Download as doc, pdf, or txt
You might also like
- Moonlight PDFDocument371 pagesMoonlight PDFFerzada Sajiran100% (2)
- Brock Biology of Microorganisms 13th Edition 140814191244 Phpapp01Document10 pagesBrock Biology of Microorganisms 13th Edition 140814191244 Phpapp01Anas LeoNo ratings yet
- Immunity (Medical) : Immunity Is A Biological Term That Describes A State of Having Sufficient BiologicalDocument8 pagesImmunity (Medical) : Immunity Is A Biological Term That Describes A State of Having Sufficient BiologicalStephanie Gianina Fong100% (1)
- ImmunologyDocument38 pagesImmunologyquaisherhossainNo ratings yet
- Introduction To The Immune SystemDocument19 pagesIntroduction To The Immune Systemratnesh gautamNo ratings yet
- Immunity: Presented By: DR - Reena Rani PG1 Year Pediatric and Preventive DentistryDocument137 pagesImmunity: Presented By: DR - Reena Rani PG1 Year Pediatric and Preventive DentistryReenaChauhanNo ratings yet
- Immunology & Immunological PreparationDocument129 pagesImmunology & Immunological PreparationBijayaKumarUprety67% (3)
- Immunologic PharmaDocument20 pagesImmunologic PharmaAnnapril TasicNo ratings yet
- BiologyDocument27 pagesBiologyAnand GNo ratings yet
- Zoology6thSem PDFDocument88 pagesZoology6thSem PDFRouf MalikNo ratings yet
- IMMUNOLOGYDocument26 pagesIMMUNOLOGY6r2byw6xnxNo ratings yet
- Introduction To Immunology PDFDocument15 pagesIntroduction To Immunology PDFanon_143800659100% (1)
- Chap. 1Document25 pagesChap. 1NadineNo ratings yet
- ImmunityDocument17 pagesImmunityNAVEEN DHIMANNo ratings yet
- IMY Unit 1, Sub Unit 1.1Document11 pagesIMY Unit 1, Sub Unit 1.1fdvfsgffefNo ratings yet
- MICROBIOLOGYDocument3 pagesMICROBIOLOGYbritishsam57No ratings yet
- Chunilal Mandal Paper2Document12 pagesChunilal Mandal Paper2Surbhi RawalNo ratings yet
- ImmunologyDocument7 pagesImmunologyadelbaneen31No ratings yet
- Comment On The Following ProverbsDocument4 pagesComment On The Following ProverbsArina CucuruzaNo ratings yet
- Vaccinosis 1Document24 pagesVaccinosis 1Dr-Sayantan BasuNo ratings yet
- MLS326 Basic ImmunologyDocument28 pagesMLS326 Basic ImmunologyMayowa OgunmolaNo ratings yet
- Basic ImmunologyDocument21 pagesBasic ImmunologyZubair AlamNo ratings yet
- ImmunityDocument31 pagesImmunityattiarph23No ratings yet
- Introduction To ImmunologyDocument10 pagesIntroduction To ImmunologyArpita MishraNo ratings yet
- Theories of Disease Causation Level200Document5 pagesTheories of Disease Causation Level200Annan Agyekum JoshuaNo ratings yet
- Sistem ImunDocument24 pagesSistem ImundliaaNo ratings yet
- (PPT) DPC 1.4.2 Immunity and Disease - Dr. Cabanos PDFDocument83 pages(PPT) DPC 1.4.2 Immunity and Disease - Dr. Cabanos PDFJennifer Pisco LiracNo ratings yet
- The Defense of The Body: Chapter Outline Key PointsDocument10 pagesThe Defense of The Body: Chapter Outline Key PointsMARIA ALEJANDRA BERMUDEZ BUITRAGONo ratings yet
- Immunology AssignmentDocument14 pagesImmunology AssignmentP AdelineNo ratings yet
- IntroductionDocument41 pagesIntroductionworknehbethanyNo ratings yet
- Human Health and DiseasesDocument74 pagesHuman Health and Diseasessimra farooquiNo ratings yet
- VMC 221 Coursematerials PDFDocument61 pagesVMC 221 Coursematerials PDFavenger 2100% (1)
- Immune SystemDocument1 pageImmune SystemTamil VillardoNo ratings yet
