Download as pdf or txt
You might also like
- Fractures Related To Occlusal Overload With Single Posterior Implants A Clinical ReportDocument6 pagesFractures Related To Occlusal Overload With Single Posterior Implants A Clinical ReportSurya TejaNo ratings yet
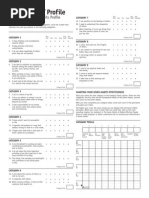
- 7 Habits ProfileDocument1 page7 Habits Profilesigal ardanNo ratings yet
- Tibial Non UnionsDocument9 pagesTibial Non UnionsluckyariadneeNo ratings yet
- Orthopaedic Clinic of Patras University, University Hospital, 26505 Rion Patras, GreeceDocument8 pagesOrthopaedic Clinic of Patras University, University Hospital, 26505 Rion Patras, Greecemasyuni cantika sariNo ratings yet
- Femoral Head Osteonecrosis Why Choose FreeDocument6 pagesFemoral Head Osteonecrosis Why Choose FreeFreestanding identificationNo ratings yet
- Humeral Non UnionDocument12 pagesHumeral Non Unionmmqk122No ratings yet
- Hume Ro Prox SutDocument15 pagesHume Ro Prox Sutbenife8420No ratings yet
- Stress Modulation of Fracture Fixation Implants: Review ArticleDocument9 pagesStress Modulation of Fracture Fixation Implants: Review ArticleAnonymous kdBDppigENo ratings yet
- Management of Aseptic Tibial NonunionDocument11 pagesManagement of Aseptic Tibial NonunionJawad KhanNo ratings yet
- Biomechanics of Locked Plates and ScrewsDocument6 pagesBiomechanics of Locked Plates and Screwsd_muamer_116983894No ratings yet
- Meniscal Repair'starke 2009Document12 pagesMeniscal Repair'starke 2009yoel mitreNo ratings yet
- AO Principles of Fracture Management - 3rd Ed. - Thieme - 2017Document7 pagesAO Principles of Fracture Management - 3rd Ed. - Thieme - 2017Roberto GuanipaNo ratings yet
- Nonunion of FracturesDocument43 pagesNonunion of FracturessharenNo ratings yet
- 17 - Distal Radius FracturesDocument78 pages17 - Distal Radius FracturesFlorin Panduru100% (1)
- Comminuted Intraarticular Fractures of The Tibial Plateau Lead To Posttraumatic Osteoarthritis of The Knee: Current Treatment ReviewDocument7 pagesComminuted Intraarticular Fractures of The Tibial Plateau Lead To Posttraumatic Osteoarthritis of The Knee: Current Treatment ReviewGustavoBecerraNo ratings yet
- Revisión Nature 2012Document11 pagesRevisión Nature 2012Pedro TorresNo ratings yet
- Tibial No UnionDocument8 pagesTibial No Unionjuan pagesNo ratings yet
- Aosm004 01 01Document12 pagesAosm004 01 01elhadidimahmoudNo ratings yet
- Calcaneal Fractures. Which Approach For Which Fracture. Orthop Clin N Am 52 (2021)Document18 pagesCalcaneal Fractures. Which Approach For Which Fracture. Orthop Clin N Am 52 (2021)Un SerNo ratings yet
- Pi Is 1043181008000225Document5 pagesPi Is 1043181008000225drbhaskar128No ratings yet
- Mandible FracturesDocument17 pagesMandible FracturesYaser JasNo ratings yet
- CH 20Document98 pagesCH 20nhieuntnNo ratings yet
- Secondary Healing Occurs in Fractures Treated With Stress Sharing Devices Such As CastsDocument4 pagesSecondary Healing Occurs in Fractures Treated With Stress Sharing Devices Such As CastsYuva RajaNo ratings yet
- Our Experience With Operative Treatment of Intra-Articular Calcaneal Fractures With Calcaneal PlatesDocument4 pagesOur Experience With Operative Treatment of Intra-Articular Calcaneal Fractures With Calcaneal PlatesBs. Hoàng AnhNo ratings yet
- Optimizing Stability in Distal Humeral Fracture Fixation: Historical PerspectiveDocument9 pagesOptimizing Stability in Distal Humeral Fracture Fixation: Historical PerspectiveNazir KhanNo ratings yet
- Femoral Neck Nonunion, Osteotomy and ArthroplastyDocument9 pagesFemoral Neck Nonunion, Osteotomy and ArthroplastyAndrés KnubelNo ratings yet
- Mandibular Implat RetainedDocument6 pagesMandibular Implat RetainedMaria Fernanda Samaniego MorochoNo ratings yet
- Evolution of Internal Fixation in Long Bone FracturesDocument18 pagesEvolution of Internal Fixation in Long Bone FracturesTraumatologia HEBANo ratings yet
