
Date: Sept 9, 2020 Time Visit Started: 2:25 PM Time Visit Ended: 3:52 PM Home Visit/ Office Visit/alternate Site
Date: Sept 9, 2020 Time Visit Started: 2:25 PM Time Visit Ended: 3:52 PM Home Visit/ Office Visit/alternate Site
You might also like
- Maternal Newborn Case Study Approach ToquestionsDocument83 pagesMaternal Newborn Case Study Approach ToquestionsVin Lorenzo Campbell67% (6)
- Maternal Newborn PDFDocument83 pagesMaternal Newborn PDFIya Katz33% (3)
- Maternity Case 3: Brenda Patton (Core) : Guided Reflection QuestionsDocument3 pagesMaternity Case 3: Brenda Patton (Core) : Guided Reflection QuestionsDai Nguyen100% (1)
- Outline For Spanking ChildDocument3 pagesOutline For Spanking Childstd_1186960% (10)
- Obstetrics and Gynecology NOTESDocument73 pagesObstetrics and Gynecology NOTESAwais Awais100% (6)
- ANC OB and GYN HISTORY Taking SampleDocument43 pagesANC OB and GYN HISTORY Taking SampleGebremichael Reta100% (3)
- Guiding Young ChildrenDocument4 pagesGuiding Young ChildrenAljon MalotNo ratings yet
- P Mssprenatalscreeningguide 1Document3 pagesP Mssprenatalscreeningguide 1Dn CredibleNo ratings yet
- Questions: Prenatal Screening GuideDocument4 pagesQuestions: Prenatal Screening GuideMaria HyacinthNo ratings yet
- P MsspostpregnancyscreeningguideDocument3 pagesP MsspostpregnancyscreeningguideKraztyl May BejadaNo ratings yet
- Interview SheetDocument3 pagesInterview SheetSheryhan Tahir BayleNo ratings yet
- Q'S: Demographic DataDocument2 pagesQ'S: Demographic DataHILARY MAE MARINNo ratings yet
- Pre Natal Care 2Document19 pagesPre Natal Care 2Isha Catimbang GenerilloNo ratings yet
- 2020 Prats Questionnaire EnglishDocument11 pages2020 Prats Questionnaire Englishapi-667949060No ratings yet
- OB/GYN Care Visit: Personal InformationDocument7 pagesOB/GYN Care Visit: Personal InformationsinarNo ratings yet
- Mom AssessmentDocument13 pagesMom Assessmentapi-508446364No ratings yet
- Obstetrics Gynaecology ReportDocument2 pagesObstetrics Gynaecology ReportBEYOND ZFSNo ratings yet
- Prenatal CareDocument9 pagesPrenatal CareAlyssa HigumNo ratings yet
- Maternal Assessment: History TakingDocument18 pagesMaternal Assessment: History TakingSirisha ChelvaNo ratings yet
- Phase5 StandardQuestionsDocument37 pagesPhase5 StandardQuestionsPatricia FernandesNo ratings yet
- 4 - Preterm BirthDocument13 pages4 - Preterm Birthsaeed hasan saeedNo ratings yet
- Full Med QuestionnaireDocument3 pagesFull Med QuestionnaireGordana ManasievaNo ratings yet
- Phase 9 Core Questionaire 508Document14 pagesPhase 9 Core Questionaire 508Bunda Happy 2023No ratings yet
- Pregnancy Weeks 34 42 EnglishDocument20 pagesPregnancy Weeks 34 42 EnglishPooja YadavNo ratings yet
- High Blood Pressure: UltrasoundDocument7 pagesHigh Blood Pressure: UltrasoundMaria Delia SalvadoNo ratings yet
- On Exam After BirthDocument4 pagesOn Exam After Birthstephen X-SILVERNo ratings yet
- Screenshot 2022-06-28 at 9.33.56 AM PDFDocument1 pageScreenshot 2022-06-28 at 9.33.56 AM PDFhelen S. DeeNo ratings yet
- Parmed Xpreg PDFDocument4 pagesParmed Xpreg PDFriddhiNo ratings yet
- Prenatal Questionnaire: General InformationDocument6 pagesPrenatal Questionnaire: General InformationChristine HernandezNo ratings yet
