Download as docx, pdf, or txt
You might also like
- That Time I Got Reincarnated As A Slime, Vol. 15Document468 pagesThat Time I Got Reincarnated As A Slime, Vol. 15Phil50% (2)
- Nursing Care Plan - Impaired Gas ExchangeDocument3 pagesNursing Care Plan - Impaired Gas ExchangeYum C86% (65)
- Executive Coaching Workbook PDFDocument19 pagesExecutive Coaching Workbook PDFDiego Fortes100% (4)
- Wpa PaperDocument12 pagesWpa Paperkhairul ezwan100% (1)
- 6 Pleural Effusion Nursing Care PlansDocument7 pages6 Pleural Effusion Nursing Care PlansShaina Fe RabaneraNo ratings yet
- Impaired Gas ExchangeDocument3 pagesImpaired Gas ExchangeBenedicto RosalNo ratings yet
- Asthma Case StudyDocument4 pagesAsthma Case StudyEver Green100% (2)
- Global Reporting System User Manual GRS-Rig V4.0: TitleDocument161 pagesGlobal Reporting System User Manual GRS-Rig V4.0: Titlevikrant911No ratings yet
- EmphysemaDocument27 pagesEmphysemaDiana Laura LeiNo ratings yet
- AssesmentDocument9 pagesAssesmentmizrypNo ratings yet
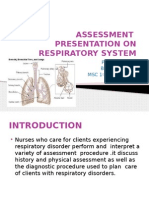
- On Respiratory AssessmentDocument38 pagesOn Respiratory AssessmentBhagyashri GaikwadNo ratings yet
- NCPDocument9 pagesNCPEjie Boy Isaga67% (3)
- Nursing Care PlanDocument14 pagesNursing Care PlanVin Landicho100% (1)
- Notes On RespiratoryDocument14 pagesNotes On RespiratorySuchitaNo ratings yet
- Emphysema Case Study AnalysisDocument10 pagesEmphysema Case Study AnalysisEfren VisteNo ratings yet
- Assessment of The Respiratory SystemDocument10 pagesAssessment of The Respiratory SystemKhanh LeNo ratings yet
- Case Study Nursing Diagnosis of PneumothoraxDocument8 pagesCase Study Nursing Diagnosis of PneumothoraxJansen Arquilita RiveraNo ratings yet
- Case Study Asthma Group 2Document17 pagesCase Study Asthma Group 2Kennedy PelicoNo ratings yet
- Nursing Care Plans of Bronchial AsthmaDocument8 pagesNursing Care Plans of Bronchial AsthmaKannanNo ratings yet
- Nursing DiagnosisDocument4 pagesNursing DiagnosisKrizzia CarlosNo ratings yet
- Chap 26 To 38 Case Study Answers To QuestionsDocument13 pagesChap 26 To 38 Case Study Answers To QuestionsElaine Jean UayanNo ratings yet
- Lesson 3 Responses To Altered Ventilatory FunctionDocument136 pagesLesson 3 Responses To Altered Ventilatory FunctionMonasque PamelaNo ratings yet
- CopdDocument47 pagesCopdNingshesil Ny HermantNo ratings yet
- Diagnostic Studies: The Forced Expiratory Volume Over 1 Second (FEVDocument7 pagesDiagnostic Studies: The Forced Expiratory Volume Over 1 Second (FEVKushan SenanayakaNo ratings yet
- Case Analysis Bronchial AsthmaDocument21 pagesCase Analysis Bronchial AsthmaKim LladaNo ratings yet
- Shortness of Breath Nursing Diagnosis and Nursing Care PlansDocument13 pagesShortness of Breath Nursing Diagnosis and Nursing Care PlansRuffy AbdulazisNo ratings yet
- Key Notes Adapted From Smeltzer Medical Surgical Nursing 11 EditionDocument5 pagesKey Notes Adapted From Smeltzer Medical Surgical Nursing 11 EditionKarla LopezNo ratings yet
- System Careplans - Integummentary SystemDocument39 pagesSystem Careplans - Integummentary SystemNicole DouglasNo ratings yet
- Ineffective Airway Clearance R/T Tracheobronchial ObstructionDocument23 pagesIneffective Airway Clearance R/T Tracheobronchial ObstructionGuia Rose SibayanNo ratings yet
