Download as pdf or txt
You might also like
- Nursing Test 4 (NP Iii)Document16 pagesNursing Test 4 (NP Iii)Yuxin Liu100% (2)
- Dream Manager GoalsDocument4 pagesDream Manager Goalsnick445544100% (1)
- PT Consultation FormDocument7 pagesPT Consultation FormRachelNo ratings yet
- Physical Education & HealthDocument16 pagesPhysical Education & HealthRAEJEHL TIMCANGNo ratings yet
- Client Info FormDocument2 pagesClient Info FormkamalsalmanNo ratings yet
- Precision Nutrition Comprehensive Client Information SheetDocument5 pagesPrecision Nutrition Comprehensive Client Information SheetStew Houston100% (3)
- Precision Nutrition Comprehensive Client Information Sheet PDFDocument5 pagesPrecision Nutrition Comprehensive Client Information Sheet PDFJosh WarrellNo ratings yet
- Health Assessment Form (Non SDAs)Document11 pagesHealth Assessment Form (Non SDAs)Christine Guardo100% (1)
- Ar Wellness Assessment FormDocument11 pagesAr Wellness Assessment FormRafique Sumardi Omar67% (3)
- Personal Fitness Unit PlanDocument54 pagesPersonal Fitness Unit PlanCarrie Blais100% (3)
- Personal Fitness WorkbookDocument13 pagesPersonal Fitness WorkbookScott KramerNo ratings yet
- Retention in Complete DentureDocument53 pagesRetention in Complete DentureVikas Aggarwal67% (3)
- Dihybrid Cross PracticeDocument3 pagesDihybrid Cross PracticeMark Davis100% (1)
- Client Intake FormsDocument5 pagesClient Intake FormsGuillaume VingtcentNo ratings yet
- DH Health Assessment FormDocument3 pagesDH Health Assessment FormRayceNo ratings yet
- PE and Health ModuleDocument17 pagesPE and Health ModuleTessaKaye AlfaroNo ratings yet
- Personal Physical Fitness Plan PacketDocument10 pagesPersonal Physical Fitness Plan Packetsavafut2No ratings yet
- HOPE 3 Module 1Document37 pagesHOPE 3 Module 1Deey Lanne Casuga RufintaNo ratings yet
- HOPE 4 Module 1Document37 pagesHOPE 4 Module 1Lei Dulay90% (10)
- Statement of The ProblemDocument2 pagesStatement of The ProblemMeiria Anika Gail Fabian SalangsangNo ratings yet
- Pe 10 Law Q2 21-22 PDFDocument8 pagesPe 10 Law Q2 21-22 PDFLEODE JOY TULANGNo ratings yet
- Answer Sheet Week 5-6Document2 pagesAnswer Sheet Week 5-6Josefina GuintoNo ratings yet
- CF 4820 Screening Rules Wavier 14 March 2015Document7 pagesCF 4820 Screening Rules Wavier 14 March 2015api-138096780No ratings yet
- Exercise History and Attitude QuestionnaireDocument3 pagesExercise History and Attitude Questionnaireapi-138865155No ratings yet
- Fitness Testing and Basic Exercise Programming: Self Learning Module inDocument26 pagesFitness Testing and Basic Exercise Programming: Self Learning Module inPaula Dimples Santiago100% (1)
- Grade 5 Science Weeks 1-4 Worksheets - Term 1Document25 pagesGrade 5 Science Weeks 1-4 Worksheets - Term 1darrengotta8No ratings yet
- Client Initial Assessment Worksheet: How Did You Here About Us or Who Referred You?Document5 pagesClient Initial Assessment Worksheet: How Did You Here About Us or Who Referred You?api-335005776No ratings yet
- Bariatric Food and Nutrition History 5-2019Document2 pagesBariatric Food and Nutrition History 5-2019klgonzalezNo ratings yet
- New Member Intake Form: Personal InformationDocument3 pagesNew Member Intake Form: Personal InformationRui CunhaNo ratings yet
- ErgonDocument2 pagesErgonjohnpodojil101No ratings yet
- GFHP QuestionsDocument16 pagesGFHP QuestionsaviaquaNo ratings yet
- Lab4.4 - Resistance Training Plan - Banderson PDFDocument3 pagesLab4.4 - Resistance Training Plan - Banderson PDFBraelyn AndersonNo ratings yet
- Fitness Lifestyle JournalDocument14 pagesFitness Lifestyle Journaljstorm100% (1)
