Download as pdf or txt
You might also like
- Atomic Habits - SuperSummary Study GuideDocument64 pagesAtomic Habits - SuperSummary Study GuideNiniNo ratings yet
- TYBCOM-Sem5 Notes 2022 1Document30 pagesTYBCOM-Sem5 Notes 2022 1jay100% (3)
- Ec6 Telangana PDFDocument673 pagesEc6 Telangana PDFshyam143225No ratings yet
- Haikal Rozi Amanda 352 1e Resume Artikel PromkesDocument4 pagesHaikal Rozi Amanda 352 1e Resume Artikel PromkesHaikal AmandaNo ratings yet
- N Acetylcysteine For Therapy Resistant Tobacco Use Disorder A Pilot StudyDocument9 pagesN Acetylcysteine For Therapy Resistant Tobacco Use Disorder A Pilot Studytami syhabNo ratings yet
- Effectiveness of School-Based Smoking Prevention Curricula: Systematic Review and Meta-AnalysisDocument16 pagesEffectiveness of School-Based Smoking Prevention Curricula: Systematic Review and Meta-AnalysisClaudiaGárateHenríquezNo ratings yet
- Smoke-Free Policies in The Global South: Nicotine & Tobacco Research October 2020Document3 pagesSmoke-Free Policies in The Global South: Nicotine & Tobacco Research October 2020Ankita RanaNo ratings yet
- Intervention For Smoking ReductionDocument15 pagesIntervention For Smoking Reductionben mwanziaNo ratings yet
- Path StudyDocument9 pagesPath StudyROSADA PIETRONo ratings yet
- Drug and Alcohol DependenceDocument7 pagesDrug and Alcohol DependenceNur Melizza, S.Kep., NsNo ratings yet
- Estudio Uso THCDocument16 pagesEstudio Uso THCMax Möller ZamoranoNo ratings yet
- Attitude Towards Second Hand Smoke, Smoking and QuitingDocument5 pagesAttitude Towards Second Hand Smoke, Smoking and QuitingBaonganNo ratings yet
- Shantal Mang InasalDocument7 pagesShantal Mang InasalShantal EsperaNo ratings yet
- Jurnal Bing 3Document11 pagesJurnal Bing 3Abangnya Dea AmandaNo ratings yet
- Cursuri EpidemioDocument824 pagesCursuri EpidemioMalina GaborNo ratings yet
- Jurnal WCU 090416.Document5 pagesJurnal WCU 090416.Alfitri YuniNo ratings yet
- A Population Level Analysis of Changes in AustraliDocument17 pagesA Population Level Analysis of Changes in AustraliYuning tyas Nursyah FitriNo ratings yet
- Research PaperDocument34 pagesResearch PaperTrisha AlegrosNo ratings yet
- Add 12140Document9 pagesAdd 12140imadhassanNo ratings yet
- Smoking Restrictions and Treatment For Smoking: Policies and Procedures in Psychiatric Inpatient Units in AustraliaDocument9 pagesSmoking Restrictions and Treatment For Smoking: Policies and Procedures in Psychiatric Inpatient Units in AustraliayasernetNo ratings yet
- 2012 - Craig - J Epi Com Health - Using Natural Experiments To Evaluate Population Health InterventionsDocument5 pages2012 - Craig - J Epi Com Health - Using Natural Experiments To Evaluate Population Health InterventionsnomdeplumNo ratings yet
- Smoking Cessation in Age Initiation and Other Suspected InfluencesDocument7 pagesSmoking Cessation in Age Initiation and Other Suspected InfluencesFilip RalucaNo ratings yet
- Substance Use and Recidivism Outcomes For Prison-Based Drug and Alcohol Interventions-FinalDocument19 pagesSubstance Use and Recidivism Outcomes For Prison-Based Drug and Alcohol Interventions-FinalFelix Omondi SceneryNo ratings yet