- MedSurg Ch30-31Document8 pagesMedSurg Ch30-31Vanessa Da Cruz100% (1)
- Nursing Care PlanDocument22 pagesNursing Care PlanjamNo ratings yet
- Copd CaseDocument36 pagesCopd Casejho_No ratings yet
- ARDSDocument18 pagesARDSChurrizo IslamiNo ratings yet
- School of Nursing and Allied Medical Sciences: Holy Angel UniversityDocument19 pagesSchool of Nursing and Allied Medical Sciences: Holy Angel UniversityMonica BorjaNo ratings yet
- COPD Acute Management ABCDEDocument11 pagesCOPD Acute Management ABCDESS100% (1)
- Study Guide Example PDFDocument18 pagesStudy Guide Example PDFmrmr92No ratings yet
- Bronchial Obstruction: Presenter Andrea Fagan 3 Year Student NurseDocument27 pagesBronchial Obstruction: Presenter Andrea Fagan 3 Year Student NurseAndrea FaganNo ratings yet
- CHD AsthmaDocument20 pagesCHD AsthmaRj MagpayoNo ratings yet
- PneumoniaDocument17 pagesPneumoniajustin_saneNo ratings yet
- NCP For COPD and Acute PainDocument7 pagesNCP For COPD and Acute PainLenny SucalditoNo ratings yet
- Below Are 8 Pneumonia Nursing Care Plans (NCP)Document16 pagesBelow Are 8 Pneumonia Nursing Care Plans (NCP)Diana CarinoNo ratings yet
- Tolleno (Pneumonia ER)Document4 pagesTolleno (Pneumonia ER)Hannah TollenoNo ratings yet
- Week 4 - Ms1 Course Task - Cu 4 - RoveroDocument2 pagesWeek 4 - Ms1 Course Task - Cu 4 - RoveroJohnmarkLorenzanaRoveroNo ratings yet
- Group 1 Case Study Chapter 24Document10 pagesGroup 1 Case Study Chapter 24Doneva Lyn MedinaNo ratings yet
- Oxy Act 2Document5 pagesOxy Act 2Joshua DauzNo ratings yet
- Pleural Effusion EssayDocument2 pagesPleural Effusion EssayAnjae GariandoNo ratings yet
- A Case Study of Bronchial Asthma in Acute Exacerbation (Baiae)Document10 pagesA Case Study of Bronchial Asthma in Acute Exacerbation (Baiae)Janina RojoNo ratings yet
- Nursing Diagnosis For AsthmaDocument6 pagesNursing Diagnosis For AsthmaTINAIDA33% (3)
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument4 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationTrisha SuazoNo ratings yet
- Asthma 1. DefinitionDocument11 pagesAsthma 1. DefinitionKarl RobleNo ratings yet
- Worksheet#4-Oxygenation Answer The Guide Questions BelowDocument4 pagesWorksheet#4-Oxygenation Answer The Guide Questions BelowCj MayoyoNo ratings yet
- COPD FixDocument47 pagesCOPD FixerniNo ratings yet
- Upper Respiratory DisordersDocument37 pagesUpper Respiratory DisordersClaire Maurice JuaneroNo ratings yet
- Respiratory RateDocument3 pagesRespiratory RateDwight YmsonNo ratings yet
- GRPB CaseStudyASthmaDocument3 pagesGRPB CaseStudyASthmaCherry Ann BalagotNo ratings yet
- EmphysemaDocument44 pagesEmphysematheonlinegeekhubNo ratings yet
- Nursing DiagnosisDocument16 pagesNursing DiagnosisSi Bunga JonquilleNo ratings yet
- Respiratory RateDocument15 pagesRespiratory RatekierchyNo ratings yet
- NCP ErDocument3 pagesNCP ErPensayo, Stephanie Keith V.No ratings yet
- What Is COPD? Chronic Obstructive Pulmonary Disease (COPD) : Signs and SymptomsDocument11 pagesWhat Is COPD? Chronic Obstructive Pulmonary Disease (COPD) : Signs and SymptomsCecil Bhang-i Cacay - PabloNo ratings yet
