
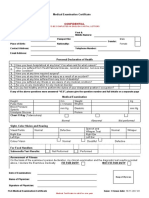
F7.6 Seafarers Medical Examination-Certificate
F7.6 Seafarers Medical Examination-Certificate
You might also like
- MPA-ANNEX B-C - Seafarer Medical Fitness and CertificateDocument6 pagesMPA-ANNEX B-C - Seafarer Medical Fitness and CertificateFred ChowNo ratings yet
- Medical Examinations Form PANAMADocument4 pagesMedical Examinations Form PANAMADany David-Diculescu56% (9)
- Medical Evaluation Form 2022Document2 pagesMedical Evaluation Form 2022jimmy p. lamhi50% (2)
- MLC Medical FormDocument5 pagesMLC Medical FormSoekhaidir SuripnoNo ratings yet
- Medical Examination Certificate: ConfidentialDocument2 pagesMedical Examination Certificate: ConfidentialVioleta100% (1)
- Ibf Jsu Amosup Immaj Cba (2015-2017)Document47 pagesIbf Jsu Amosup Immaj Cba (2015-2017)HaroldRamos100% (1)
- Official Medical Examination Form (2021 GKS-U)Document1 pageOfficial Medical Examination Form (2021 GKS-U)hNo ratings yet
- RCI-CEL-AZA PEME FormA-Rev09-2019 FormB MedCertDocument8 pagesRCI-CEL-AZA PEME FormA-Rev09-2019 FormB MedCertVhal AlbientoNo ratings yet
- Ks 0497 Medical Examination Eng PDFDocument8 pagesKs 0497 Medical Examination Eng PDFIsaNo ratings yet
- Hearing Meets The Section A-L/9?: PractitionerDocument13 pagesHearing Meets The Section A-L/9?: PractitionerRian Daud SadewaNo ratings yet
- Ibf Mui Agreement 2010 2011Document23 pagesIbf Mui Agreement 2010 2011raghuroxxNo ratings yet
- Medical Examination Form SeafarersDocument5 pagesMedical Examination Form SeafarersHazem ElbananNo ratings yet
- Medical Form For Countries That Did Not Ratified MLCDocument1 pageMedical Form For Countries That Did Not Ratified MLCBranimira Dukic BaracNo ratings yet
- Annex 2 - RLM-105M - Rev.12-2017Document2 pagesAnnex 2 - RLM-105M - Rev.12-2017Deany Noor100% (2)
- Medical Certificate For Personnel Service On BoardDocument1 pageMedical Certificate For Personnel Service On BoardMuhammad rizal100% (1)
- Medical Examination Form MLC 2013Document7 pagesMedical Examination Form MLC 2013danadimache100% (4)
- Mpa SC052020 - Mpa Medical FormDocument6 pagesMpa SC052020 - Mpa Medical FormFred ChowNo ratings yet
- 5, Ngaporf Seafarer Reebieael Eerfifieate: Marmme and Port Author!Ty of SlngaporeDocument5 pages5, Ngaporf Seafarer Reebieael Eerfifieate: Marmme and Port Author!Ty of SlngaporeinstalasiNo ratings yet
- Singapore Mpa Medical Oct 2013Document5 pagesSingapore Mpa Medical Oct 2013Nebojsa MijovicNo ratings yet
- Medical Certificate For Service at Sea: ConfidentialDocument4 pagesMedical Certificate For Service at Sea: ConfidentialADMIN MCU RSU SAHID SAHIRMAN100% (1)
- C105a-Pre-Sea-And-Periodic-Medical-Fitness-Examinations-For-Seafarers - by AstroDocument5 pagesC105a-Pre-Sea-And-Periodic-Medical-Fitness-Examinations-For-Seafarers - by Astroklinik utama Bali Puri MedikaNo ratings yet
- Bahamas Medical FormDocument9 pagesBahamas Medical FormКсения ЧучковаNo ratings yet
- Form Malta Medical Cek UpDocument6 pagesForm Malta Medical Cek UpannuryogNo ratings yet
- Peme Reme Form ADocument1 pagePeme Reme Form AClick TechnologyNo ratings yet
- Peme Reme Form ADocument1 pagePeme Reme Form AHector ValleNo ratings yet
- 2013 MedicalsDocument5 pages2013 MedicalsSebastia Felipe SolisNo ratings yet
- Format Pre EmploymentDocument10 pagesFormat Pre EmploymentNurman HidayatNo ratings yet
- Do You Have Did You Ever Have or Have You Been Told You HaveDocument8 pagesDo You Have Did You Ever Have or Have You Been Told You HaveDodi CrossandaNo ratings yet
- Sample Form - New Pre-Employment - MEDEX 001Document3 pagesSample Form - New Pre-Employment - MEDEX 001Helmi C MahadyNo ratings yet