- Determinants of Mental Health and Abuse of Psychoactive Substances Associated With Tobacco Use. A Case-Control StudyDocument12 pagesDeterminants of Mental Health and Abuse of Psychoactive Substances Associated With Tobacco Use. A Case-Control Studymodesto66No ratings yet
- Chapter 3Document3 pagesChapter 3Cayanong Joel Jr I.No ratings yet
- Evaluation of Smoking Cessation Success in AdultsDocument8 pagesEvaluation of Smoking Cessation Success in AdultsSISNo ratings yet
- Review of Related LiteratureDocument5 pagesReview of Related Literaturesigfridmonte68% (28)
- Nursing Intervention and Smoking Cessation: A Meta-AnalysisDocument17 pagesNursing Intervention and Smoking Cessation: A Meta-AnalysisingevelystareslyNo ratings yet
- Hidden Risks Associated With Clinical Trials in Developing CountriesDocument6 pagesHidden Risks Associated With Clinical Trials in Developing CountriesSophiaNo ratings yet
- A Uri Kulot Era PijaDocument10 pagesA Uri Kulot Era PijaGg KNo ratings yet
- E-Cigarette Awareness, Use, and Harm Perceptions in US AdultsDocument9 pagesE-Cigarette Awareness, Use, and Harm Perceptions in US AdultsJimin ParkNo ratings yet
- Nursing Research Paper Final DraftDocument15 pagesNursing Research Paper Final Draftapi-593455086No ratings yet
- Global Health Professions Student Survey Turkey: Second-Hand Smoke Exposure and Opinions of Medical Students On Anti-Tobacco LawDocument6 pagesGlobal Health Professions Student Survey Turkey: Second-Hand Smoke Exposure and Opinions of Medical Students On Anti-Tobacco LawTwiebie Sejhathy TacxingienzTrsaxit'iNo ratings yet
- Smoking Cessation Nursing InterventionsDocument12 pagesSmoking Cessation Nursing Interventionsapi-741272284No ratings yet
- Cannabis For Symptom Management in Older Adults - 2020Document19 pagesCannabis For Symptom Management in Older Adults - 2020Carlos Ferrete JuniorNo ratings yet
- Vaping Smoking and Phy Fitness Young MenDocument7 pagesVaping Smoking and Phy Fitness Young MenShreeya AthavaleNo ratings yet
- 54-Article Text-539-1-10-20230301Document9 pages54-Article Text-539-1-10-20230301jovandaureliaNo ratings yet
- Summerize The F-WPS OfficemDocument4 pagesSummerize The F-WPS OfficemA HNo ratings yet
- Passed and Cleared' - Former Tobacco Smokers' Experience in Quitting SmokingDocument9 pagesPassed and Cleared' - Former Tobacco Smokers' Experience in Quitting SmokingzikriNo ratings yet
- Content ServerDocument16 pagesContent ServerJelena VidićNo ratings yet
- Factors Correlated With Smoking Cessation Success in Older Adults: A Retrospective Cohort Study in TaiwanDocument9 pagesFactors Correlated With Smoking Cessation Success in Older Adults: A Retrospective Cohort Study in TaiwanKhaziatun NurNo ratings yet
- Adolescent Inhalant Abuse Leads To Other Drug Use and Impaired Growth Implications For DiagnosisDocument6 pagesAdolescent Inhalant Abuse Leads To Other Drug Use and Impaired Growth Implications For DiagnosisAlfredo MorenoNo ratings yet
- 4-Effects of Different Combined Behavioral and Pharmacological Interventions On Smoking Cessation A Network Meta-Analysis of 103 Randomized Controlled TrialsDocument11 pages4-Effects of Different Combined Behavioral and Pharmacological Interventions On Smoking Cessation A Network Meta-Analysis of 103 Randomized Controlled Trialszhouliying684No ratings yet
