Download as docx, pdf, or txt
You might also like
- NCLEX-RN Cheat Sheet (Claudia Goncalves)Document14 pagesNCLEX-RN Cheat Sheet (Claudia Goncalves)Rovie Gonzales Dimas100% (38)
- American Board of Family Medicine: 2020 Questions & AnswersDocument112 pagesAmerican Board of Family Medicine: 2020 Questions & AnswersthanaaNo ratings yet
- Neonatal Parenteral and Enteral NutritionDocument23 pagesNeonatal Parenteral and Enteral NutritionPrimadiati Nickyta Sari100% (1)
- Identifying VariablesDocument4 pagesIdentifying VariablesAllan CastroNo ratings yet
- Identifying VariablesDocument4 pagesIdentifying VariablesAllan CastroNo ratings yet
- McCormick 2012 Ch2 Understanding Relating - CHANGEDocument10 pagesMcCormick 2012 Ch2 Understanding Relating - CHANGEDiana ElenaNo ratings yet
- Uncovery - A New Understanding B - Amanda JonesDocument133 pagesUncovery - A New Understanding B - Amanda JonesMaicon Thiago100% (1)
- Seronegative Myasthenia Gravis Presenting With PneumoniaDocument4 pagesSeronegative Myasthenia Gravis Presenting With PneumoniaJ. Ruben HermannNo ratings yet
- Paravertebral AbscessDocument3 pagesParavertebral AbscessAlam MartadipuraNo ratings yet
- 17Document19 pages17Francisco Javier Ortega Guillem0% (1)
- Question of The Week # 433: Archer Red 11:25 AM Links To This PostDocument34 pagesQuestion of The Week # 433: Archer Red 11:25 AM Links To This PostChristian JaraNo ratings yet
- Treatment of Gynecomastia With Prednisone Case RepDocument8 pagesTreatment of Gynecomastia With Prednisone Case RepGonzalo Sanchez DiazNo ratings yet
- Attending Osteomyelitis ModuleDocument9 pagesAttending Osteomyelitis ModuleMrLarry DolorNo ratings yet
- Jurnal AE 2Document3 pagesJurnal AE 2Mira Mariana UlfahNo ratings yet
- Patient Case Presentation IIDocument7 pagesPatient Case Presentation IILangat IsaacNo ratings yet
- Letters To The Editors: Primary Sjögren's Syndrome As Paraneoplastic Disorder: A Case ReportDocument1 pageLetters To The Editors: Primary Sjögren's Syndrome As Paraneoplastic Disorder: A Case ReportDarian AngNo ratings yet
- Medicine: Systemic Lupus Erythematosus With Guillian - Barre SyndromeDocument5 pagesMedicine: Systemic Lupus Erythematosus With Guillian - Barre SyndromeShri RamNo ratings yet
- BPJ Vol 10 No 3 P 1369-1377Document9 pagesBPJ Vol 10 No 3 P 1369-1377citra annisa fitriNo ratings yet
- Case 34-2008 - BrucellaDocument43 pagesCase 34-2008 - Brucellapalak32No ratings yet
- Artigo Denagem LinfáticaDocument3 pagesArtigo Denagem LinfáticaLeonardo MelloNo ratings yet
- Group 2 Case ScenarioDocument6 pagesGroup 2 Case ScenarioNur SanaaniNo ratings yet
- MBChB4 5PastPapersDocument172 pagesMBChB4 5PastPapersHariharan NarendranNo ratings yet
- Hypomagnesemia and Prolonged Hospital Stay: A Case Report and Literature ReviewDocument6 pagesHypomagnesemia and Prolonged Hospital Stay: A Case Report and Literature ReviewIJAR JOURNALNo ratings yet
- MYASTHENIA GRAVIS Case PresentationDocument78 pagesMYASTHENIA GRAVIS Case PresentationRho Vince Caño Malagueño50% (4)
- The Challenge of Diagnosing Psoas Abscess: Case ReportDocument4 pagesThe Challenge of Diagnosing Psoas Abscess: Case ReportNataliaMaedyNo ratings yet