- IMPORTANT: The Original of This Form Is To Be Kept by The Seafarer. A Copy Must Be Kept by The ClinicDocument2 pagesIMPORTANT: The Original of This Form Is To Be Kept by The Seafarer. A Copy Must Be Kept by The ClinicTigreal MLNo ratings yet
- RCL Form A 2020Document4 pagesRCL Form A 2020michael enriquezNo ratings yet
- RCL Employment Medical Examination Form A (New-Returning) Revised 2015-03Document2 pagesRCL Employment Medical Examination Form A (New-Returning) Revised 2015-03Ahmad ShodiqNo ratings yet
- Biennial National Medical ReportDocument5 pagesBiennial National Medical ReportXimena FariasNo ratings yet
- Medical Screening Questionnaire and Examination Record: Social / Occupational History Yes No CommentsDocument4 pagesMedical Screening Questionnaire and Examination Record: Social / Occupational History Yes No CommentsAnnisa DiendaNo ratings yet
- Medical Forms A&BDocument6 pagesMedical Forms A&BMarija CepuloNo ratings yet
- Medical Form For Prospective Recreational Scuba Divers: Candidate Details: This Section To Be Completed by CandidateDocument4 pagesMedical Form For Prospective Recreational Scuba Divers: Candidate Details: This Section To Be Completed by Candidateanon-897008No ratings yet
- HM Medical Checkups at Project Sites Medical CampsDocument2 pagesHM Medical Checkups at Project Sites Medical Campsraj kumariNo ratings yet
- Health DeclarationDocument5 pagesHealth Declarationust dol100% (1)
- CA 67-02 (A)Document4 pagesCA 67-02 (A)Cameron BaxterNo ratings yet
- Medical Fitness Report New For JordanDocument1 pageMedical Fitness Report New For Jordanahmad abdullahNo ratings yet
- Part - 1 (Self Declaration) : Personal DetailsDocument2 pagesPart - 1 (Self Declaration) : Personal DetailsRitesh kumarNo ratings yet
- OGUK Medical FormDocument7 pagesOGUK Medical Formum erNo ratings yet
- Documents MLC Medical ReportDocument3 pagesDocuments MLC Medical ReportSumeet SudNo ratings yet
- Medical Long Form A PDFDocument2 pagesMedical Long Form A PDFGanesh TeenaNo ratings yet
- Medical FormDocument9 pagesMedical Formaosei8185No ratings yet
- TRF For COVID-19 TEST (Coronavirus) : History Yes NoDocument1 pageTRF For COVID-19 TEST (Coronavirus) : History Yes NoRajendra ChavanNo ratings yet
- Medical Examiner'S Confidential ReportDocument2 pagesMedical Examiner'S Confidential ReportParesh BorboruahNo ratings yet
- Interview - Medical Information Please-print-And-signDocument1 pageInterview - Medical Information Please-print-And-signMiloNo ratings yet
- I. Confidential Medical Report Ii. Laboratory Report Iii. X-Ray FormDocument9 pagesI. Confidential Medical Report Ii. Laboratory Report Iii. X-Ray FormAlex BensonNo ratings yet
- مستوصف سمرقند الحديثDocument4 pagesمستوصف سمرقند الحديثالجنيد الطيبNo ratings yet
- Npdmdu Medical Evaluation Form 2023Document2 pagesNpdmdu Medical Evaluation Form 2023Substationsix MalaboncpsNo ratings yet
- Pre Employement Medical Fitness Policy PDFDocument5 pagesPre Employement Medical Fitness Policy PDFShubham SharmaNo ratings yet
- Annexure 1Document8 pagesAnnexure 1Abhas GahlotNo ratings yet
- CSC 03 Seafarers Medical Examination FormDocument2 pagesCSC 03 Seafarers Medical Examination FormAndrew BedwinNo ratings yet
- Medical Form For Pre-Medical EnrollmentDocument1 pageMedical Form For Pre-Medical EnrollmentFrancine Joyce AguilaNo ratings yet
- Declaration of Good Health Form - With Covid QDocument2 pagesDeclaration of Good Health Form - With Covid QRajnish YadavNo ratings yet
- New Health Screening Medical FormDocument4 pagesNew Health Screening Medical Formsalmankhan.484875No ratings yet