- Bone Marrow Stimulation and Biological Adjuncts For Treatment of Osteochondral Lesions of The TalusDocument12 pagesBone Marrow Stimulation and Biological Adjuncts For Treatment of Osteochondral Lesions of The TalusAnonymous kdBDppigENo ratings yet
- Meniscal Root Injuries.3Document9 pagesMeniscal Root Injuries.3cooperorthopaedicsNo ratings yet
- 2021 Acetabular Wear in THADocument9 pages2021 Acetabular Wear in THAilanNo ratings yet
- D5DADocument3 pagesD5DAdemoaccount demoNo ratings yet
- 2001 - Cartilage Substitutes - Overview of Basic Science and Treatment OptionsDocument16 pages2001 - Cartilage Substitutes - Overview of Basic Science and Treatment Optionsgrofecbio1No ratings yet
- Article PDFDocument5 pagesArticle PDFLauren LimNo ratings yet
- Controversiesin Traditionaloraland MaxillofacialreconstructionDocument13 pagesControversiesin Traditionaloraland MaxillofacialreconstructionSheetal HNo ratings yet
- Cartilage Injury in The Knee Assessment And.2Document9 pagesCartilage Injury in The Knee Assessment And.2cooperorthopaedicsNo ratings yet
- Meniscal Root Tears - Solving The Silent EpidemicDocument11 pagesMeniscal Root Tears - Solving The Silent EpidemicJake sanchezNo ratings yet
- Internal Fixation of Distal Fibula Fractures JFAS 1995Document9 pagesInternal Fixation of Distal Fibula Fractures JFAS 1995Evan BowlesNo ratings yet
- Femoral Neck Fractures in Young Patients State Of.3Document5 pagesFemoral Neck Fractures in Young Patients State Of.3Rizwan Ahamed T ANo ratings yet
- Fractures of The Tibial PlafondDocument21 pagesFractures of The Tibial PlafondCamila FontechaNo ratings yet
- Successful Outcome With Minimally Invasive Plate Osteosynthesis For Periprosthetic Tibial Fracture After Total Knee ArthroplastyDocument6 pagesSuccessful Outcome With Minimally Invasive Plate Osteosynthesis For Periprosthetic Tibial Fracture After Total Knee ArthroplastyMohebNo ratings yet
- Functional Bracing Fractures PDFDocument10 pagesFunctional Bracing Fractures PDFPPVRM100% (1)
- The Mechanics of External Fixation-YaDocument17 pagesThe Mechanics of External Fixation-Yalucky sevenNo ratings yet
- Total Knee Arthroplasty in Osteopetrosis Using Patient-Specific InstrumentationDocument4 pagesTotal Knee Arthroplasty in Osteopetrosis Using Patient-Specific InstrumentationDavidBeatonComuladaNo ratings yet
- Os 13 1465Document9 pagesOs 13 1465Mar HernandezNo ratings yet
- Manuscript ARMDocument11 pagesManuscript ARMMahardika PutraNo ratings yet
- Surgical Stabilization of SpineDocument4 pagesSurgical Stabilization of SpineMaria Jonnalin SantosNo ratings yet
- Osteop Intl 07Document9 pagesOsteop Intl 07szarysimbaNo ratings yet
- Hofstetter 2014Document7 pagesHofstetter 2014HCP 89No ratings yet
- Fai 2009 0142Document8 pagesFai 2009 0142Mohamed GoudaNo ratings yet
- Posterior Malleolus Fractures: AnnotationDocument7 pagesPosterior Malleolus Fractures: AnnotationFrigandraSyahputriNo ratings yet
- PRD 88 116Document14 pagesPRD 88 116Gt SolarcNo ratings yet
- Manejo 3Document15 pagesManejo 3Gt SolarcNo ratings yet
- Chapter 13Document58 pagesChapter 13Yaser JasNo ratings yet
- Effects of Mechanical Factors On The Fracture Healing ProcessDocument16 pagesEffects of Mechanical Factors On The Fracture Healing ProcessBastion ReinhartNo ratings yet
- Metal AnchorsDocument3 pagesMetal AnchorsMarcelo Wiltemburg AlvesNo ratings yet
- Bone Graft AssingmentDocument4 pagesBone Graft AssingmentNyein Chan AungNo ratings yet
- Currentconceptsof Femoroacetabular Impingement: Aria Ghaffari,, Ivan Davis,, Troy Storey,, Michael MoserDocument18 pagesCurrentconceptsof Femoroacetabular Impingement: Aria Ghaffari,, Ivan Davis,, Troy Storey,, Michael MosertanyasisNo ratings yet
- Cavanaugh, J. (2014) - Rehabilitation of Meniscal Injury and Surgery. Journal of Knee SurgeryDocument20 pagesCavanaugh, J. (2014) - Rehabilitation of Meniscal Injury and Surgery. Journal of Knee SurgeryDanijela HalilovićNo ratings yet
