Download as pdf or txt
You might also like
- B-Medium Opening ActivatorDocument31 pagesB-Medium Opening ActivatorAbiha Ali100% (1)
- COVID-19 Disease SeverityDocument7 pagesCOVID-19 Disease SeverityParishan SaeedNo ratings yet
- Practical Considerations and Management of Multi-Organ Failure of in Pre-ICU SettingDocument24 pagesPractical Considerations and Management of Multi-Organ Failure of in Pre-ICU SettingyusNo ratings yet
- Respiratory Failure (ACUTE) : Dora M Alvarez MD LH 2004Document72 pagesRespiratory Failure (ACUTE) : Dora M Alvarez MD LH 2004Lovely San SebastianNo ratings yet
- COVID-19 Management of Critical Care Cases PDFDocument6 pagesCOVID-19 Management of Critical Care Cases PDFLubna AliNo ratings yet
- Screening For COVID-19Document11 pagesScreening For COVID-19ruhulcoc1No ratings yet
- 14.guidelines AsthmaDocument4 pages14.guidelines AsthmaRed DevilNo ratings yet
- Respiratory Management Pada KegawatanDocument31 pagesRespiratory Management Pada KegawatanM.Arif FananiNo ratings yet
- Covid19 - Pathophysiology and ManagementDocument51 pagesCovid19 - Pathophysiology and ManagementMyraflor CaroNo ratings yet
- Covid For ClerksDocument60 pagesCovid For ClerksNehemiah FranciscoNo ratings yet
- Guidelines Treatment Protocol April 2021 MergedDocument78 pagesGuidelines Treatment Protocol April 2021 Mergedjose j kochuparambilNo ratings yet
- COVID-19 Disease Severity: - Mild Disease: - Moderate Disease:pneumoniaDocument2 pagesCOVID-19 Disease Severity: - Mild Disease: - Moderate Disease:pneumoniaSam Raven AndresNo ratings yet
- Pneumonia: Tim Teaching Farmakoterapi Penyakit Infeksi Dan Keganasan Fakultas Farmasi Universitas Jember Gasal 20211Document67 pagesPneumonia: Tim Teaching Farmakoterapi Penyakit Infeksi Dan Keganasan Fakultas Farmasi Universitas Jember Gasal 20211Evie WulansariNo ratings yet
- Oxygen Therapy PDFDocument36 pagesOxygen Therapy PDFStefanus LimNo ratings yet
- Coronavirus19 1Document60 pagesCoronavirus19 1bekbekk cabahugNo ratings yet
- Eathing IDI 2015Document58 pagesEathing IDI 2015Syamsul Bahri AkhasNo ratings yet
- CG VM Management of ARDSDocument31 pagesCG VM Management of ARDSVishnu ManglaNo ratings yet
- Covid-19 Protocol Severity and ManagementDocument4 pagesCovid-19 Protocol Severity and ManagementMardy DeponaNo ratings yet
- Covid-19 Physiotherapy ManagementDocument69 pagesCovid-19 Physiotherapy ManagementMaulidya Deasy KurniasiNo ratings yet
- Silent Hypoxia TriageDocument4 pagesSilent Hypoxia TriageKNGNo ratings yet
- ABG, Diffusion CapacityDocument32 pagesABG, Diffusion CapacitySujan ThapaNo ratings yet
- CopdDocument16 pagesCopdHot MathNo ratings yet
- Assessment Pada Covid-19Document60 pagesAssessment Pada Covid-19FISIOTERAPI TRIMITRANo ratings yet
- Niall Cosgrave Email: Ncosgrav@Tcd - IeDocument24 pagesNiall Cosgrave Email: Ncosgrav@Tcd - IeSaoirse MorrinNo ratings yet
- Copd NatsDocument47 pagesCopd NatsKristen Nathany MalapitNo ratings yet
- Early Assessment of Respiratory DistressDocument17 pagesEarly Assessment of Respiratory DistressRosi AmaliaNo ratings yet
- ARDS Case PresentationDocument80 pagesARDS Case Presentationsupladitasha_750% (3)
- 006 COPD - Lecture StudentsDocument52 pages006 COPD - Lecture Studentszyz6639No ratings yet
- Acute Respiratory Failure: Recognition and Early InterventionDocument31 pagesAcute Respiratory Failure: Recognition and Early InterventionChristian JaraNo ratings yet
- PneumoniaDocument69 pagesPneumoniaHamna ZainabNo ratings yet
- COPD Ready To Paste FormatDocument4 pagesCOPD Ready To Paste FormatGiselle EstoquiaNo ratings yet
- Physiotherapy Managment For CoviedDocument110 pagesPhysiotherapy Managment For CoviedRuba DahlanNo ratings yet
- Approach To A Hypoxic Patient in IcuDocument64 pagesApproach To A Hypoxic Patient in IcusanjibNo ratings yet
- Covid 2021Document48 pagesCovid 2021Diego SarmientoNo ratings yet