- The Complete Asthma Guide: An Asthma book for adults and children, that teaches how to be asthma free naturally with the right therapeutic diets, medications & alternative herbal therapiesFrom EverandThe Complete Asthma Guide: An Asthma book for adults and children, that teaches how to be asthma free naturally with the right therapeutic diets, medications & alternative herbal therapiesNo ratings yet
- Breathing Freely Atropic Asthma: Transforming Atopic Bronchial Asthma into WellnessFrom EverandBreathing Freely Atropic Asthma: Transforming Atopic Bronchial Asthma into WellnessNo ratings yet
- Growing Thriving TrachDocument138 pagesGrowing Thriving TrachShaina Fe RabaneraNo ratings yet
- Archive of SID: The Most Well-Known Health Literacy Questionnaires: A Narrative ReviewDocument10 pagesArchive of SID: The Most Well-Known Health Literacy Questionnaires: A Narrative ReviewShaina Fe RabaneraNo ratings yet
- Reading and WritingDocument3 pagesReading and WritingShaina Fe RabaneraNo ratings yet
- Cues and Objectives Explanation of The Problem Goals and Objectives Interventions Rationale EvaluationDocument4 pagesCues and Objectives Explanation of The Problem Goals and Objectives Interventions Rationale EvaluationShaina Fe RabaneraNo ratings yet
- Coronavirus (Covid-19) : NEJM Group Follow Us Sign in Create AccountDocument28 pagesCoronavirus (Covid-19) : NEJM Group Follow Us Sign in Create AccountShaina Fe RabaneraNo ratings yet
- Factitious Disorders: Definition and Symptoms - Quiz & WorksheetDocument6 pagesFactitious Disorders: Definition and Symptoms - Quiz & WorksheetShaina Fe RabaneraNo ratings yet
- DVDGDDocument5 pagesDVDGDShaina Fe RabaneraNo ratings yet
- Reading and Writing: What's More Activity 1.3.1Document3 pagesReading and Writing: What's More Activity 1.3.1Shaina Fe RabaneraNo ratings yet
- Media and Information Literacy: ACTIVITY 1: Forget Me NotDocument5 pagesMedia and Information Literacy: ACTIVITY 1: Forget Me NotShaina Fe RabaneraNo ratings yet
- Reading and Writing: What's More Activity 1.3.1Document3 pagesReading and Writing: What's More Activity 1.3.1Shaina Fe RabaneraNo ratings yet
- Media and Information Literacy: ACTIVITY 1: Forget Me NotDocument5 pagesMedia and Information Literacy: ACTIVITY 1: Forget Me NotShaina Fe RabaneraNo ratings yet
- Tamad 3Document3 pagesTamad 3Shaina Fe RabaneraNo ratings yet
- Skip Directly To Site Contentskip Directly To Page Optionsskip Directly To ADocument10 pagesSkip Directly To Site Contentskip Directly To Page Optionsskip Directly To AShaina Fe RabaneraNo ratings yet
- Tamad 4Document3 pagesTamad 4Shaina Fe Rabanera100% (1)
- Trasnsport Processes: Heat TransferDocument4 pagesTrasnsport Processes: Heat TransferShaina Fe RabaneraNo ratings yet
- Aspirin: Assess The Overall Condition of The SkinDocument4 pagesAspirin: Assess The Overall Condition of The SkinShaina Fe RabaneraNo ratings yet
- Care PlansDocument67 pagesCare PlansShaina Fe RabaneraNo ratings yet
- The Public Health Nurse Is The Supervisor of Rural Health Midwives. Which of The Following Is A Supervisory Function of The Pubic Health Nurse?Document2 pagesThe Public Health Nurse Is The Supervisor of Rural Health Midwives. Which of The Following Is A Supervisory Function of The Pubic Health Nurse?Shaina Fe RabaneraNo ratings yet