- Case SheetDocument9 pagesCase SheetmoghkadayanallurNo ratings yet
- Medical ForDocument8 pagesMedical FormarandugebraNo ratings yet
- RCL Re-Employment Medical Exam FormsDocument5 pagesRCL Re-Employment Medical Exam FormsScias84No ratings yet
- RCL Pre-Employment Medical Exam FormsDocument5 pagesRCL Pre-Employment Medical Exam FormsScias84No ratings yet
- Patient History Edited 2019Document3 pagesPatient History Edited 2019api-468186696No ratings yet
- Importance of The On Board Crew Trainings and Drills For The Improvement of The Vessels' SafetyDocument8 pagesImportance of The On Board Crew Trainings and Drills For The Improvement of The Vessels' SafetyilgarNo ratings yet
- SEAMANSHIPDocument57 pagesSEAMANSHIPrahulrs123483% (6)
- MSC 396Document6 pagesMSC 396Khant PhyoNo ratings yet
- Deck Procedures Manual (DPM)Document344 pagesDeck Procedures Manual (DPM)Gogita Jaiani100% (2)
- MebpDocument3 pagesMebpDiha HabualilahNo ratings yet
- JCMMC No. 03 Series of 2022 1Document19 pagesJCMMC No. 03 Series of 2022 1Jayson Cabello0% (1)
- Introduction To Shipping IndustryDocument21 pagesIntroduction To Shipping IndustryAman GautamNo ratings yet
- Status IMO Documents-XDocument24 pagesStatus IMO Documents-XCristhian Fernando Paz CNo ratings yet
- List of IMO Model CoursesDocument16 pagesList of IMO Model CoursesWilliam JacksonNo ratings yet
- TrainingManual PDFDocument46 pagesTrainingManual PDFSatish DabralNo ratings yet
- Proficiency in Personal Survival Techniques: Model CourseDocument53 pagesProficiency in Personal Survival Techniques: Model CourseKaushik SamantaNo ratings yet
- BSM SM CVDocument36 pagesBSM SM CValexsmn100% (1)
- Agricultural Crops Production NC I CGDocument5 pagesAgricultural Crops Production NC I CGJohnRenzoMolinarNo ratings yet
- Romanian Nautical CollegeDocument24 pagesRomanian Nautical Collegeadrian4fanNo ratings yet
- Minimum Safe Manning Requirements For VesselsDocument31 pagesMinimum Safe Manning Requirements For VesselsRAMSINGH CHAUHANNo ratings yet
- TSM Personnel FormDocument10 pagesTSM Personnel FormMano VijayNo ratings yet
- "Efficient Deck Hand Training Course": The Code of Practice For ConductingDocument18 pages"Efficient Deck Hand Training Course": The Code of Practice For Conductingalonso_rNo ratings yet
- MSI Application Form (ANTIDO)Document7 pagesMSI Application Form (ANTIDO)Raboni AntidoNo ratings yet
- Meo 1 - Question BankDocument81 pagesMeo 1 - Question BankVijai Abraham80% (5)
- Maritime Education and Training in Turkey and Throughout The WorldDocument43 pagesMaritime Education and Training in Turkey and Throughout The Worldkullanici2010No ratings yet
- List of IMO Conventions: Related Protocols Are Referred To Under The Main ConventionDocument3 pagesList of IMO Conventions: Related Protocols Are Referred To Under The Main ConventionhutsonianpNo ratings yet
- Maritime Labour Convention: GuideDocument40 pagesMaritime Labour Convention: GuideVanessa GaringoNo ratings yet
- Crisis Presentation Part 1Document90 pagesCrisis Presentation Part 1Ryuu Yamada100% (2)
- Basic Training For Oil and Chemical Tanker Cargo OperationsDocument240 pagesBasic Training For Oil and Chemical Tanker Cargo Operationsbharatheeeyudu67% (6)
- Ched-Marina Moa PDFDocument45 pagesChed-Marina Moa PDFChes Vergara100% (1)
- 1.1 Overview STCWDocument39 pages1.1 Overview STCWmonica matualageNo ratings yet
- Παραρτήματα 3522.2 08Document23 pagesΠαραρτήματα 3522.2 08VaggelisTragwdosPitsikalisNo ratings yet