- Acure Resp Failure and ARDS 1-13-2020Document37 pagesAcure Resp Failure and ARDS 1-13-2020slatcheshotmail.comNo ratings yet
- RHC in PH FinalDocument36 pagesRHC in PH FinalKirti KadianNo ratings yet
- ABG InterpretationDocument49 pagesABG InterpretationMuhammad Fathullah MazparNo ratings yet
- Oxygen Therapy-2Document18 pagesOxygen Therapy-2fildzah fitriyaniNo ratings yet
- Chronic Obstructive Pulmonary Disease, MMRC Grade 1: Primary ImpressionDocument5 pagesChronic Obstructive Pulmonary Disease, MMRC Grade 1: Primary ImpressionJayson Joseph AngloNo ratings yet
- Hypercapnia During Acute Respiratory Distress SyndromeDocument6 pagesHypercapnia During Acute Respiratory Distress SyndromeJZHZL QNo ratings yet
- Bronsiolita, WH Rec, 3Document56 pagesBronsiolita, WH Rec, 3Marian Balan100% (1)
- Critical CareDocument44 pagesCritical Caremohamedsharkawwy82No ratings yet
- Covid-19 Physiotherapy ManagementDocument60 pagesCovid-19 Physiotherapy ManagementMartiasariiiNo ratings yet
- Basic Arterial Blood Gas (Abg) Interpretation: By: Jesus Mario A Lopez JR., R.T.,R.NDocument36 pagesBasic Arterial Blood Gas (Abg) Interpretation: By: Jesus Mario A Lopez JR., R.T.,R.NJesus Mario LopezNo ratings yet
- Hypotension and Respiratory DistressDocument15 pagesHypotension and Respiratory DistressEmily EresumaNo ratings yet
- Pulmo EmergencyDocument172 pagesPulmo EmergencypanvilaiNo ratings yet
- REV MRJagaTengah - MEDCON - ANI - hyperbilirubinemia+transaminitis+AKIDocument22 pagesREV MRJagaTengah - MEDCON - ANI - hyperbilirubinemia+transaminitis+AKILilik AndayatiNo ratings yet
- Pneumonia: Andrian Dwi Rizki Setyawan 30101306872Document25 pagesPneumonia: Andrian Dwi Rizki Setyawan 30101306872Dayu MandhaNo ratings yet
- Acute Chest SyndromeDocument28 pagesAcute Chest SyndromeJohn OkidiNo ratings yet
- 6.pneumonia (New)Document104 pages6.pneumonia (New)Ryana Fitriana IINo ratings yet
- Guidelines On Management of Covid-19 Icu PatientDocument32 pagesGuidelines On Management of Covid-19 Icu PatientBrainy LumineusNo ratings yet
- Cap No GraphyDocument37 pagesCap No GraphyLeypotNo ratings yet
- Just A Pneumonia!Document37 pagesJust A Pneumonia!Afiqslim MohdNo ratings yet
- Week 1Document13 pagesWeek 1KalistaArdeliaNo ratings yet
- Respiratory (Medicalstudyzone - Com)Document72 pagesRespiratory (Medicalstudyzone - Com)shahroozabbas66No ratings yet
- Test 1Document13 pagesTest 1Kat IvyNo ratings yet
- 02 Bolnavul Dispneic 2015Document69 pages02 Bolnavul Dispneic 2015Madalina BulboacaNo ratings yet
- Adult Respiratory Distress Syndrome: Mazen Kherallah, MD, FCCPDocument51 pagesAdult Respiratory Distress Syndrome: Mazen Kherallah, MD, FCCPArsitoNo ratings yet
- Soba-Clinical Practice GuideDocument19 pagesSoba-Clinical Practice GuideScribdTranslationsNo ratings yet
- Copd VS AsthmaDocument2 pagesCopd VS AsthmaHarkirat AtwalNo ratings yet
- Important Instructions For Online Admission 2020-21: NSCBM Govt. College Hamirpur District Hamirpur, Himachal PradeshDocument5 pagesImportant Instructions For Online Admission 2020-21: NSCBM Govt. College Hamirpur District Hamirpur, Himachal PradeshabhishekNo ratings yet
- 1.1 Introduction - NotesDocument12 pages1.1 Introduction - NotesabhishekNo ratings yet
- Automatic MotorBike Stand Slider 2020Document16 pagesAutomatic MotorBike Stand Slider 2020abhishek100% (2)
- Abhishek Chandel: Key CompetenciesDocument2 pagesAbhishek Chandel: Key CompetenciesabhishekNo ratings yet
- Tangent (Geometry) : Tangent To A Curve. The Red Line Is Tangential To The Curve at The Point Marked by A Red DotDocument41 pagesTangent (Geometry) : Tangent To A Curve. The Red Line Is Tangential To The Curve at The Point Marked by A Red DotabhishekNo ratings yet
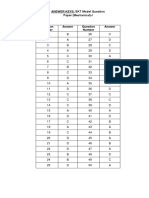
- Answer Keys: EKT Model Question Paper (Mechanical) - IDocument6 pagesAnswer Keys: EKT Model Question Paper (Mechanical) - IabhishekNo ratings yet