- Experiment 7. DESIGN AND METHODOLOGYDocument1 pageExperiment 7. DESIGN AND METHODOLOGYShaina Fe RabaneraNo ratings yet
- Trasnsport Processes: Heat TransferDocument4 pagesTrasnsport Processes: Heat TransferShaina Fe RabaneraNo ratings yet
- Monitoring The Outbreak: Regulations For Disease Reporting and Control, It Has Been Clarified ThatDocument5 pagesMonitoring The Outbreak: Regulations For Disease Reporting and Control, It Has Been Clarified ThatShaina Fe RabaneraNo ratings yet
- Grade 8 Integrated Science Week 2 Lesson 2Document5 pagesGrade 8 Integrated Science Week 2 Lesson 2Balram HaroldNo ratings yet
- BT08 PDFDocument4 pagesBT08 PDFAfdhalNo ratings yet
- Introduction To Spread Spectrum CommunicationDocument7 pagesIntroduction To Spread Spectrum CommunicationAli KashiNo ratings yet
- LinkBelt 108H5Document20 pagesLinkBelt 108H5amirNo ratings yet
- Persia and The Persian Question Volume IDocument275 pagesPersia and The Persian Question Volume IhbatesNo ratings yet
- From Protista To DNADocument11 pagesFrom Protista To DNAtantalus11No ratings yet
- Diffraction GratingDocument9 pagesDiffraction GratingRajaswi BeleNo ratings yet
- Full Project ReportDocument46 pagesFull Project ReportRakeshNo ratings yet
- Query ManualDocument37 pagesQuery ManualstraNo ratings yet
- Section Q - Ventilation:: Chapter 511-6-1Document27 pagesSection Q - Ventilation:: Chapter 511-6-1Kingsley OchiengNo ratings yet
- 802.1AEbw-2013 - IEEE STD For LAN&MANs - Media Access Control (MAC) Security. Amendment 2. Extended Packet NumberingDocument67 pages802.1AEbw-2013 - IEEE STD For LAN&MANs - Media Access Control (MAC) Security. Amendment 2. Extended Packet NumberingLenina Viktoriya TeknyetovaNo ratings yet
- STEIM, Leaves+petalz PDFDocument2 pagesSTEIM, Leaves+petalz PDFFrancescoDiMaggioNo ratings yet
- Architecture Firms: CCBA DesignsDocument1 pageArchitecture Firms: CCBA DesignspallaviNo ratings yet
- PS: Patient Safety and Risk ManagementDocument5 pagesPS: Patient Safety and Risk Managementnoor88No ratings yet
- Filtration For HPLC Sample Preparation DistributorDocument24 pagesFiltration For HPLC Sample Preparation DistributorTuyết NgânNo ratings yet
- Cobol 1.0Document43 pagesCobol 1.0sarathNo ratings yet
- Philippines RegionsDocument5 pagesPhilippines RegionsKristine MercadoNo ratings yet
- Instruction SMA TripowerDocument10 pagesInstruction SMA TripowerMirea AurelNo ratings yet
- Dangase Group - Research FinalDocument59 pagesDangase Group - Research FinalGlenda PapelleroNo ratings yet
- JES Command OverviewDocument74 pagesJES Command Overviewdb manishNo ratings yet
- IELTS All 4 Tests at Méthode Barnes Anglais RecommanderDocument21 pagesIELTS All 4 Tests at Méthode Barnes Anglais Recommanderbarnes method books internationalNo ratings yet
- Passive VoiceDocument2 pagesPassive Voicenguyen hong phuong63% (19)
- Panasonic hc-vx870 hc-vx878 hc-v770 hc-v777 Series SMDocument71 pagesPanasonic hc-vx870 hc-vx878 hc-v770 hc-v777 Series SMhector mirandaNo ratings yet
- Kilmarnock To ArdrossanDocument2 pagesKilmarnock To Ardrossanadamdon89100% (1)
- MR SecGH Grp1 LeverAyushDocument12 pagesMR SecGH Grp1 LeverAyushSoumya HalderNo ratings yet
- Lesson Plan Ds 8603Document7 pagesLesson Plan Ds 8603sramalingam288953No ratings yet