- MBE - Students' NotesDocument350 pagesMBE - Students' NotessanjayNo ratings yet























































































Download as pdf or txt
You might also like
- MPA-ANNEX B-C - Seafarer Medical Fitness and CertificateDocument6 pagesMPA-ANNEX B-C - Seafarer Medical Fitness and CertificateFred ChowNo ratings yet
- Medical Examinations Form PANAMADocument4 pagesMedical Examinations Form PANAMADany David-Diculescu56% (9)
- Medical Evaluation Form 2022Document2 pagesMedical Evaluation Form 2022jimmy p. lamhi50% (2)
- MLC Medical FormDocument5 pagesMLC Medical FormSoekhaidir SuripnoNo ratings yet
- Medical Examination Certificate: ConfidentialDocument2 pagesMedical Examination Certificate: ConfidentialVioleta100% (1)
- Ibf Jsu Amosup Immaj Cba (2015-2017)Document47 pagesIbf Jsu Amosup Immaj Cba (2015-2017)HaroldRamos100% (1)
- Official Medical Examination Form (2021 GKS-U)Document1 pageOfficial Medical Examination Form (2021 GKS-U)hNo ratings yet
- RCI-CEL-AZA PEME FormA-Rev09-2019 FormB MedCertDocument8 pagesRCI-CEL-AZA PEME FormA-Rev09-2019 FormB MedCertVhal AlbientoNo ratings yet
- Ks 0497 Medical Examination Eng PDFDocument8 pagesKs 0497 Medical Examination Eng PDFIsaNo ratings yet
- Hearing Meets The Section A-L/9?: PractitionerDocument13 pagesHearing Meets The Section A-L/9?: PractitionerRian Daud SadewaNo ratings yet
- Ibf Mui Agreement 2010 2011Document23 pagesIbf Mui Agreement 2010 2011raghuroxxNo ratings yet
- Medical Examination Form SeafarersDocument5 pagesMedical Examination Form SeafarersHazem ElbananNo ratings yet
- Medical Form For Countries That Did Not Ratified MLCDocument1 pageMedical Form For Countries That Did Not Ratified MLCBranimira Dukic BaracNo ratings yet
- Annex 2 - RLM-105M - Rev.12-2017Document2 pagesAnnex 2 - RLM-105M - Rev.12-2017Deany Noor100% (2)
- Medical Certificate For Personnel Service On BoardDocument1 pageMedical Certificate For Personnel Service On BoardMuhammad rizal100% (1)
- Medical Examination Form MLC 2013Document7 pagesMedical Examination Form MLC 2013danadimache100% (4)
- Mpa SC052020 - Mpa Medical FormDocument6 pagesMpa SC052020 - Mpa Medical FormFred ChowNo ratings yet
- 5, Ngaporf Seafarer Reebieael Eerfifieate: Marmme and Port Author!Ty of SlngaporeDocument5 pages5, Ngaporf Seafarer Reebieael Eerfifieate: Marmme and Port Author!Ty of SlngaporeinstalasiNo ratings yet
- Singapore Mpa Medical Oct 2013Document5 pagesSingapore Mpa Medical Oct 2013Nebojsa MijovicNo ratings yet
- Medical Certificate For Service at Sea: ConfidentialDocument4 pagesMedical Certificate For Service at Sea: ConfidentialADMIN MCU RSU SAHID SAHIRMAN100% (1)
- C105a-Pre-Sea-And-Periodic-Medical-Fitness-Examinations-For-Seafarers - by AstroDocument5 pagesC105a-Pre-Sea-And-Periodic-Medical-Fitness-Examinations-For-Seafarers - by Astroklinik utama Bali Puri MedikaNo ratings yet
- Bahamas Medical FormDocument9 pagesBahamas Medical FormКсения ЧучковаNo ratings yet
- Form Malta Medical Cek UpDocument6 pagesForm Malta Medical Cek UpannuryogNo ratings yet
- Peme Reme Form ADocument1 pagePeme Reme Form AClick TechnologyNo ratings yet
- Peme Reme Form ADocument1 pagePeme Reme Form AHector ValleNo ratings yet
- 2013 MedicalsDocument5 pages2013 MedicalsSebastia Felipe SolisNo ratings yet
- Format Pre EmploymentDocument10 pagesFormat Pre EmploymentNurman HidayatNo ratings yet
- Do You Have Did You Ever Have or Have You Been Told You HaveDocument8 pagesDo You Have Did You Ever Have or Have You Been Told You HaveDodi CrossandaNo ratings yet
- Sample Form - New Pre-Employment - MEDEX 001Document3 pagesSample Form - New Pre-Employment - MEDEX 001Helmi C MahadyNo ratings yet