- Review of Antenatal Care: EsmoeDocument84 pagesReview of Antenatal Care: EsmoeLana LocoNo ratings yet
- OBSTETRIC History Template V4Document2 pagesOBSTETRIC History Template V4Shan PatelNo ratings yet
- Antenatal Self Referral Form Whipps Cross HospitalDocument2 pagesAntenatal Self Referral Form Whipps Cross Hospitalirinelstanciu0No ratings yet
- PregnancyDocument32 pagesPregnancyAllyah Anthonette FerweloNo ratings yet
- Pre Employment Health AssessmentDocument7 pagesPre Employment Health AssessmentMP13No ratings yet
- WPH OB Appointment Schedule Flyer ENGLISHDocument2 pagesWPH OB Appointment Schedule Flyer ENGLISHIsabela BauchNo ratings yet
- Antenatal 1Document2 pagesAntenatal 1jonaNo ratings yet
- Pre Natal Care. Outline 2Document4 pagesPre Natal Care. Outline 2daniloallauigan19No ratings yet
- Simulated-Learning Case StudyDocument6 pagesSimulated-Learning Case StudyChristopher jan LegaspiNo ratings yet
- 5.sick Child Recording Form Hiv Adap 2014Document2 pages5.sick Child Recording Form Hiv Adap 2014Umar Faruk LawanNo ratings yet
- OB HN Week 1Document21 pagesOB HN Week 1Hanna Bianca TaguinodNo ratings yet
- 2023.aug.29 IMCI FormDocument5 pages2023.aug.29 IMCI FormHanna Fritch LariosaNo ratings yet
- 6 HTTP Familydoctor Org Familydoctor en Health Tools Search by Symptom Breast Problems Women HTMLDocument4 pages6 HTTP Familydoctor Org Familydoctor en Health Tools Search by Symptom Breast Problems Women HTMLYasaan ChaudharyNo ratings yet
- Picture To Be Added Here: Pregnancy Health and Antenatal TestingDocument2 pagesPicture To Be Added Here: Pregnancy Health and Antenatal TestingYanni YangNo ratings yet
- Sinovac - April 15 2021 (Health Declaration Screening Form)Document1 pageSinovac - April 15 2021 (Health Declaration Screening Form)Karen BalanayNo ratings yet
- Obstetrics and Gynaecology ReportDocument4 pagesObstetrics and Gynaecology ReportcachoydapNo ratings yet
- Pregnancy OptionsDocument1 pagePregnancy Optionsapi-581534854No ratings yet
- Signs of PregnancyDocument4 pagesSigns of Pregnancybreanna zyreNo ratings yet
- WW.05.02 Obstetrical Triage and AssessmentDocument7 pagesWW.05.02 Obstetrical Triage and AssessmentFransiscus Braveno RapaNo ratings yet
- Sinovac - March 5 2021 (Health Declaration Screening Form)Document1 pageSinovac - March 5 2021 (Health Declaration Screening Form)IT DepartmentNo ratings yet
- Antepartum Care AssignmentDocument3 pagesAntepartum Care AssignmentMattNo ratings yet
- Bishop's ScoreDocument2 pagesBishop's ScoreAndy WijayaNo ratings yet
- TB Ra & Ss Fillable Pace 2Document1 pageTB Ra & Ss Fillable Pace 2Joseph ThomasNo ratings yet
- Case Write Up 1 ANCDocument5 pagesCase Write Up 1 ANCfafa dejanNo ratings yet
- Your Antenatal Care - NHS PDFDocument1 pageYour Antenatal Care - NHS PDFS SNo ratings yet
- Care of The Mother and The Fetus During The Perinatal PeriodDocument22 pagesCare of The Mother and The Fetus During The Perinatal PeriodRoshin Tejero100% (1)
- Prenatal CareDocument5 pagesPrenatal CareJoshua AysonNo ratings yet
- Materi Dua Bhasa InggrisDocument15 pagesMateri Dua Bhasa InggrisNeliserNo ratings yet