- National Christian Life College: Physical Education and Health 12 WORKSHEETDocument6 pagesNational Christian Life College: Physical Education and Health 12 WORKSHEETVon bhrianeNo ratings yet
- Protein Bar Whey/Egg/Mix Protein Protein Drink:) Supported by University of Palermo and University of PaduaDocument2 pagesProtein Bar Whey/Egg/Mix Protein Protein Drink:) Supported by University of Palermo and University of PaduakalikNo ratings yet
- Gordons Functional Health Patterns Assessment 1Document11 pagesGordons Functional Health Patterns Assessment 1Katherine Lizell Lopez100% (1)
- Personal Fitness MBDocument14 pagesPersonal Fitness MBtom2susanNo ratings yet
- Trainee's ProfileDocument2 pagesTrainee's ProfileArvin CruzNo ratings yet
- Personal FitnessDocument14 pagesPersonal FitnessW4NRNo ratings yet
- Learning Guide Physical Education 11 Grade 11-Abm/Humss/Stem SY: 2020-2021Document12 pagesLearning Guide Physical Education 11 Grade 11-Abm/Humss/Stem SY: 2020-2021akaiaNo ratings yet
- Systems of Knowledge SurveyDocument2 pagesSystems of Knowledge SurveymarscibNo ratings yet
- NB AssessmentDocument6 pagesNB AssessmentstephanyNo ratings yet
- PE and Health 12 - Module 1Document39 pagesPE and Health 12 - Module 1Stephen Lorenzo A. Doria100% (1)
- 1 Year Omt Florence Claire D. Calutan: - 6. Time Is Also Dependent On The Intensity of Your Work-OutDocument4 pages1 Year Omt Florence Claire D. Calutan: - 6. Time Is Also Dependent On The Intensity of Your Work-Outjumel delunaNo ratings yet
- Health History Assessment ToolDocument3 pagesHealth History Assessment ToolDaniela Suarez NimNo ratings yet
- Pe & Health 11 Finals Activity 2 Developing A Homebased Family WorkoutDocument3 pagesPe & Health 11 Finals Activity 2 Developing A Homebased Family WorkoutRyan BersaminNo ratings yet
- Week 1-2 Wuarter 3Document11 pagesWeek 1-2 Wuarter 3Josefina GuintoNo ratings yet
- Attachment P.EDocument2 pagesAttachment P.EMichelle Wendy Y. VenturaNo ratings yet
- Secondary 3: Module 2 Level 2Document8 pagesSecondary 3: Module 2 Level 2crystaltang570No ratings yet
- (Include State, City, Zip Code) :: HH Forms 570307 N08/06 Printed by The Digital Print Center at HHDocument8 pages(Include State, City, Zip Code) :: HH Forms 570307 N08/06 Printed by The Digital Print Center at HHadil shabbirNo ratings yet
- Let's Get It On!: Arellano University 3058 Taft Avenue, Pasay CityDocument4 pagesLet's Get It On!: Arellano University 3058 Taft Avenue, Pasay CityRosé StylesNo ratings yet
- Chnursing NotesDocument21 pagesChnursing Notesjimmy boy canlas jrNo ratings yet
- Initial Nutrition AssessmentDocument7 pagesInitial Nutrition Assessmenthabiba arifNo ratings yet
- Hyde Square Task Force Youth Leadership ApplicationDocument9 pagesHyde Square Task Force Youth Leadership ApplicationKaren BossNo ratings yet
- Personalized Exercise Program Questionnaire: Bangor YmcaDocument4 pagesPersonalized Exercise Program Questionnaire: Bangor YmcaSusan MatayonNo ratings yet
- Setting Exercise and Fitness GoalsDocument8 pagesSetting Exercise and Fitness Goalstim csNo ratings yet
- Health and Nutrition History Client Information: Today's DateDocument6 pagesHealth and Nutrition History Client Information: Today's DateMalaika ShaikhNo ratings yet
- Tutoring IntakeDocument7 pagesTutoring Intakeapi-279821501No ratings yet
- Hope1 Q1LC4 Week 5Document12 pagesHope1 Q1LC4 Week 5ByeonNo ratings yet
- Worksheet 1Document2 pagesWorksheet 1Raging PotatoNo ratings yet
- Confidential Parent Occupational Physical Therapy 01 15Document7 pagesConfidential Parent Occupational Physical Therapy 01 15Giselle Pezoa WattsonNo ratings yet