- IMPORTANT: The Original of This Form Is To Be Kept by The Seafarer. A Copy Must Be Kept by The ClinicDocument2 pagesIMPORTANT: The Original of This Form Is To Be Kept by The Seafarer. A Copy Must Be Kept by The ClinicTigreal MLNo ratings yet
- RCL Form A 2020Document4 pagesRCL Form A 2020michael enriquezNo ratings yet
- RCL Employment Medical Examination Form A (New-Returning) Revised 2015-03Document2 pagesRCL Employment Medical Examination Form A (New-Returning) Revised 2015-03Ahmad ShodiqNo ratings yet
- Biennial National Medical ReportDocument5 pagesBiennial National Medical ReportXimena FariasNo ratings yet
- Medical Screening Questionnaire and Examination Record: Social / Occupational History Yes No CommentsDocument4 pagesMedical Screening Questionnaire and Examination Record: Social / Occupational History Yes No CommentsAnnisa DiendaNo ratings yet
- Medical Forms A&BDocument6 pagesMedical Forms A&BMarija CepuloNo ratings yet
- Medical Form For Prospective Recreational Scuba Divers: Candidate Details: This Section To Be Completed by CandidateDocument4 pagesMedical Form For Prospective Recreational Scuba Divers: Candidate Details: This Section To Be Completed by Candidateanon-897008No ratings yet
- HM Medical Checkups at Project Sites Medical CampsDocument2 pagesHM Medical Checkups at Project Sites Medical Campsraj kumariNo ratings yet
- Health DeclarationDocument5 pagesHealth Declarationust dol100% (1)
- CA 67-02 (A)Document4 pagesCA 67-02 (A)Cameron BaxterNo ratings yet
- Medical Fitness Report New For JordanDocument1 pageMedical Fitness Report New For Jordanahmad abdullahNo ratings yet
- Part - 1 (Self Declaration) : Personal DetailsDocument2 pagesPart - 1 (Self Declaration) : Personal DetailsRitesh kumarNo ratings yet
- OGUK Medical FormDocument7 pagesOGUK Medical Formum erNo ratings yet
- Documents MLC Medical ReportDocument3 pagesDocuments MLC Medical ReportSumeet SudNo ratings yet
- Medical Long Form A PDFDocument2 pagesMedical Long Form A PDFGanesh TeenaNo ratings yet
- Medical FormDocument9 pagesMedical Formaosei8185No ratings yet
- TRF For COVID-19 TEST (Coronavirus) : History Yes NoDocument1 pageTRF For COVID-19 TEST (Coronavirus) : History Yes NoRajendra ChavanNo ratings yet
- Medical Examiner'S Confidential ReportDocument2 pagesMedical Examiner'S Confidential ReportParesh BorboruahNo ratings yet
- Interview - Medical Information Please-print-And-signDocument1 pageInterview - Medical Information Please-print-And-signMiloNo ratings yet
- I. Confidential Medical Report Ii. Laboratory Report Iii. X-Ray FormDocument9 pagesI. Confidential Medical Report Ii. Laboratory Report Iii. X-Ray FormAlex BensonNo ratings yet
- مستوصف سمرقند الحديثDocument4 pagesمستوصف سمرقند الحديثالجنيد الطيبNo ratings yet
- Npdmdu Medical Evaluation Form 2023Document2 pagesNpdmdu Medical Evaluation Form 2023Substationsix MalaboncpsNo ratings yet
- Pre Employement Medical Fitness Policy PDFDocument5 pagesPre Employement Medical Fitness Policy PDFShubham SharmaNo ratings yet
- Annexure 1Document8 pagesAnnexure 1Abhas GahlotNo ratings yet
- CSC 03 Seafarers Medical Examination FormDocument2 pagesCSC 03 Seafarers Medical Examination FormAndrew BedwinNo ratings yet
- Medical Form For Pre-Medical EnrollmentDocument1 pageMedical Form For Pre-Medical EnrollmentFrancine Joyce AguilaNo ratings yet
- Declaration of Good Health Form - With Covid QDocument2 pagesDeclaration of Good Health Form - With Covid QRajnish YadavNo ratings yet
- New Health Screening Medical FormDocument4 pagesNew Health Screening Medical Formsalmankhan.484875No ratings yet