- Brmedj03163 0034Document4 pagesBrmedj03163 0034stevenburrow06No ratings yet
- Klair 2014Document3 pagesKlair 2014PabloIgLopezNo ratings yet
- Clinical CaseDocument10 pagesClinical CaseCristy RomeroNo ratings yet
- PBL 10Document4 pagesPBL 10lliioNo ratings yet
- Shortal2019 PDFDocument13 pagesShortal2019 PDFdr_imronrosyadiNo ratings yet
- New Onset Autoimmune Disease or Macrophage Activation SyndromeDocument5 pagesNew Onset Autoimmune Disease or Macrophage Activation SyndromePyaePhyoAungNo ratings yet
- Recuero 2014Document1 pageRecuero 20142dradhtiphonephotosbackupNo ratings yet
- Atypical Presentation Acute AppendicitisDocument5 pagesAtypical Presentation Acute AppendicitisE. Tito Julianda SinagaNo ratings yet
- Case Study of Benign Hand TremorsDocument7 pagesCase Study of Benign Hand TremorsLupa Ingatan100% (1)
- Chest Pain - Part 1 - Initial Presentation & InvestigationsDocument4 pagesChest Pain - Part 1 - Initial Presentation & InvestigationsThorgan HazardNo ratings yet
- ExperimentalDocument10 pagesExperimentalKelly Díaz RiveraNo ratings yet
- 1986 - Traditional Chinese Acupuncture A Potentially Useful Antiemetic - Dundee Et Al.Document2 pages1986 - Traditional Chinese Acupuncture A Potentially Useful Antiemetic - Dundee Et Al.A CNo ratings yet
- Case ReportDocument12 pagesCase Reportmohammad khinagirNo ratings yet
- A Crazy Cause of DyspneaDocument6 pagesA Crazy Cause of DyspneaAbdur Rachman Ba'abdullahNo ratings yet
- A Pain in The Butt - A Case Series of Gluteal Compartment Syndrome - PMCDocument6 pagesA Pain in The Butt - A Case Series of Gluteal Compartment Syndrome - PMCchhabraanNo ratings yet
- Prescription WritingDocument2 pagesPrescription Writingkinda goodNo ratings yet
- Update On Prostatitis and TreatmentsDocument37 pagesUpdate On Prostatitis and TreatmentsAlbert Palomino RaymeNo ratings yet
- Siegler 1988Document4 pagesSiegler 19882024046No ratings yet
- Ondan Hipo 3Document5 pagesOndan Hipo 3putri maharani andesNo ratings yet
- Lumbar Radiculopathy RuDocument29 pagesLumbar Radiculopathy RuMark MarivelesNo ratings yet
- Emergency Medicine EducationGuillain-Barré Syndrome - Third Time's The Charm - EmDOCs - Net - Emergency Medicine EducationDocument14 pagesEmergency Medicine EducationGuillain-Barré Syndrome - Third Time's The Charm - EmDOCs - Net - Emergency Medicine EducationPgmee KimsNo ratings yet
- April2005 EditorialDocument3 pagesApril2005 EditorialJonathan Alexis Salinas UlloaNo ratings yet
- Guillain-Barre Syndrome Presenting With Sensory Disturbance Following A Herpes Virus Infection: A Case ReportDocument5 pagesGuillain-Barre Syndrome Presenting With Sensory Disturbance Following A Herpes Virus Infection: A Case ReportAsep MetrikaNo ratings yet
- IDC203 Bioethics Case 2Document4 pagesIDC203 Bioethics Case 2ggasg_9No ratings yet
- Systemic Lupus ErythematosusDocument6 pagesSystemic Lupus Erythematosusapi-3743565No ratings yet
- Mga Case Study Na Dili Ko SureDocument5 pagesMga Case Study Na Dili Ko SureReem MahmoudNo ratings yet
- 03TES2011Document999 pages03TES2011Ahmad IsmatullahNo ratings yet