- Application of Differential EquationDocument42 pagesApplication of Differential EquationabhishekNo ratings yet
- Application of Partial Derivative (NIDHI)Document13 pagesApplication of Partial Derivative (NIDHI)abhishekNo ratings yet
- Application of Differential EquationDocument42 pagesApplication of Differential EquationabhishekNo ratings yet
- Process To Apply Student LeaveDocument3 pagesProcess To Apply Student LeaveabhishekNo ratings yet
- Revised Monthly Reporting Format - HWCDocument8 pagesRevised Monthly Reporting Format - HWCChanmari West Sub-Centre50% (2)
- 15) Refractory Open-Angle Glaucoma After Neodymium - Yttrium-Aluminum-Garnet Laser Lysis of Vitreous FloatersDocument6 pages15) Refractory Open-Angle Glaucoma After Neodymium - Yttrium-Aluminum-Garnet Laser Lysis of Vitreous FloatershasdiniNo ratings yet
- HALLOCINOGENDocument43 pagesHALLOCINOGENChinnu ChinnuNo ratings yet
- 03 NCP 1 Viral HepatitisDocument17 pages03 NCP 1 Viral Hepatitisamit100% (2)
- Incident Investigation and Corrective ActionDocument56 pagesIncident Investigation and Corrective ActionBryant YowNo ratings yet
- ADA EASD Consensus 2012Document16 pagesADA EASD Consensus 2012Beta Cells in DiabetesNo ratings yet
- The Reality of Monkeypox in UtahDocument4 pagesThe Reality of Monkeypox in UtahJaxon FlorenceNo ratings yet
- VPTH 121 1ST Lec ExamDocument1 pageVPTH 121 1ST Lec ExamSzarina KoNo ratings yet
- Exercise 1. Complete The Text Using The Words From The BoxDocument5 pagesExercise 1. Complete The Text Using The Words From The BoxВлада ВоеводинаNo ratings yet
- RESPIFLODocument32 pagesRESPIFLOrissaNo ratings yet
- Psych Narrative Report (1) LoissDocument21 pagesPsych Narrative Report (1) LoissBea Aldueza100% (1)
- Nutrition Care Process Note-IcuDocument2 pagesNutrition Care Process Note-Icuapi-1032325430% (1)
- MS - Tile InstallationDocument14 pagesMS - Tile InstallationabedNo ratings yet
- General Education ReviewerDocument15 pagesGeneral Education ReviewerMat Seigfried SaguiboNo ratings yet
- Test Questions GRADE 9 NAIL CAREDocument2 pagesTest Questions GRADE 9 NAIL CARESharmaine ManigosNo ratings yet
- Icesu Updates Covid19 Confirmed Cases: Morbidity Week 13 January 1 - April 2, 2022Document15 pagesIcesu Updates Covid19 Confirmed Cases: Morbidity Week 13 January 1 - April 2, 2022Jeremae VentarNo ratings yet
- Drug Induced Movement DisordersDocument65 pagesDrug Induced Movement DisordersShaunak Patil100% (1)
- Hepatic Embolotherapy in Interventional Oncology - Technology, Techniques, and ApplicationsDocument15 pagesHepatic Embolotherapy in Interventional Oncology - Technology, Techniques, and ApplicationsVeronica AlexanderNo ratings yet
- Psychophysiological Methods in NeuroscienceDocument17 pagesPsychophysiological Methods in NeuroscienceKariela EstherNo ratings yet
- Ex - Cerebellar ExamDocument2 pagesEx - Cerebellar ExamssNo ratings yet
- PIIS2589537023000172Document12 pagesPIIS2589537023000172Gerry FonziNo ratings yet
- Quarter 3 Health 10Document34 pagesQuarter 3 Health 10Arvin SeraniasNo ratings yet
- Nursing Clinical QuestionsDocument8 pagesNursing Clinical QuestionsMrinalini BakshiNo ratings yet
- The Panama Aging Research Initiative Longitudinal Study: Lessons From The FieldDocument5 pagesThe Panama Aging Research Initiative Longitudinal Study: Lessons From The FieldMiguel Ángel DominguezNo ratings yet
- Bakteriološki Nalaz U Uretri Muškaraca Sa I Bez Negonoroičnog UretritisaDocument4 pagesBakteriološki Nalaz U Uretri Muškaraca Sa I Bez Negonoroičnog UretritisaNemanjaDragosavacNo ratings yet
- Amity UniversityDocument7 pagesAmity UniversityAryan ShantamNo ratings yet
- Exam 5 TermsDocument2 pagesExam 5 Termsapi-315572926No ratings yet
- 840 B2 Fire Rated Pu FoamDocument10 pages840 B2 Fire Rated Pu FoamJonathan Alexis Abarzua TorresNo ratings yet
- SHOULD OBESITY BE LABELLED AS A DISEASE-editedDocument9 pagesSHOULD OBESITY BE LABELLED AS A DISEASE-editedthirumal rNo ratings yet