- Strength Training For Runners: 3 Basics Of Weight Training For RunnersFrom EverandStrength Training For Runners: 3 Basics Of Weight Training For RunnersNo ratings yet
- Auxiliary PowerDocument29 pagesAuxiliary PowerManoj UpadhyayNo ratings yet
- CPC CC Hydraulic Cable Cutting Tools SeriesDocument0 pagesCPC CC Hydraulic Cable Cutting Tools SeriesbaolifengNo ratings yet
- Nebosh International Diploma ID1Document6 pagesNebosh International Diploma ID1Haltebaye Djim RahmNo ratings yet
- Electrical License Examination Guide: 20210211 - Licensingexaminationguide Checked 20210211Document33 pagesElectrical License Examination Guide: 20210211 - Licensingexaminationguide Checked 20210211paddyNo ratings yet
- Laughter Is Best Essay OtherDocument2 pagesLaughter Is Best Essay OtherArchana SharmaNo ratings yet
- Performance Appraisal SystemDocument13 pagesPerformance Appraisal SystemAli AsgarNo ratings yet
- Standard Test Method For Moisture in The Analysis Sample of Coal and CokeDocument7 pagesStandard Test Method For Moisture in The Analysis Sample of Coal and CokemuchtarNo ratings yet
- AppetizerDocument47 pagesAppetizerCecelle BaluarteNo ratings yet
- Field ParasitologyDocument73 pagesField ParasitologyMALIK WASEEM ABBASNo ratings yet
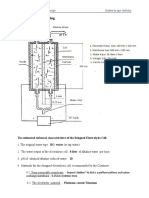
- Elecrolysis Cell DrawingDocument2 pagesElecrolysis Cell DrawingRimaNo ratings yet
- Navi Gi PolicyDocumentSA006T0VDocument25 pagesNavi Gi PolicyDocumentSA006T0Vdattam venkateswarluNo ratings yet
- Research On:: Department of English Language Faculty of Arts University of KordofanDocument49 pagesResearch On:: Department of English Language Faculty of Arts University of KordofanMr DragonNo ratings yet
- INTRODUCTION of Digital RecruitmentDocument11 pagesINTRODUCTION of Digital Recruitmentpawan bathamNo ratings yet
- Automatic Bottle Washing Machine-NewDocument5 pagesAutomatic Bottle Washing Machine-Newsathish kumarNo ratings yet
- Pe 610 Waiver Reflection PaperDocument2 pagesPe 610 Waiver Reflection Paperapi-459743145No ratings yet
- Related SrudiesDocument103 pagesRelated SrudiesMichael BiaNo ratings yet
- 780B-780C Spec (99014) D.1Document1 page780B-780C Spec (99014) D.1Cristobal ArayaNo ratings yet
- Week 9 Activity - Concepts On The CPS Exam Rebecca Miller Commercial Law LEG565 Professor Lori Baggot March 4, 2022Document3 pagesWeek 9 Activity - Concepts On The CPS Exam Rebecca Miller Commercial Law LEG565 Professor Lori Baggot March 4, 2022Rebecca Miller HorneNo ratings yet
- Process and Material Specification: AIPI05-03-006 01-02-71 A1 FEB 01/21Document17 pagesProcess and Material Specification: AIPI05-03-006 01-02-71 A1 FEB 01/21schembriryanNo ratings yet
- Earthquake Preparedness: Emergency Plan: What To Do Before An Earthquake - Be Prepared!Document16 pagesEarthquake Preparedness: Emergency Plan: What To Do Before An Earthquake - Be Prepared!Lenaj EbronNo ratings yet
- Importance of SleepDocument10 pagesImportance of SleepKopano'Gucci'ModisenyaneNo ratings yet
- CN3083 - Lithium Ion Battery Charger For Solar-Powered SystemsDocument11 pagesCN3083 - Lithium Ion Battery Charger For Solar-Powered Systemsabyscott19No ratings yet
- HCL Sap Means in Self Declaration FormDocument13 pagesHCL Sap Means in Self Declaration FormdrdomarkNo ratings yet
- Insurance LawDocument15 pagesInsurance LawShruti KambleNo ratings yet
- August 2012Document19 pagesAugust 2012TheUnknown LyssNo ratings yet
- 10.01.2011/EN FCI-Standard #149: Federation Cynologique Internationale (Aisbl)Document6 pages10.01.2011/EN FCI-Standard #149: Federation Cynologique Internationale (Aisbl)Domingos CunhaNo ratings yet
- Calamities in PhilippinesDocument44 pagesCalamities in PhilippinesMic BaldevaronaNo ratings yet