- PP Mother AssessmentDocument10 pagesPP Mother Assessmentapi-455745761100% (1)
- Askeb Persalinan 5 MayuDocument13 pagesAskeb Persalinan 5 Mayugek ayuNo ratings yet
- Take Charge of Your Fertility: A Step by Step Guide to Making Babies, Including Getting Pregnant Naturally, Preventing Miscarriage and Improving Your Chances in IVFFrom EverandTake Charge of Your Fertility: A Step by Step Guide to Making Babies, Including Getting Pregnant Naturally, Preventing Miscarriage and Improving Your Chances in IVFRating: 3 out of 5 stars3/5 (1)
- Nursing Disaster1stDocument11 pagesNursing Disaster1stArlyn MarcelinoNo ratings yet
- Quality AssuranceDocument16 pagesQuality AssuranceArlyn MarcelinoNo ratings yet
- Rle or Cases FormatDocument4 pagesRle or Cases FormatArlyn MarcelinoNo ratings yet
- RLE DR CASES MarcelinoDocument8 pagesRLE DR CASES MarcelinoArlyn MarcelinoNo ratings yet
- NCMB418 Pet 2223Document2 pagesNCMB418 Pet 2223Arlyn MarcelinoNo ratings yet
- Updated Rubrics 2023 PDFDocument6 pagesUpdated Rubrics 2023 PDFArlyn MarcelinoNo ratings yet
- Week 8 CU 7 DN-M2-CU7 School Mitigation and Preparedness, Evaluation-2 - 1460360581 PDFDocument9 pagesWeek 8 CU 7 DN-M2-CU7 School Mitigation and Preparedness, Evaluation-2 - 1460360581 PDFArlyn MarcelinoNo ratings yet
- Pediatric NursingDocument291 pagesPediatric NursingArlyn MarcelinoNo ratings yet
- Propranolol, Prophylactic Warfarin, Low Molecular Weight Heparin (LMWH), Furosemide, AntibioticsDocument8 pagesPropranolol, Prophylactic Warfarin, Low Molecular Weight Heparin (LMWH), Furosemide, AntibioticsArlyn MarcelinoNo ratings yet
- Bachelor of Science in Nursing: Community Health Nursing: Course Module Course Unit WeekDocument8 pagesBachelor of Science in Nursing: Community Health Nursing: Course Module Course Unit WeekArlyn MarcelinoNo ratings yet
- FamDocument1 pageFamArlyn MarcelinoNo ratings yet
- Module 13 & 14: Broadening Compassion: Our Lady of Fatima University Veritas Et MisericordiaDocument3 pagesModule 13 & 14: Broadening Compassion: Our Lady of Fatima University Veritas Et MisericordiaArlyn MarcelinoNo ratings yet
- Natural Family Planning and Fertility AwarenessDocument7 pagesNatural Family Planning and Fertility AwarenessArlyn MarcelinoNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument3 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationArlyn MarcelinoNo ratings yet
- Ebook PDF Child Development A Thematic Approach 6th Edition PDFDocument41 pagesEbook PDF Child Development A Thematic Approach 6th Edition PDFmike.casteel807100% (45)
- Maria Dalisay C. Caponpon, Man, RN, RM, BSM Member APSOM Group of TrainersDocument63 pagesMaria Dalisay C. Caponpon, Man, RN, RM, BSM Member APSOM Group of Trainersjamaica cabrigaNo ratings yet
- Ilmp Grade 8Document22 pagesIlmp Grade 8liezelNo ratings yet
- Agresivnost Kod Djece I AdolescenataDocument12 pagesAgresivnost Kod Djece I Adolescenatamatea tijaNo ratings yet
- Questions Answers About Child Sexual AbuseDocument6 pagesQuestions Answers About Child Sexual AbusealandNo ratings yet
- Pepsi ScreeningDocument13 pagesPepsi Screeningapi-509422938No ratings yet