- Fractures of Thetibial PlafondDocument21 pagesFractures of Thetibial PlafondMario Esteban Muñoz RojasNo ratings yet
- Peri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentFrom EverandPeri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentNo ratings yet
- CTS Sample QuestionsDocument30 pagesCTS Sample Questionsகார்த்திகேயன் பழனிச்சாமிNo ratings yet
- A Study On Consumer Buying Behaviour On Honda Motor CyclesDocument38 pagesA Study On Consumer Buying Behaviour On Honda Motor CyclesNaga Jyothi Kiran BusamNo ratings yet
- FinGAT Financial Graph Attention Networks For Recommending Top-KK Profitable StocksDocument13 pagesFinGAT Financial Graph Attention Networks For Recommending Top-KK Profitable StocksSivaramakrishnan KanagarajNo ratings yet
- Dbs Group Data Anaytics in Audit CS CleanDocument12 pagesDbs Group Data Anaytics in Audit CS CleanJustine LinNo ratings yet
- Effects of Different Charcoal Concentration On The Growth and Yield of Okra PlantDocument2 pagesEffects of Different Charcoal Concentration On The Growth and Yield of Okra PlantWahahahaha suck my dickNo ratings yet
- Electronics Media Internship Report ZEE NEWS CGDocument15 pagesElectronics Media Internship Report ZEE NEWS CGPrashant PandyaNo ratings yet
- Quantum Grover Algorithm SearchDocument23 pagesQuantum Grover Algorithm SearchSaif HassanNo ratings yet
- Mobile Broadband For Emerging Markets 2011 Programme CoverDocument2 pagesMobile Broadband For Emerging Markets 2011 Programme Covereugene_azucenaNo ratings yet
- Acer 1Document2 pagesAcer 1limsoonkiong4823No ratings yet
- AD22650 EliteSemiconductorDocument24 pagesAD22650 EliteSemiconductorpauloNo ratings yet
- Defence Account CodeDocument41 pagesDefence Account Codem kNo ratings yet
- Centrifugal Compressor Pulsation-Vibration ProblemsDocument4 pagesCentrifugal Compressor Pulsation-Vibration ProblemszaidbismaNo ratings yet
- Firstbeat Sports System Data Sheet ENG 09 2018Document2 pagesFirstbeat Sports System Data Sheet ENG 09 2018Antonio JairoNo ratings yet
- Omron Cp1l El M UsersmanualDocument800 pagesOmron Cp1l El M Usersmanualarmandoa71565No ratings yet
- Air Conditioning System For Your CarDocument9 pagesAir Conditioning System For Your CarSanjeev GuptaNo ratings yet
- A. Globalization and Multicultural LiteracyDocument7 pagesA. Globalization and Multicultural LiteracySarah YumulNo ratings yet
- Peavey Rockmaster PreampDocument1 pagePeavey Rockmaster PreampFrancisco FerrerNo ratings yet
- PPA115D-TRO115D Issue 2 Umsebenzi - LODDocument7 pagesPPA115D-TRO115D Issue 2 Umsebenzi - LODGontse DubeNo ratings yet
- PH NR 01 en PDFDocument111 pagesPH NR 01 en PDFKristiane Reyes De VillaNo ratings yet
- Writing A Marketing Research ReportDocument9 pagesWriting A Marketing Research Reportaprille altNo ratings yet
- BS en 00040-3-1-2000 PDFDocument22 pagesBS en 00040-3-1-2000 PDFShan Sandaruwan AbeywardeneNo ratings yet
- Electrical Conductivity and Resistivity of Water: Standard Test Methods ForDocument8 pagesElectrical Conductivity and Resistivity of Water: Standard Test Methods ForAngel MurilloNo ratings yet
- Receiverbook - Online Receiver Directory - HomeDocument1 pageReceiverbook - Online Receiver Directory - Homekennymckornic5334No ratings yet
- Theory Critique NursingDocument4 pagesTheory Critique NursingLowellaJulioNo ratings yet
- Fms BulletinDocument31 pagesFms BulletinalphaNo ratings yet
- Practice-Design Patterns PDFDocument10 pagesPractice-Design Patterns PDFوسيلة قندوزيNo ratings yet
- Dynamic ProgrammingDocument23 pagesDynamic ProgrammingHydroNo ratings yet
- Amps Flat GainDocument3 pagesAmps Flat GainJaime Misael JalifeNo ratings yet
- Northwestern University, Inc: Laoag City, Ilocos NorteDocument3 pagesNorthwestern University, Inc: Laoag City, Ilocos NorteAlex MarcosNo ratings yet