Download as docx, pdf, or txt
You might also like
- Ranjith ProjectDocument11 pagesRanjith ProjectKumar KumaresanNo ratings yet
- 3BIdMvM5TsW9Xy8kMzZu Baby 4-18 Mo Sleep Guide Baby Sleep Dr. 2021Document98 pages3BIdMvM5TsW9Xy8kMzZu Baby 4-18 Mo Sleep Guide Baby Sleep Dr. 2021dragana novakovic100% (1)
- ER Protocols in The PhilippinesDocument9 pagesER Protocols in The PhilippinesJobelle Acena100% (2)
- Shelby CountyDocument3 pagesShelby CountyFOX13 MemphisNo ratings yet
- Case Study (Lung Cancer)Document17 pagesCase Study (Lung Cancer)Jobelle Acena100% (1)
- Combs G. & Freedman J. (1990) Symbol, Story, and Ceremony - Using Metaphor in Individual and Family TherapyDocument292 pagesCombs G. & Freedman J. (1990) Symbol, Story, and Ceremony - Using Metaphor in Individual and Family TherapyJera Andia100% (1)
- Health Lifestyle TheoryDocument3 pagesHealth Lifestyle Theoryremshop100% (1)
- Laguna State Polytechnic University: College of Nursing and Allied Health A.Y. 2021-22 PurposeDocument4 pagesLaguna State Polytechnic University: College of Nursing and Allied Health A.Y. 2021-22 PurposeKristine Louise JavierNo ratings yet
- 1 Child Abuse Nursing Care Plan PDFDocument7 pages1 Child Abuse Nursing Care Plan PDFMAHESH KOUJALAGINo ratings yet
- Geriatric Case StudyDocument15 pagesGeriatric Case StudyJobelle AcenaNo ratings yet
- Assessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationDocument10 pagesAssessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationJobelle Acena100% (2)
- Price List New-HC Reguler 2019 (3) 1Document5 pagesPrice List New-HC Reguler 2019 (3) 1Nam-Nam SRN NamiraNo ratings yet
- Lesson Plan MDTDocument21 pagesLesson Plan MDTchaitali shankarNo ratings yet
- Spiritual Needs of A Patient With Acute IllnessDocument3 pagesSpiritual Needs of A Patient With Acute IllnessMarimiel PagulayanNo ratings yet
- CoughDocument2 pagesCoughBheru LalNo ratings yet
- Health, Wellness and IllnessDocument4 pagesHealth, Wellness and Illnessmbx47No ratings yet
- Annotated BibliographyDocument4 pagesAnnotated Bibliographymerin sunilNo ratings yet
- Rationale: This Will Assess Pain LevelDocument7 pagesRationale: This Will Assess Pain LevelCoreyNo ratings yet
- Nursing Care Plan No. 1 3Document4 pagesNursing Care Plan No. 1 3Kristina ParasNo ratings yet
- Case Report On Bipolar Affective Disorder: Mania With Psychotic SymptomsDocument2 pagesCase Report On Bipolar Affective Disorder: Mania With Psychotic SymptomskslhfwoiebvNo ratings yet
- Date and Time Objectives Learning Contents Strategies Target Population Resources Evaluation OutcomeDocument8 pagesDate and Time Objectives Learning Contents Strategies Target Population Resources Evaluation OutcometrizzlecNo ratings yet
- Process RecordingDocument9 pagesProcess Recordingnailed_heartNo ratings yet
- NCP OsteomyelitisDocument6 pagesNCP OsteomyelitisRenie SerranoNo ratings yet
- Recreational Therapy Presentee: Sukhdeep Kaur Msc. (N) 1 YearDocument26 pagesRecreational Therapy Presentee: Sukhdeep Kaur Msc. (N) 1 YearSatbir GillNo ratings yet
- Nurse Patient Interaction: I. Background InformationDocument6 pagesNurse Patient Interaction: I. Background InformationLizli LoredoNo ratings yet
- Health AssessmentDocument115 pagesHealth Assessmentteuuuu100% (1)
- NCP of PnuemoniaDocument13 pagesNCP of PnuemoniaFrando kenneth100% (1)
- Bipolar NCPDocument2 pagesBipolar NCPAngel BunolNo ratings yet
- All The Best: Mewar Girls Institute of Nursing, Chittorgarh (Raj.) B.Sc. Nursing II Year II Internal Examination, 2016Document1 pageAll The Best: Mewar Girls Institute of Nursing, Chittorgarh (Raj.) B.Sc. Nursing II Year II Internal Examination, 2016amitNo ratings yet
- Nurse Patient RelationshipDocument29 pagesNurse Patient Relationshipaseel jamalNo ratings yet