- Entrevista Baseada Nas Rotinas - Modelo InglêsDocument12 pagesEntrevista Baseada Nas Rotinas - Modelo InglêsLiana Amorim SantanaNo ratings yet
- Determinan SC Djamil Cover Dan AbstrakDocument3 pagesDeterminan SC Djamil Cover Dan AbstrakPPDS OBGYN UNAND JULI 2023No ratings yet
- Summary of Results: Early Childhood Development (Ecd) CHECKLIST S.Y. 2020 - 2021Document4 pagesSummary of Results: Early Childhood Development (Ecd) CHECKLIST S.Y. 2020 - 2021Mary Rose VargasNo ratings yet
- CBSE Class 3 EVS Worksheet PDFDocument3 pagesCBSE Class 3 EVS Worksheet PDFSheldon CooperNo ratings yet
- Growth and Development Theory - ARNOLD GESELL (1880 - 1961) - SchoolWorkHelperDocument3 pagesGrowth and Development Theory - ARNOLD GESELL (1880 - 1961) - SchoolWorkHelperMraghhh AghhhNo ratings yet
- Ex-21 Worksheet (Blood Relations)Document2 pagesEx-21 Worksheet (Blood Relations)RishikaNo ratings yet
- Publication NPDAF Children BrochureDocument3 pagesPublication NPDAF Children BrochureVictoria Hargan100% (1)
- 10 Early Adulthood Young AdulthoodDocument35 pages10 Early Adulthood Young AdulthoodgenalinangNo ratings yet
- The Only Exception: Teenage Pregnancy in The Philippines: January 2018Document29 pagesThe Only Exception: Teenage Pregnancy in The Philippines: January 2018Abby YambaoNo ratings yet
- Racheal Crane Babyloss Awareness Case Studies 20th March 2023Document1 pageRacheal Crane Babyloss Awareness Case Studies 20th March 2023api-286232866No ratings yet
- Caars Self (S) Int.Document7 pagesCaars Self (S) Int.Farida LarryNo ratings yet
- Philippine National Police Kiangan Quarantine Facility: Health Service General HospitalDocument6 pagesPhilippine National Police Kiangan Quarantine Facility: Health Service General HospitalNHQ Quarantine FacilityNo ratings yet
- Module 3 - Skills, Tasks, and Challenges Appropriate For Middle and Late AdolescenceDocument41 pagesModule 3 - Skills, Tasks, and Challenges Appropriate For Middle and Late AdolescenceLIZALYNN MAMBIARNo ratings yet
- Lyubomirsky S Sheldon and Schkade 2005 Pursuing Happiness PDFDocument21 pagesLyubomirsky S Sheldon and Schkade 2005 Pursuing Happiness PDFChristie AnggeloNo ratings yet
- Manuskrip LusitasariDocument19 pagesManuskrip Lusitasaricb6wnzfqdrNo ratings yet
- Developing Stages in Middle & Late AdolescenceDocument16 pagesDeveloping Stages in Middle & Late AdolescenceJitz BugoyNo ratings yet
- My Social Studies SBADocument10 pagesMy Social Studies SBACamaya RumbleNo ratings yet
- Breastfeeding InfoDocument2 pagesBreastfeeding InfoThe Vancouver SunNo ratings yet
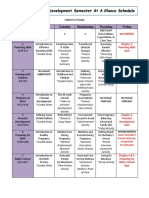
- Child Development Semester at GlanceDocument3 pagesChild Development Semester at Glanceapi-326704239No ratings yet
- Explorative Essay Rough DraftDocument6 pagesExplorative Essay Rough Draftapi-238508557No ratings yet
- Narcissism in Parental Alienation - Clarifying Examples - Psychology Today PrintedDocument7 pagesNarcissism in Parental Alienation - Clarifying Examples - Psychology Today PrintedFamily Court-CorruptionNo ratings yet