- Class IX Science Why Do We Fall Ill NotesDocument15 pagesClass IX Science Why Do We Fall Ill NotesASHWANI KUMARNo ratings yet
- Host Defence..Document23 pagesHost Defence..Nagendrappa MalipatilNo ratings yet
- SCIENTISTSDocument5 pagesSCIENTISTSMarica Mae PreNo ratings yet
- IMMUNITY - 5th FormDocument21 pagesIMMUNITY - 5th FormKristal CampbellNo ratings yet
- Serology Section in Principles of Medical Laboratory ScienceDocument3 pagesSerology Section in Principles of Medical Laboratory ScienceElle ENo ratings yet
- Undergraduate Immunology Course (2018-2019) For Third Class: Biology Dept. College of ScienceDocument34 pagesUndergraduate Immunology Course (2018-2019) For Third Class: Biology Dept. College of ScienceAhmed Asaad Majid Al Mousawi100% (1)
- Micro Assignment Unit 3 Group BDocument12 pagesMicro Assignment Unit 3 Group Bnabeelpatras19No ratings yet
- IS LessonDocument30 pagesIS Lessonjohn dale duranoNo ratings yet
- Imse Trans PrelimDocument12 pagesImse Trans PrelimSarah EugenioNo ratings yet
- Disease and Immunity NotesDocument8 pagesDisease and Immunity NotesFaeequa nasrahNo ratings yet
- The Immune SystemDocument4 pagesThe Immune SystemSseguya Lubega YaqubNo ratings yet
- The Role of The Circulatory System in The Body's Defence MechanismDocument22 pagesThe Role of The Circulatory System in The Body's Defence MechanismSyamsamaria AzizNo ratings yet
- Prof. Dr. Payman A.Hamaseed: VaccinationDocument19 pagesProf. Dr. Payman A.Hamaseed: Vaccinationasia groupNo ratings yet
- MicroDocument6 pagesMicroMaynard ArandaNo ratings yet
- Types of ImmunityDocument13 pagesTypes of ImmunityKailash Nagar100% (3)
- History of ImmunologyDocument18 pagesHistory of ImmunologyOlgah NyamorNo ratings yet
- ImmunizationDocument10 pagesImmunizationVernon MonteiroNo ratings yet
- 1 Immunology 1Document55 pages1 Immunology 1Iqra NaeemNo ratings yet
- CH 1. Overview of The Immune SystemDocument23 pagesCH 1. Overview of The Immune SystemIbrahim MNo ratings yet
- Csa ExerciseDocument17 pagesCsa ExerciseBlack starNo ratings yet
- Acquired Immunity Immune Memory: NtroductionDocument2 pagesAcquired Immunity Immune Memory: NtroductionShahid MahmudNo ratings yet
- Immunity Is Defined As Resistance To Disease, Specifically Infectious Disease. TheDocument9 pagesImmunity Is Defined As Resistance To Disease, Specifically Infectious Disease. Thesaad samyNo ratings yet
- Human Health & DiseasesDocument55 pagesHuman Health & DiseasesSAGAR PADALKARNo ratings yet
- Mutate or Die - DiseaseDocument34 pagesMutate or Die - Diseasefreddiek2004No ratings yet
- MODULE 3 Infection and Host Resistance PDFDocument22 pagesMODULE 3 Infection and Host Resistance PDFVillanueva, AbegailNo ratings yet
- Chapter 1 - OverviewDocument47 pagesChapter 1 - OverviewZea Mae AgirNo ratings yet
- Lec # 4 Body Defence SystemsDocument31 pagesLec # 4 Body Defence SystemssamotherlianNo ratings yet
- Immunology in the Twentieth Century: From Basic Science to Clinical ApplicationFrom EverandImmunology in the Twentieth Century: From Basic Science to Clinical ApplicationNo ratings yet
- Immunology Unveiled: A Comprehensive Journey through the Human Immune System: Guardians of the Body: The Unseen Heroes of ImmunityFrom EverandImmunology Unveiled: A Comprehensive Journey through the Human Immune System: Guardians of the Body: The Unseen Heroes of ImmunityNo ratings yet