- Case SheetDocument9 pagesCase SheetmoghkadayanallurNo ratings yet
- Medical ForDocument8 pagesMedical FormarandugebraNo ratings yet
- RCL Re-Employment Medical Exam FormsDocument5 pagesRCL Re-Employment Medical Exam FormsScias84No ratings yet
- RCL Pre-Employment Medical Exam FormsDocument5 pagesRCL Pre-Employment Medical Exam FormsScias84No ratings yet
- Patient History Edited 2019Document3 pagesPatient History Edited 2019api-468186696No ratings yet
- Importance of The On Board Crew Trainings and Drills For The Improvement of The Vessels' SafetyDocument8 pagesImportance of The On Board Crew Trainings and Drills For The Improvement of The Vessels' SafetyilgarNo ratings yet
- SEAMANSHIPDocument57 pagesSEAMANSHIPrahulrs123483% (6)
- MSC 396Document6 pagesMSC 396Khant PhyoNo ratings yet
- Deck Procedures Manual (DPM)Document344 pagesDeck Procedures Manual (DPM)Gogita Jaiani100% (2)
- MebpDocument3 pagesMebpDiha HabualilahNo ratings yet
- JCMMC No. 03 Series of 2022 1Document19 pagesJCMMC No. 03 Series of 2022 1Jayson Cabello0% (1)
- Introduction To Shipping IndustryDocument21 pagesIntroduction To Shipping IndustryAman GautamNo ratings yet
- Status IMO Documents-XDocument24 pagesStatus IMO Documents-XCristhian Fernando Paz CNo ratings yet
- List of IMO Model CoursesDocument16 pagesList of IMO Model CoursesWilliam JacksonNo ratings yet
- TrainingManual PDFDocument46 pagesTrainingManual PDFSatish DabralNo ratings yet
- Proficiency in Personal Survival Techniques: Model CourseDocument53 pagesProficiency in Personal Survival Techniques: Model CourseKaushik SamantaNo ratings yet
- BSM SM CVDocument36 pagesBSM SM CValexsmn100% (1)
- Agricultural Crops Production NC I CGDocument5 pagesAgricultural Crops Production NC I CGJohnRenzoMolinarNo ratings yet
- Romanian Nautical CollegeDocument24 pagesRomanian Nautical Collegeadrian4fanNo ratings yet
- Minimum Safe Manning Requirements For VesselsDocument31 pagesMinimum Safe Manning Requirements For VesselsRAMSINGH CHAUHANNo ratings yet
- TSM Personnel FormDocument10 pagesTSM Personnel FormMano VijayNo ratings yet
- "Efficient Deck Hand Training Course": The Code of Practice For ConductingDocument18 pages"Efficient Deck Hand Training Course": The Code of Practice For Conductingalonso_rNo ratings yet
- MSI Application Form (ANTIDO)Document7 pagesMSI Application Form (ANTIDO)Raboni AntidoNo ratings yet
- Meo 1 - Question BankDocument81 pagesMeo 1 - Question BankVijai Abraham80% (5)
- Maritime Education and Training in Turkey and Throughout The WorldDocument43 pagesMaritime Education and Training in Turkey and Throughout The Worldkullanici2010No ratings yet
- List of IMO Conventions: Related Protocols Are Referred To Under The Main ConventionDocument3 pagesList of IMO Conventions: Related Protocols Are Referred To Under The Main ConventionhutsonianpNo ratings yet
- Maritime Labour Convention: GuideDocument40 pagesMaritime Labour Convention: GuideVanessa GaringoNo ratings yet
- Crisis Presentation Part 1Document90 pagesCrisis Presentation Part 1Ryuu Yamada100% (2)
- Basic Training For Oil and Chemical Tanker Cargo OperationsDocument240 pagesBasic Training For Oil and Chemical Tanker Cargo Operationsbharatheeeyudu67% (6)
- Ched-Marina Moa PDFDocument45 pagesChed-Marina Moa PDFChes Vergara100% (1)
- 1.1 Overview STCWDocument39 pages1.1 Overview STCWmonica matualageNo ratings yet
- Παραρτήματα 3522.2 08Document23 pagesΠαραρτήματα 3522.2 08VaggelisTragwdosPitsikalisNo ratings yet
- MBE - Students' NotesDocument350 pagesMBE - Students' NotessanjayNo ratings yet