- The Child and Adolescent Learners and Learning PrinciplesDocument8 pagesThe Child and Adolescent Learners and Learning PrinciplesMarny Pangandian MasiglatNo ratings yet






































































































Download as docx, pdf, or txt
You might also like
- Maternal Newborn Case Study Approach ToquestionsDocument83 pagesMaternal Newborn Case Study Approach ToquestionsVin Lorenzo Campbell67% (6)
- Maternal Newborn PDFDocument83 pagesMaternal Newborn PDFIya Katz33% (3)
- Maternity Case 3: Brenda Patton (Core) : Guided Reflection QuestionsDocument3 pagesMaternity Case 3: Brenda Patton (Core) : Guided Reflection QuestionsDai Nguyen100% (1)
- Outline For Spanking ChildDocument3 pagesOutline For Spanking Childstd_1186960% (10)
- Obstetrics and Gynecology NOTESDocument73 pagesObstetrics and Gynecology NOTESAwais Awais100% (6)
- ANC OB and GYN HISTORY Taking SampleDocument43 pagesANC OB and GYN HISTORY Taking SampleGebremichael Reta100% (3)
- Guiding Young ChildrenDocument4 pagesGuiding Young ChildrenAljon MalotNo ratings yet
- P Mssprenatalscreeningguide 1Document3 pagesP Mssprenatalscreeningguide 1Dn CredibleNo ratings yet
- Questions: Prenatal Screening GuideDocument4 pagesQuestions: Prenatal Screening GuideMaria HyacinthNo ratings yet
- P MsspostpregnancyscreeningguideDocument3 pagesP MsspostpregnancyscreeningguideKraztyl May BejadaNo ratings yet
- Interview SheetDocument3 pagesInterview SheetSheryhan Tahir BayleNo ratings yet
- Q'S: Demographic DataDocument2 pagesQ'S: Demographic DataHILARY MAE MARINNo ratings yet
- Pre Natal Care 2Document19 pagesPre Natal Care 2Isha Catimbang GenerilloNo ratings yet
- 2020 Prats Questionnaire EnglishDocument11 pages2020 Prats Questionnaire Englishapi-667949060No ratings yet
- OB/GYN Care Visit: Personal InformationDocument7 pagesOB/GYN Care Visit: Personal InformationsinarNo ratings yet
- Mom AssessmentDocument13 pagesMom Assessmentapi-508446364No ratings yet
- Obstetrics Gynaecology ReportDocument2 pagesObstetrics Gynaecology ReportBEYOND ZFSNo ratings yet
- Prenatal CareDocument9 pagesPrenatal CareAlyssa HigumNo ratings yet
- Maternal Assessment: History TakingDocument18 pagesMaternal Assessment: History TakingSirisha ChelvaNo ratings yet
- Phase5 StandardQuestionsDocument37 pagesPhase5 StandardQuestionsPatricia FernandesNo ratings yet
- 4 - Preterm BirthDocument13 pages4 - Preterm Birthsaeed hasan saeedNo ratings yet
- Full Med QuestionnaireDocument3 pagesFull Med QuestionnaireGordana ManasievaNo ratings yet
- Phase 9 Core Questionaire 508Document14 pagesPhase 9 Core Questionaire 508Bunda Happy 2023No ratings yet
- Pregnancy Weeks 34 42 EnglishDocument20 pagesPregnancy Weeks 34 42 EnglishPooja YadavNo ratings yet
- High Blood Pressure: UltrasoundDocument7 pagesHigh Blood Pressure: UltrasoundMaria Delia SalvadoNo ratings yet
- On Exam After BirthDocument4 pagesOn Exam After Birthstephen X-SILVERNo ratings yet
- Screenshot 2022-06-28 at 9.33.56 AM PDFDocument1 pageScreenshot 2022-06-28 at 9.33.56 AM PDFhelen S. DeeNo ratings yet
- Parmed Xpreg PDFDocument4 pagesParmed Xpreg PDFriddhiNo ratings yet
- Prenatal Questionnaire: General InformationDocument6 pagesPrenatal Questionnaire: General InformationChristine HernandezNo ratings yet