- Association of Myasthenia Gravis and Behçet's Disease: A CaseDocument4 pagesAssociation of Myasthenia Gravis and Behçet's Disease: A CaseTrần Văn ĐệNo ratings yet
- Byol Meridians Body MeridiansDocument70 pagesByol Meridians Body Meridianspbi tv100% (2)
- Im - RheumatologyDocument3 pagesIm - Rheumatologysnapb202No ratings yet
- HshsjneDocument5 pagesHshsjneyunia habsariNo ratings yet
- Case ReportDocument11 pagesCase ReportJenna LysiaNo ratings yet
- Clinical Challenge SeriesDocument28 pagesClinical Challenge SeriesayugitaNo ratings yet
- Poliadenitis NodosaDocument5 pagesPoliadenitis NodosaRicardo Uzcategui ArreguiNo ratings yet
- Comparison Between Epleys Maneuvre and Prochlorperazine Maleate in Treatment of Benign Paroxysmal Positional VertigoDocument5 pagesComparison Between Epleys Maneuvre and Prochlorperazine Maleate in Treatment of Benign Paroxysmal Positional VertigoFila DelviaNo ratings yet
- MKSAP13 RheumatologyDocument67 pagesMKSAP13 RheumatologyMuneer Ahmad100% (1)
- Thornton 2016Document5 pagesThornton 2016AfdhalRuslanNo ratings yet
- Case of Celiac's Disease Mimicking ALSDocument4 pagesCase of Celiac's Disease Mimicking ALSfakbikNo ratings yet
- Subjects of International LawDocument16 pagesSubjects of International LawAllan CastroNo ratings yet
- Castro, Allan B. (Assignment 1 - PIL)Document53 pagesCastro, Allan B. (Assignment 1 - PIL)Allan CastroNo ratings yet
- Castro, Allan B. (Assignment 2 - Torts)Document77 pagesCastro, Allan B. (Assignment 2 - Torts)Allan CastroNo ratings yet
- Castro, Allan B. (Assignment 3 - Credit Transactions)Document31 pagesCastro, Allan B. (Assignment 3 - Credit Transactions)Allan CastroNo ratings yet
- General Principles in Public International LawDocument15 pagesGeneral Principles in Public International LawAllan CastroNo ratings yet
- Petition: SPEC. PRO. CASE No.Document6 pagesPetition: SPEC. PRO. CASE No.Allan CastroNo ratings yet
- 1 NebresHemorrhagic StrokeDocument5 pages1 NebresHemorrhagic StrokeAllan CastroNo ratings yet
- 8 Ramirez Spinal Cord TraumaDocument6 pages8 Ramirez Spinal Cord TraumaAllan CastroNo ratings yet
- Flail Chest Part I: Case Report Review A) Patient InformationDocument5 pagesFlail Chest Part I: Case Report Review A) Patient InformationAllan Castro100% (1)
- Traumatic Brain Injury A Case Report: SCORE:40/50Document10 pagesTraumatic Brain Injury A Case Report: SCORE:40/50Allan CastroNo ratings yet
- 2 Diclihon Ischemic StrokeDocument5 pages2 Diclihon Ischemic StrokeAllan CastroNo ratings yet
- 5 Malado Guillain Barre SyndromeDocument7 pages5 Malado Guillain Barre SyndromeAllan CastroNo ratings yet
- Amyotrophic Lateral Sclerosis A.: Excellent History But Was This Copy-Pasted?Document8 pagesAmyotrophic Lateral Sclerosis A.: Excellent History But Was This Copy-Pasted?Allan CastroNo ratings yet
- Patient: Multiple Sclerosis Part I: Case Report Review A) Patient InformationDocument7 pagesPatient: Multiple Sclerosis Part I: Case Report Review A) Patient InformationAllan CastroNo ratings yet
- Exploring Major Predictors of Student Satisfaction: An Input Towards A Learning-Friendly School EnvironmentDocument24 pagesExploring Major Predictors of Student Satisfaction: An Input Towards A Learning-Friendly School EnvironmentAllan CastroNo ratings yet