- Recreational TherapyDocument22 pagesRecreational TherapyKishore RathoreNo ratings yet
- Health-Perception-Health-Management PatternDocument3 pagesHealth-Perception-Health-Management PatternBela MillenaNo ratings yet
- Role - Responsibilities of Psychiatry Health NurseDocument3 pagesRole - Responsibilities of Psychiatry Health NurseDhAiRyA ArOrANo ratings yet
- Complementary Therapies in NursingDocument12 pagesComplementary Therapies in NursingHamza Ishtiaq100% (1)
- Nursing Care Plan: Nikolai P. Funcion, FSUU-SNDocument5 pagesNursing Care Plan: Nikolai P. Funcion, FSUU-SNNikolai FuncionNo ratings yet
- Assessment Diagnosis Planning Nursing Intervention Rationale EvaluationDocument2 pagesAssessment Diagnosis Planning Nursing Intervention Rationale Evaluationjennelyn losantaNo ratings yet
- NCP Alcoholic NeuropathyDocument5 pagesNCP Alcoholic NeuropathyPeachy Marie Anca100% (1)
- Manaois - SPIRITUALITY IN NURSING QUIZDocument3 pagesManaois - SPIRITUALITY IN NURSING QUIZDan Dan Manaois100% (1)
- Discharge Planning AmangDocument1 pageDischarge Planning AmangMaricris CarranchoNo ratings yet
- Newborn Care: Prepare The (Sterile) Hypo Tray-The Inner Side Is Considered SterileDocument5 pagesNewborn Care: Prepare The (Sterile) Hypo Tray-The Inner Side Is Considered Sterileallkhusairy6tuansiNo ratings yet
- Community Health Nursing Chapter 10Document1 pageCommunity Health Nursing Chapter 10Audrie Allyson GabalesNo ratings yet
- Lumbar Puncture ReportDocument5 pagesLumbar Puncture ReportTweenie DalumpinesNo ratings yet
- Health Teaching Plan CHFDocument3 pagesHealth Teaching Plan CHFInah Floresta Besas100% (1)
- Nursing Care Plan For Low SelfDocument3 pagesNursing Care Plan For Low SelfMarissa AsimNo ratings yet
- Schizophrenia An OverviewDocument12 pagesSchizophrenia An OverviewEriekafebriayana RNo ratings yet
- 1-N 289 Psychosocial Nursing Overview PPT - Copy-2Document14 pages1-N 289 Psychosocial Nursing Overview PPT - Copy-2jaNo ratings yet
- Assessment Diagnosis Rationale Planning Implementation Rationale EvaluationDocument2 pagesAssessment Diagnosis Rationale Planning Implementation Rationale Evaluationkristel_nicole18yahoNo ratings yet
- Tonsilitis NCPDocument2 pagesTonsilitis NCPFATIMA MARYAMA USMANNo ratings yet
- Word Ncp.......... TetanusDocument6 pagesWord Ncp.......... TetanusaianrNo ratings yet
- Process Recording (PR) GuidelinesDocument2 pagesProcess Recording (PR) Guidelinesmrda9228No ratings yet
- NCP Depression1Document1 pageNCP Depression1kyreNo ratings yet
- Discharge PlanningDocument3 pagesDischarge PlanningJemmalyn RonquilloNo ratings yet
- Unit 1 CommunityDocument11 pagesUnit 1 CommunityRija AcharyaNo ratings yet
- Health Education Plan - Case StudyDocument7 pagesHealth Education Plan - Case StudyRenzy Mayven Pedriña LobatonNo ratings yet
- Process Recording, Suicide Assesment and Psyche-Med ConditionDocument44 pagesProcess Recording, Suicide Assesment and Psyche-Med ConditionShy Dela PuertaNo ratings yet
- Fundamental of NursingDocument1 pageFundamental of Nursingioana_ciobincanNo ratings yet
- Nursing Care Plan Marife: 45 Years Old Assessment Diagnosis Background Study/ Planning Implementation Rationale Expected Outcome/ EvaluationDocument6 pagesNursing Care Plan Marife: 45 Years Old Assessment Diagnosis Background Study/ Planning Implementation Rationale Expected Outcome/ EvaluationAngelica Malacay RevilNo ratings yet
- Nursing Care Plan: IndependentDocument1 pageNursing Care Plan: IndependentJay Mar BabateNo ratings yet
- Nursing Care PlanDocument3 pagesNursing Care PlandeliejoyceNo ratings yet
- Nursing Care Plan Assessment Nursing Diagnosis Planning Interventions Rationale EvaluationDocument2 pagesNursing Care Plan Assessment Nursing Diagnosis Planning Interventions Rationale EvaluationValerie FischerNo ratings yet