- Adverse Health Effects of Chronic Cannabis Use - Hall - Drug Testing and Analysis 6 (2014)Document7 pagesAdverse Health Effects of Chronic Cannabis Use - Hall - Drug Testing and Analysis 6 (2014)dextroenantiomerNo ratings yet
- Research Paper-2Document9 pagesResearch Paper-2api-741551545No ratings yet
- HHS Public Access: Smoking Cessation and The Cardiovascular PatientDocument11 pagesHHS Public Access: Smoking Cessation and The Cardiovascular PatientNatalia CaballeroNo ratings yet
- Review Related LiteratureDocument7 pagesReview Related Literaturehannah enopiaNo ratings yet
- Factors Affecting Dropout in The Smoking Cessation Outpatient ClinicDocument7 pagesFactors Affecting Dropout in The Smoking Cessation Outpatient ClinicAmbarsari HamidahNo ratings yet
- The Effect of Smoking in Increasing Stroke Risks Among Palestinian PeopleDocument15 pagesThe Effect of Smoking in Increasing Stroke Risks Among Palestinian PeopleMahmoud IbraheemNo ratings yet
- Young Adult Sequelae of Adolescent Cannabis Use: An Integrative AnalysisDocument8 pagesYoung Adult Sequelae of Adolescent Cannabis Use: An Integrative Analysisirribarra.nlopez3046No ratings yet
- Change in TbaccoDocument6 pagesChange in Tbaccosofia ayu lestariNo ratings yet
- Combination of Varenicline and Nicotine Patch For Smoking Cessation: A Case ReportDocument3 pagesCombination of Varenicline and Nicotine Patch For Smoking Cessation: A Case Reportrbatjun576No ratings yet
- Association of Smoking and Obesity Among Residents of Zone 2 Sto. Domingo, Biňan, Laguna ON MAY 2016Document24 pagesAssociation of Smoking and Obesity Among Residents of Zone 2 Sto. Domingo, Biňan, Laguna ON MAY 2016Sherlock HolmesNo ratings yet
- Radiol 212611Document7 pagesRadiol 212611Julián DuránNo ratings yet
- Smoking InfertilityDocument8 pagesSmoking Infertilityjames.armstrong35No ratings yet
- Smoking Cessation or Reduction With Nicotine Replacement Therapy: A Placebo-Controlled Double Blind Trial With Nicotine Gum and InhalerDocument28 pagesSmoking Cessation or Reduction With Nicotine Replacement Therapy: A Placebo-Controlled Double Blind Trial With Nicotine Gum and InhalerSigit Harya HutamaNo ratings yet
- Final Thesis 1Document57 pagesFinal Thesis 1Claribel LamsisNo ratings yet
- A Pragmatic Trial of E-Cigarettes, Incentives, and Drugs For Smoking CessationDocument9 pagesA Pragmatic Trial of E-Cigarettes, Incentives, and Drugs For Smoking CessationMr. LNo ratings yet
- Cigarette Smoking Among Medical StudentsDocument3 pagesCigarette Smoking Among Medical StudentsazifattahNo ratings yet
- 1post-Class Quiz1 StudydesignsDocument14 pages1post-Class Quiz1 Studydesignssimplify8000No ratings yet
- NIH Conference: Systematic Review: Smoking Cessation Intervention Strategies For Adults and Adults in Special PopulationsDocument20 pagesNIH Conference: Systematic Review: Smoking Cessation Intervention Strategies For Adults and Adults in Special PopulationsFábio FreitasNo ratings yet
- Seeking The Light From The Smoke: A Case Study of Chain Smokers On Smoking Cessation in Mandaue City, PhilippinesDocument10 pagesSeeking The Light From The Smoke: A Case Study of Chain Smokers On Smoking Cessation in Mandaue City, PhilippinesPsychology and Education: A Multidisciplinary Journal100% (1)
- Stop Smoking Start Vaping - The Healthy Truth About VapingFrom EverandStop Smoking Start Vaping - The Healthy Truth About VapingNo ratings yet