- Review of Antenatal Care: EsmoeDocument84 pagesReview of Antenatal Care: EsmoeLana LocoNo ratings yet
- OBSTETRIC History Template V4Document2 pagesOBSTETRIC History Template V4Shan PatelNo ratings yet
- Antenatal Self Referral Form Whipps Cross HospitalDocument2 pagesAntenatal Self Referral Form Whipps Cross Hospitalirinelstanciu0No ratings yet
- PregnancyDocument32 pagesPregnancyAllyah Anthonette FerweloNo ratings yet
- Pre Employment Health AssessmentDocument7 pagesPre Employment Health AssessmentMP13No ratings yet
- WPH OB Appointment Schedule Flyer ENGLISHDocument2 pagesWPH OB Appointment Schedule Flyer ENGLISHIsabela BauchNo ratings yet
- Antenatal 1Document2 pagesAntenatal 1jonaNo ratings yet
- Pre Natal Care. Outline 2Document4 pagesPre Natal Care. Outline 2daniloallauigan19No ratings yet
- Simulated-Learning Case StudyDocument6 pagesSimulated-Learning Case StudyChristopher jan LegaspiNo ratings yet
- 5.sick Child Recording Form Hiv Adap 2014Document2 pages5.sick Child Recording Form Hiv Adap 2014Umar Faruk LawanNo ratings yet
- OB HN Week 1Document21 pagesOB HN Week 1Hanna Bianca TaguinodNo ratings yet
- 2023.aug.29 IMCI FormDocument5 pages2023.aug.29 IMCI FormHanna Fritch LariosaNo ratings yet
- 6 HTTP Familydoctor Org Familydoctor en Health Tools Search by Symptom Breast Problems Women HTMLDocument4 pages6 HTTP Familydoctor Org Familydoctor en Health Tools Search by Symptom Breast Problems Women HTMLYasaan ChaudharyNo ratings yet
- Picture To Be Added Here: Pregnancy Health and Antenatal TestingDocument2 pagesPicture To Be Added Here: Pregnancy Health and Antenatal TestingYanni YangNo ratings yet
- Sinovac - April 15 2021 (Health Declaration Screening Form)Document1 pageSinovac - April 15 2021 (Health Declaration Screening Form)Karen BalanayNo ratings yet
- Obstetrics and Gynaecology ReportDocument4 pagesObstetrics and Gynaecology ReportcachoydapNo ratings yet
- Pregnancy OptionsDocument1 pagePregnancy Optionsapi-581534854No ratings yet
- Signs of PregnancyDocument4 pagesSigns of Pregnancybreanna zyreNo ratings yet
- WW.05.02 Obstetrical Triage and AssessmentDocument7 pagesWW.05.02 Obstetrical Triage and AssessmentFransiscus Braveno RapaNo ratings yet
- Sinovac - March 5 2021 (Health Declaration Screening Form)Document1 pageSinovac - March 5 2021 (Health Declaration Screening Form)IT DepartmentNo ratings yet
- Antepartum Care AssignmentDocument3 pagesAntepartum Care AssignmentMattNo ratings yet
- Bishop's ScoreDocument2 pagesBishop's ScoreAndy WijayaNo ratings yet
- TB Ra & Ss Fillable Pace 2Document1 pageTB Ra & Ss Fillable Pace 2Joseph ThomasNo ratings yet
- Case Write Up 1 ANCDocument5 pagesCase Write Up 1 ANCfafa dejanNo ratings yet
- Your Antenatal Care - NHS PDFDocument1 pageYour Antenatal Care - NHS PDFS SNo ratings yet
- Care of The Mother and The Fetus During The Perinatal PeriodDocument22 pagesCare of The Mother and The Fetus During The Perinatal PeriodRoshin Tejero100% (1)
- Prenatal CareDocument5 pagesPrenatal CareJoshua AysonNo ratings yet
- Materi Dua Bhasa InggrisDocument15 pagesMateri Dua Bhasa InggrisNeliserNo ratings yet