- Content: Outline Form Only Make A Separate Sheet For The Content. The Health Teaching Plan Should Focus On Home Care For Patients With Mood DisorderDocument4 pagesContent: Outline Form Only Make A Separate Sheet For The Content. The Health Teaching Plan Should Focus On Home Care For Patients With Mood DisorderRaffy Sebastian Seballos100% (1)
- NCP - Anxiety and DepressionDocument2 pagesNCP - Anxiety and DepressionJenny Agustin FabrosNo ratings yet
- Nursing Care Plan, Diagnosis, Interventions Hyperthermia, Fever, High TemperatureDocument2 pagesNursing Care Plan, Diagnosis, Interventions Hyperthermia, Fever, High TemperatureVanessa AbboudNo ratings yet
- Nursing TheoristDocument22 pagesNursing TheoristG a i l R i c h w e l lNo ratings yet
- Nursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDocument4 pagesNursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDimpal ChoudharyNo ratings yet
- Republic of The Philippines University Town, Northern Samar Website: EmailDocument5 pagesRepublic of The Philippines University Town, Northern Samar Website: EmailCzarina Mae Quinones TadeoNo ratings yet
- Self-Care: FirstDocument2 pagesSelf-Care: FirstAllen KateNo ratings yet
- Spirituality and HCDocument27 pagesSpirituality and HCDan Yel YangcoNo ratings yet
- SpiritualityDocument17 pagesSpiritualityNgu W PhooNo ratings yet
- Ethics in Spiritual Nursing CareDocument11 pagesEthics in Spiritual Nursing CareTrixia Nicole B. Salva100% (1)
- Date/Schedule Activities Expected Output Verified/Checked by Area in ChargeDocument2 pagesDate/Schedule Activities Expected Output Verified/Checked by Area in ChargeJobelle AcenaNo ratings yet
- Assessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale Evaluation Short Term Goal Independent: Short Term GoalDocument5 pagesAssessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale Evaluation Short Term Goal Independent: Short Term GoalJobelle AcenaNo ratings yet
- Pediatric Case StudyDocument21 pagesPediatric Case StudyJobelle AcenaNo ratings yet
- NCM 107 Leadership and Management RLEDocument4 pagesNCM 107 Leadership and Management RLEJobelle AcenaNo ratings yet
- Case StudyDocument10 pagesCase StudyJobelle AcenaNo ratings yet
- Union Christian College School of Health and Sciences City of San Fernando La UnionDocument11 pagesUnion Christian College School of Health and Sciences City of San Fernando La UnionJobelle AcenaNo ratings yet
- Subjective: Ventilation AssistanceDocument3 pagesSubjective: Ventilation AssistanceJobelle Acena100% (2)
- DRUG STUDY (Lung Cancer)Document10 pagesDRUG STUDY (Lung Cancer)Jobelle AcenaNo ratings yet
- Online LectureDocument9 pagesOnline LectureJobelle AcenaNo ratings yet
- NCPsDocument11 pagesNCPsJobelle AcenaNo ratings yet
- Drug Study (Pe)Document15 pagesDrug Study (Pe)Jobelle AcenaNo ratings yet
- Er Drugs StudyDocument80 pagesEr Drugs StudyJobelle AcenaNo ratings yet
- Nursing: Core Values of NursingDocument14 pagesNursing: Core Values of NursingJobelle AcenaNo ratings yet
- PHARMAfdDocument7 pagesPHARMAfdJobelle AcenaNo ratings yet
- Psychiatric Nursing Michael Jimenez, PENTAGON Slovin'S Formula: N 1 + NeDocument10 pagesPsychiatric Nursing Michael Jimenez, PENTAGON Slovin'S Formula: N 1 + NeJobelle AcenaNo ratings yet
- Notes On Obstetrics: Normal Labor (Theories of Labor Onset)Document22 pagesNotes On Obstetrics: Normal Labor (Theories of Labor Onset)Jobelle Acena100% (1)
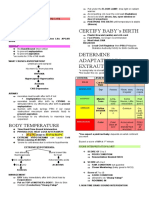
- Certify Baby'S Birth: Body TemperatureDocument9 pagesCertify Baby'S Birth: Body TemperatureJobelle Acena100% (1)
- Assessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationDocument10 pagesAssessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationJobelle AcenaNo ratings yet