- MICRO BIOLOGY ConjunctivitisDocument5 pagesMICRO BIOLOGY Conjunctivitisbabyko143444No ratings yet
- QC Stock Organism Maintenance ProgramDocument3 pagesQC Stock Organism Maintenance ProgramLiana PergisNo ratings yet
- TH e Curr Icu Lum Ou Tli Ne of Le Mol Ogy: (Temporary Edition)Document36 pagesTH e Curr Icu Lum Ou Tli Ne of Le Mol Ogy: (Temporary Edition)api-3728690No ratings yet
- PolioDocument14 pagesPolioapi-31767091450% (2)
- E2200307.full CHW As VaccinatorsDocument23 pagesE2200307.full CHW As VaccinatorsDavid KanamugireNo ratings yet
- Chapter 19Document16 pagesChapter 19missy23pap100% (1)
- Accomplishment Report On Supervisory Plan Maligaya Elem School June December 2016-2017Document33 pagesAccomplishment Report On Supervisory Plan Maligaya Elem School June December 2016-2017benjamin m. martinez100% (1)
- Health Effects in Vaccinated Versus Unvaccinated ChildrenDocument11 pagesHealth Effects in Vaccinated Versus Unvaccinated ChildrenMahesh JayaramanNo ratings yet
- Steroids PDFDocument12 pagesSteroids PDFRahulNo ratings yet
- UC Davis Koret Shelter Medicine Program - Feline Leukemia Virus (FeLV) - 2012-04-25Document3 pagesUC Davis Koret Shelter Medicine Program - Feline Leukemia Virus (FeLV) - 2012-04-25Kitt KaosNo ratings yet
- Epi NotesDocument5 pagesEpi NoteshoneykrizelNo ratings yet
- Nurhayati, Sudiyati, Erlin Puspita, Siti Rahmadani: Research ArticleDocument4 pagesNurhayati, Sudiyati, Erlin Puspita, Siti Rahmadani: Research ArticleMery Merdiana IsmailNo ratings yet
- Short Covid-19 Dialog 1Document3 pagesShort Covid-19 Dialog 1karin kamilaNo ratings yet
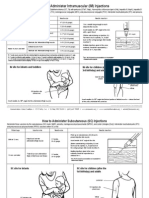
- I/M Injection Sites Acording To AgeDocument2 pagesI/M Injection Sites Acording To Ageman0billiNo ratings yet
- Covid-19 Vaccination Certificate: Vaccinee DetailsDocument1 pageCovid-19 Vaccination Certificate: Vaccinee DetailsSantiago A. de Guzman Elementary SchoolNo ratings yet
- COVID-19 Prevention and Control Quarantine and Border Control ProtocolDocument4 pagesCOVID-19 Prevention and Control Quarantine and Border Control ProtocolTsehaye yonasNo ratings yet
- Benifits of SuvarnaprashanDocument2 pagesBenifits of Suvarnaprashanharish4ayur100% (1)
- Hepatitis B Immunisation ForDocument89 pagesHepatitis B Immunisation ForNacko StavreskiNo ratings yet
- RSRCH DefenseDocument6 pagesRSRCH DefenseKim Pastorin ArogarNo ratings yet
- Rational Use of DrugsDocument3 pagesRational Use of DrugsRphNaeemMalikNo ratings yet
- Operational Guide For Pulse Polio Immunisation in India - 2006Document101 pagesOperational Guide For Pulse Polio Immunisation in India - 2006Dr.Sagindar100% (1)
- Aiims Medical PG May 2014Document19 pagesAiims Medical PG May 2014drpnnreddy100% (1)
- SBO#06 - Anti-Rabies OrdinanceDocument6 pagesSBO#06 - Anti-Rabies OrdinanceLeonardo Miranda BayotasNo ratings yet
- What Is A Cross Infection?Document5 pagesWhat Is A Cross Infection?nandyta febryani100% (2)
- The Doctor Within - 10 Vaccination Is Not Immunization - 2012Document5 pagesThe Doctor Within - 10 Vaccination Is Not Immunization - 2012Cristinel CristeaNo ratings yet
- Rabies Form 1658084407 3529518Document1 pageRabies Form 1658084407 3529518Nicole ComasNo ratings yet
- An 17500Document20 pagesAn 17500nivratNo ratings yet
- Colloidal Silver Cures MRSA ReportDocument16 pagesColloidal Silver Cures MRSA ReportGodwinNo ratings yet