- PP Mother AssessmentDocument10 pagesPP Mother Assessmentapi-455745761100% (1)
- Askeb Persalinan 5 MayuDocument13 pagesAskeb Persalinan 5 Mayugek ayuNo ratings yet
- Take Charge of Your Fertility: A Step by Step Guide to Making Babies, Including Getting Pregnant Naturally, Preventing Miscarriage and Improving Your Chances in IVFFrom EverandTake Charge of Your Fertility: A Step by Step Guide to Making Babies, Including Getting Pregnant Naturally, Preventing Miscarriage and Improving Your Chances in IVFRating: 3 out of 5 stars3/5 (1)
- Nursing Disaster1stDocument11 pagesNursing Disaster1stArlyn MarcelinoNo ratings yet
- Quality AssuranceDocument16 pagesQuality AssuranceArlyn MarcelinoNo ratings yet
- Rle or Cases FormatDocument4 pagesRle or Cases FormatArlyn MarcelinoNo ratings yet
- RLE DR CASES MarcelinoDocument8 pagesRLE DR CASES MarcelinoArlyn MarcelinoNo ratings yet
- NCMB418 Pet 2223Document2 pagesNCMB418 Pet 2223Arlyn MarcelinoNo ratings yet
- Updated Rubrics 2023 PDFDocument6 pagesUpdated Rubrics 2023 PDFArlyn MarcelinoNo ratings yet
- Week 8 CU 7 DN-M2-CU7 School Mitigation and Preparedness, Evaluation-2 - 1460360581 PDFDocument9 pagesWeek 8 CU 7 DN-M2-CU7 School Mitigation and Preparedness, Evaluation-2 - 1460360581 PDFArlyn MarcelinoNo ratings yet
- Pediatric NursingDocument291 pagesPediatric NursingArlyn MarcelinoNo ratings yet
- Propranolol, Prophylactic Warfarin, Low Molecular Weight Heparin (LMWH), Furosemide, AntibioticsDocument8 pagesPropranolol, Prophylactic Warfarin, Low Molecular Weight Heparin (LMWH), Furosemide, AntibioticsArlyn MarcelinoNo ratings yet
- Bachelor of Science in Nursing: Community Health Nursing: Course Module Course Unit WeekDocument8 pagesBachelor of Science in Nursing: Community Health Nursing: Course Module Course Unit WeekArlyn MarcelinoNo ratings yet
- FamDocument1 pageFamArlyn MarcelinoNo ratings yet
- Module 13 & 14: Broadening Compassion: Our Lady of Fatima University Veritas Et MisericordiaDocument3 pagesModule 13 & 14: Broadening Compassion: Our Lady of Fatima University Veritas Et MisericordiaArlyn MarcelinoNo ratings yet
- Natural Family Planning and Fertility AwarenessDocument7 pagesNatural Family Planning and Fertility AwarenessArlyn MarcelinoNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument3 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationArlyn MarcelinoNo ratings yet
- Ebook PDF Child Development A Thematic Approach 6th Edition PDFDocument41 pagesEbook PDF Child Development A Thematic Approach 6th Edition PDFmike.casteel807100% (45)
- Maria Dalisay C. Caponpon, Man, RN, RM, BSM Member APSOM Group of TrainersDocument63 pagesMaria Dalisay C. Caponpon, Man, RN, RM, BSM Member APSOM Group of Trainersjamaica cabrigaNo ratings yet
- Ilmp Grade 8Document22 pagesIlmp Grade 8liezelNo ratings yet
- Agresivnost Kod Djece I AdolescenataDocument12 pagesAgresivnost Kod Djece I Adolescenatamatea tijaNo ratings yet
- Questions Answers About Child Sexual AbuseDocument6 pagesQuestions Answers About Child Sexual AbusealandNo ratings yet
- Pepsi ScreeningDocument13 pagesPepsi Screeningapi-509422938No ratings yet
