. 1. 1 Definition of NsaidsROHITNo ratings yet
- WSH Guidelines Commercial DivingDocument151 pagesWSH Guidelines Commercial Divingyassentaha20000No ratings yet
- Catálogo SuplementosDocument55 pagesCatálogo SuplementosMarcilio BrunoNo ratings yet
- Email Correspondance - Ato Payment PlanDocument2 pagesEmail Correspondance - Ato Payment Planapi-358201396No ratings yet
- Policies Regarding Water Conservation in India (Conserve Water, Conserve Life, Save Water, and It Will Save You)Document11 pagesPolicies Regarding Water Conservation in India (Conserve Water, Conserve Life, Save Water, and It Will Save You)International Journal of Innovative Science and Research TechnologyNo ratings yet
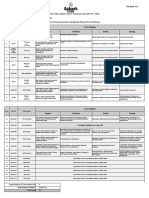
- Test Planner - Phase-01 For CF OYM - AY-2024-2025 Version 1.0Document2 pagesTest Planner - Phase-01 For CF OYM - AY-2024-2025 Version 1.0GorgonSlayer41No ratings yet
- The Interaction Function 3 EsoDocument2 pagesThe Interaction Function 3 EsoParty CularNo ratings yet
- 100 6TH Sem-Dse4t-Classification of Mushroom - Saini MandalDocument15 pages100 6TH Sem-Dse4t-Classification of Mushroom - Saini MandalJada KnightsNo ratings yet
- Failures in FPDDocument15 pagesFailures in FPDAnkita Piplani DuaNo ratings yet
- DS PNSSDocument3 pagesDS PNSSKathryne May JinonNo ratings yet
- 1725S1TKCE60132018 - Operasi Teknik Kimia III - Pertemuan 8 - TugasDocument2 pages1725S1TKCE60132018 - Operasi Teknik Kimia III - Pertemuan 8 - TugasPaulus Sampe LambiNo ratings yet
- Proposal Defense Correction Matrix Comment ReactionDocument2 pagesProposal Defense Correction Matrix Comment ReactionIZIMBA67% (6)
- Activity 3-Cognitive Diffusion Mindfulness Meditation 1Document3 pagesActivity 3-Cognitive Diffusion Mindfulness Meditation 1api-568093192No ratings yet
- Five Temperaments PDFDocument4 pagesFive Temperaments PDFgargamel09400% (1)
- Soal PAT B.ING Kelas 4Document4 pagesSoal PAT B.ING Kelas 4NurmaAnggeliaNo ratings yet
- Ethics CaseDocument3 pagesEthics Casekishi8mempinNo ratings yet
- MuetDocument2 pagesMuetYi XunNo ratings yet
- Adhesives and Consolidants For Wax and Wax-Like Materials: ArticleDocument9 pagesAdhesives and Consolidants For Wax and Wax-Like Materials: ArticleFelix LeeNo ratings yet
- Keycote Binder System: R&R Ransom & RandolphDocument2 pagesKeycote Binder System: R&R Ransom & RandolphskluxNo ratings yet
- 2015parathyroid Carcinoma Challenges in Diagnosis and TreatmentDocument9 pages2015parathyroid Carcinoma Challenges in Diagnosis and TreatmentCharley WangNo ratings yet