- SLU Accountancy Boards AnalysisDocument7 pagesSLU Accountancy Boards AnalysisAllan CastroNo ratings yet
- Far Infrared Med FactsDocument3 pagesFar Infrared Med FactsBeni Setiawan100% (2)
- Joint MobilizationDocument35 pagesJoint Mobilizationkiran patil75% (4)
- Farah Al Souheil, Pharmd, RPH Lebanese International University, SopDocument36 pagesFarah Al Souheil, Pharmd, RPH Lebanese International University, Sopعلي عويد جابر محمدNo ratings yet
- A Critical Review of Interventions Targeting ProsodyDocument7 pagesA Critical Review of Interventions Targeting ProsodyDigilindaNo ratings yet
- Internet Case For Supplement 7Document3 pagesInternet Case For Supplement 7johnmia20No ratings yet
- Tumours of The Central Nervous System: FM Brett MD., FrcpathDocument57 pagesTumours of The Central Nervous System: FM Brett MD., FrcpathDrGasnasNo ratings yet
- UrticaDocument9 pagesUrticaSundara Veerraju100% (1)
- HYPERALDOSTERONISMDocument7 pagesHYPERALDOSTERONISMMarnee Justine ColladoNo ratings yet
- MHS ProjectDocument3 pagesMHS ProjectcbjdcbsjdNo ratings yet
- 9 Hip MobilizationDocument12 pages9 Hip MobilizationGautamNo ratings yet
- Chapter 3 - Legal IssuesDocument6 pagesChapter 3 - Legal IssuesKTNo ratings yet
- Multiple Microneedling Sessions For Minimally Invasive FacialDocument9 pagesMultiple Microneedling Sessions For Minimally Invasive FacialludyNo ratings yet
- Guia Biomedica Completa OkDocument11 pagesGuia Biomedica Completa OkpaolaNo ratings yet
- Hygiene and Sanitary Practices in The Fruit JuiceDocument19 pagesHygiene and Sanitary Practices in The Fruit JuiceJoyce Marian BelonguelNo ratings yet
- Depersonalization DisorderDocument12 pagesDepersonalization Disorderapi-12656630No ratings yet
- Liquid Coming Out of Butt After DrinkingDocument1 pageLiquid Coming Out of Butt After DrinkingKrystal IsomNo ratings yet
- Bulimia Nervosa JDocument10 pagesBulimia Nervosa JnessaNo ratings yet
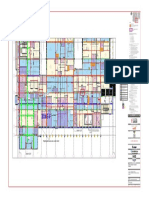
- OR4100-1-ATNM-AB4-SDW-00001-4A - Level-00-ZONE FDocument1 pageOR4100-1-ATNM-AB4-SDW-00001-4A - Level-00-ZONE FAhmed SolankiNo ratings yet
- Session 6Document6 pagesSession 6Sistine Rose LabajoNo ratings yet
- The Ocular Surface: Sarah E. Kenny, Cooper B. Tye, Daniel A. Johnson, Ahmad Kheirkhah TDocument7 pagesThe Ocular Surface: Sarah E. Kenny, Cooper B. Tye, Daniel A. Johnson, Ahmad Kheirkhah TSaaraAlleyahAlAnaziNo ratings yet
- To Adjust or Not Adjust Nonparametric Effect Sizes, Confidence Intervals, and Real-World Meaning PDFDocument7 pagesTo Adjust or Not Adjust Nonparametric Effect Sizes, Confidence Intervals, and Real-World Meaning PDFTodd MartinezNo ratings yet
- AHA Hypertension Guidelines 2017Document22 pagesAHA Hypertension Guidelines 2017Anonymous elSqPhzKNo ratings yet
- Diabetes ... : Primary Prevention: Primary PreventionDocument3 pagesDiabetes ... : Primary Prevention: Primary PreventionsajithrkNo ratings yet
- Thoracic SurgeryDocument33 pagesThoracic SurgeryChino Estoque FragataNo ratings yet
- Movement Disorders 4335Document28 pagesMovement Disorders 4335Fitri Amelia RizkiNo ratings yet
- Icrp 117Document102 pagesIcrp 117Sari BustillosNo ratings yet