- Entrevista Baseada Nas Rotinas - Modelo InglêsDocument12 pagesEntrevista Baseada Nas Rotinas - Modelo InglêsLiana Amorim SantanaNo ratings yet
- Determinan SC Djamil Cover Dan AbstrakDocument3 pagesDeterminan SC Djamil Cover Dan AbstrakPPDS OBGYN UNAND JULI 2023No ratings yet
- Summary of Results: Early Childhood Development (Ecd) CHECKLIST S.Y. 2020 - 2021Document4 pagesSummary of Results: Early Childhood Development (Ecd) CHECKLIST S.Y. 2020 - 2021Mary Rose VargasNo ratings yet
- CBSE Class 3 EVS Worksheet PDFDocument3 pagesCBSE Class 3 EVS Worksheet PDFSheldon CooperNo ratings yet
- Growth and Development Theory - ARNOLD GESELL (1880 - 1961) - SchoolWorkHelperDocument3 pagesGrowth and Development Theory - ARNOLD GESELL (1880 - 1961) - SchoolWorkHelperMraghhh AghhhNo ratings yet
- Ex-21 Worksheet (Blood Relations)Document2 pagesEx-21 Worksheet (Blood Relations)RishikaNo ratings yet
- Publication NPDAF Children BrochureDocument3 pagesPublication NPDAF Children BrochureVictoria Hargan100% (1)
- 10 Early Adulthood Young AdulthoodDocument35 pages10 Early Adulthood Young AdulthoodgenalinangNo ratings yet
- The Only Exception: Teenage Pregnancy in The Philippines: January 2018Document29 pagesThe Only Exception: Teenage Pregnancy in The Philippines: January 2018Abby YambaoNo ratings yet
- Racheal Crane Babyloss Awareness Case Studies 20th March 2023Document1 pageRacheal Crane Babyloss Awareness Case Studies 20th March 2023api-286232866No ratings yet
- Caars Self (S) Int.Document7 pagesCaars Self (S) Int.Farida LarryNo ratings yet
- Philippine National Police Kiangan Quarantine Facility: Health Service General HospitalDocument6 pagesPhilippine National Police Kiangan Quarantine Facility: Health Service General HospitalNHQ Quarantine FacilityNo ratings yet
- Module 3 - Skills, Tasks, and Challenges Appropriate For Middle and Late AdolescenceDocument41 pagesModule 3 - Skills, Tasks, and Challenges Appropriate For Middle and Late AdolescenceLIZALYNN MAMBIARNo ratings yet
- Lyubomirsky S Sheldon and Schkade 2005 Pursuing Happiness PDFDocument21 pagesLyubomirsky S Sheldon and Schkade 2005 Pursuing Happiness PDFChristie AnggeloNo ratings yet
- Manuskrip LusitasariDocument19 pagesManuskrip Lusitasaricb6wnzfqdrNo ratings yet
- Developing Stages in Middle & Late AdolescenceDocument16 pagesDeveloping Stages in Middle & Late AdolescenceJitz BugoyNo ratings yet
- My Social Studies SBADocument10 pagesMy Social Studies SBACamaya RumbleNo ratings yet
- Breastfeeding InfoDocument2 pagesBreastfeeding InfoThe Vancouver SunNo ratings yet
- Child Development Semester at GlanceDocument3 pagesChild Development Semester at Glanceapi-326704239No ratings yet
- Explorative Essay Rough DraftDocument6 pagesExplorative Essay Rough Draftapi-238508557No ratings yet
- Narcissism in Parental Alienation - Clarifying Examples - Psychology Today PrintedDocument7 pagesNarcissism in Parental Alienation - Clarifying Examples - Psychology Today PrintedFamily Court-CorruptionNo ratings yet
- The Child and Adolescent Learners and Learning PrinciplesDocument8 pagesThe Child and Adolescent Learners and Learning PrinciplesMarny Pangandian MasiglatNo ratings yet