- Thesis About Teenage Smoking in The PhilippinesDocument8 pagesThesis About Teenage Smoking in The PhilippinesKelly Lipiec100% (2)
- Exposition Text 10 Mei.Document4 pagesExposition Text 10 Mei.santi santiNo ratings yet
- Format Soal B. Inggris Kelas XiDocument5 pagesFormat Soal B. Inggris Kelas XiNonnie RahmaNo ratings yet
- Little and Falaces Dental Management of The Medically Compromised Patient 8th Edition Little Test Bank Full Chapter PDFDocument24 pagesLittle and Falaces Dental Management of The Medically Compromised Patient 8th Edition Little Test Bank Full Chapter PDFFredMurphybgzr100% (11)
- Fire Risk Assessment FormDocument20 pagesFire Risk Assessment FormAhmed Ibrahim100% (1)
- Part 1 - LEXICO-GRAMMARDocument8 pagesPart 1 - LEXICO-GRAMMARLinh LêNo ratings yet
- Booty BumpingDocument1 pageBooty BumpinglololmartianNo ratings yet
- Writing A Project Proposal-Detailed Lesson PlanDocument13 pagesWriting A Project Proposal-Detailed Lesson PlanNathalie MoraNo ratings yet
- Adoc - Pub - SMP Kelas 8 Bahasa Inggris Chapter 10latihan SoalDocument6 pagesAdoc - Pub - SMP Kelas 8 Bahasa Inggris Chapter 10latihan Soalalmaira sudiNo ratings yet
- 1st Draft Essay CompleteDocument11 pages1st Draft Essay Completeapi-549704676No ratings yet
- Unit 2 More Practice - VocabularyDocument3 pagesUnit 2 More Practice - VocabularypsvsolisNo ratings yet
- Intrebari AntreprenoriatDocument1 pageIntrebari AntreprenoriatMaria AlexandruNo ratings yet
- From Social Taboo To "Torch of Freedom": The Marketing of Cigarettes To WomenDocument6 pagesFrom Social Taboo To "Torch of Freedom": The Marketing of Cigarettes To WomenfaithnicNo ratings yet
- An Expository Essay-Secondhand SmokeDocument2 pagesAn Expository Essay-Secondhand Smokejuzroy91No ratings yet
- Dialog Asking & Giving Opinion (ANNISA FADILAH ALFIA)Document2 pagesDialog Asking & Giving Opinion (ANNISA FADILAH ALFIA)annisa fadilah alfiaNo ratings yet
- FU-Z31E: Air Purifier Operation Manual Petunjuk Pengoperasian Air PurifierDocument15 pagesFU-Z31E: Air Purifier Operation Manual Petunjuk Pengoperasian Air PurifierpempekplgNo ratings yet
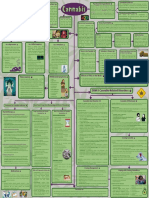
- Cannabis Concept MapDocument2 pagesCannabis Concept MapAminath Maana Ibrahim ShakeeNo ratings yet
- TTC Presentation1Document20 pagesTTC Presentation1Randy SNo ratings yet
- Soal Pts Bing 10 DKVDocument9 pagesSoal Pts Bing 10 DKVRizqi AgusnovianNo ratings yet
- Amazing Manifestation BlueprintDocument26 pagesAmazing Manifestation BlueprintDebanik Ghosh100% (5)
- Product: CatalogueDocument63 pagesProduct: CatalogueJuan PoloNo ratings yet
- English Speaking: Channel: VideoDocument18 pagesEnglish Speaking: Channel: Videofadi kimya100% (1)
- Radiation Effects of SmokingDocument5 pagesRadiation Effects of SmokingJayagokul SaravananNo ratings yet
- The Side Effects of SmokingDocument5 pagesThe Side Effects of SmokingCentral Asian StudiesNo ratings yet
- Final DemoDocument7 pagesFinal DemoJoy Santiago VeneracionNo ratings yet
- Quitnet Presentation-Csu StanislausDocument14 pagesQuitnet Presentation-Csu StanislausMaria Carmela CabalquintoNo ratings yet
- Economics Unit 5 - 1457145468349Document5 pagesEconomics Unit 5 - 1457145468349VaanazhaganNo ratings yet