- Case Study (Preeclampsia)Document6 pagesCase Study (Preeclampsia)Jobelle AcenaNo ratings yet
- DRUG STUDY (Appendicitis)Document14 pagesDRUG STUDY (Appendicitis)Jobelle AcenaNo ratings yet
- DRUG STUDY (Preeclampsia)Document11 pagesDRUG STUDY (Preeclampsia)Jobelle AcenaNo ratings yet
- Case Study On Pulmonary EmbolismDocument12 pagesCase Study On Pulmonary EmbolismJobelle Acena100% (2)
- F3 Final ExamDocument2 pagesF3 Final Examtombstone.0842No ratings yet
- Meet Indian Genius Who Dropped Out of School at 10, Started His Company at 15, He Is NowDocument8 pagesMeet Indian Genius Who Dropped Out of School at 10, Started His Company at 15, He Is NowBlack Jack 21No ratings yet
- Supercare Medical Services, Inc. Health Declaration Form: Remarks of Examining PhysicianDocument1 pageSupercare Medical Services, Inc. Health Declaration Form: Remarks of Examining PhysicianJunexielJalop100% (1)
- LET Facilitating Learning EDITED3Document12 pagesLET Facilitating Learning EDITED3Likhaan PerformingArts HomeStudio100% (5)
- Chapter 8 Report Writing and Recipient of ReportDocument6 pagesChapter 8 Report Writing and Recipient of Reportrinku jainNo ratings yet
- Netball Practitioner 1Document54 pagesNetball Practitioner 1Ongica SolomonNo ratings yet
- Daily Health Assessment Form - Student and ParentDocument1 pageDaily Health Assessment Form - Student and Parentapi-269483056No ratings yet
- Construction Compendium (Dismantling Scaffolds)Document10 pagesConstruction Compendium (Dismantling Scaffolds)FOZCANNo ratings yet
- Berg and Hayashi 2013 PDFDocument10 pagesBerg and Hayashi 2013 PDFRAMONA GABRIELA LEBADANo ratings yet
- Organizational Behaviour Unit II Values, Attitudes and EmotionsDocument7 pagesOrganizational Behaviour Unit II Values, Attitudes and Emotionspullarao kotaNo ratings yet
- Amoxillin Glimepirid Amoxillin Metronidazol Metformin: Ambroxol Tablet Ambroxol TabletDocument10 pagesAmoxillin Glimepirid Amoxillin Metronidazol Metformin: Ambroxol Tablet Ambroxol TabletSeptia MonalisaNo ratings yet
- Method Statement: Conduit Condition EvaluationDocument21 pagesMethod Statement: Conduit Condition EvaluationAzhar KhanNo ratings yet
- Safety Data Sheet: According To Regulation (EC) No. 1907/2006 (REACH)Document7 pagesSafety Data Sheet: According To Regulation (EC) No. 1907/2006 (REACH)Naishal PatelNo ratings yet
- 1st Quarter 1 CONSUMER HEALTH EDUCATION (Autosaved)Document16 pages1st Quarter 1 CONSUMER HEALTH EDUCATION (Autosaved)JEANY BARROZONo ratings yet
- Parameters of Mechanics of BreathingDocument16 pagesParameters of Mechanics of BreathingKaioNo ratings yet
- Ventilator Cleanroom TypeDocument25 pagesVentilator Cleanroom Typereeta kumariNo ratings yet
- Summary of Amrikology MYDocument1 pageSummary of Amrikology MYHargun ArtNo ratings yet
- ThesisDocument111 pagesThesisVictor AkinseyeNo ratings yet
- SSC 2022 Full Written Part (45marks) Suggestion and Shortcuts by Mr. English Mahmudul HasanDocument11 pagesSSC 2022 Full Written Part (45marks) Suggestion and Shortcuts by Mr. English Mahmudul HasanBMT TCYSNo ratings yet
- BU OP AO No 10 S 2023 Re Guidelines On The Conduct of Full Face-to-Face Classes in BU Starting 2nd Sem SY2022-2023Document5 pagesBU OP AO No 10 S 2023 Re Guidelines On The Conduct of Full Face-to-Face Classes in BU Starting 2nd Sem SY2022-2023Teddy GutayNo ratings yet
- Uv-C TechnologyDocument9 pagesUv-C TechnologyGaurav ZanzadNo ratings yet
- Validity and RealibilityDocument42 pagesValidity and RealibilityKaren AfianNo ratings yet
- Unit 1 - An Introduction To Health Social CareDocument16 pagesUnit 1 - An Introduction To Health Social CareLubalenkosi MliloNo ratings yet
- My Life History (Poster)Document3 pagesMy Life History (Poster)FPagota, Kristine Fe S.No ratings yet